
Abstract
Abstract
Background:
To evaluate the feasibility, clinical and perioperative outcomes of laparoscopic retroperitoneal lymph node dissection (L-RPLND) in the management of patients with germ cell tumors (GCT) and residual post-chemotherapy mass.
Methods:
We report our experience of 25 patients treated with L-RPLND between 2008 and 2015. All 25 patients were diagnosed with GCT by primary pathological evaluation of the specimens after orchiectomy. All patients received cisplatin-based chemotherapy. The technique consisted of L-RPLND excision of the residual mass using unilateral template dissection. We assessed perioperative data and histological findings.
Results:
Surgery was successfully completed in 24 (96%) patients, 1 patient required an open surgery due to intense adhesions of the mass to the inferior vena cava. Mean operation time was 213 minutes. Mean blood loss was 260 mL. Postoperative complications were upper limb osteomuscular pain in 2 patients and chylous ascites in 1 patient. Mean postoperative hospital stay was 2 days. The median residual mass diameter was 3.3 cm (range 1.1–6.6 cm). Histopathological findings were necrotic tissue in 9 patients, teratoma in 9 patients, viable tumor in 6 patients, and Castleman disease in 1 patient. The median follow-up was 30 months. Normal antegrade ejaculation was preserved in all patients.
Conclusions:
Laparoscopic postchemotherapy RPLND is a feasible, safe, and highly oncologically efficient procedure, which has the benefits of minimally invasive surgery.
Introduction
T
RPLND after chemotherapy is indicated if there is incomplete tumor remission in the retroperitoneum. 2 In these cases, open RPLND is often performed and represents a widely accepted diagnosis and treatment option for patients with germ cell tumors (GCTs). Among patients with postchemotherapy residual retroperitoneal masses treated with RPLND for testicular cancer, ∼40% have necrosis, 40% present teratoma, and 20% have a viable tumor in the resected mass. 3
RPLND is a challenging procedure, as fibrosis hinders tissue dissection and is associated with prolonged surgery time and overall complication rate of 20.7%. 4 Open RPLND is associated with significant morbidity in terms of length of hospital stay and recovery, as it involves large incisions in predominantly young patients, chylous ascites, prolonged ileus, postoperative pain, and retrograde ejaculation. To overcome these problems, laparoscopic RPLND (L-RPLND) has evolved since 1992 5 and gained popularity, because it offered a promising approach. The procedure is technically feasible, especially for unilateral template dissection, yet lacks the objective evidence of long-term oncological equivalence with open surgery.
We report our experience using L-RPLND after chemotherapy in 25 patients with stage II GCT. Our objective was to evaluate the feasibility and clinical and perioperative outcomes of this technique.
Materials and Methods
We performed retrospective analysis of data retrieved from medical records of 25 patients treated with L-RPLND for residual testicular tumor masses after chemotherapy at the Hospital de Câncer de Barretos between January 2008 and January 2015. Only records with complete data were considered.
Tumor stage was determined by the nodal diameter measured on computed tomography (CT) of the abdomen and chest, and levels of serum tumor markers: α-fetoprotein (AFP), human chorionic β-gonadotropin (β-HCG), and lactic dehydrogenase (LDH). The patients received cisplatin-based chemotherapy before L-RPLND, according to the tumor stage and prognosis, until tumor markers were negative. Patients with residual retroperitoneal masses larger than 1 cm on CT and normal tumor markers were selected for L-RPLND. Patients with postchemotherapy voluminous masses (large tumors with compression of the vena cava, aorta, or renal vessels) were not considered for laparoscopy. The surgical technique for RPLND (open or laparoscopic) was defined individually according to the size and location of the tumor.
Surgical complications were scored according to the Clavien classification, updated in 2004. 6
The patients were followed up every 3 months during the first 3 years, every 6 months until completion of the fifth year, and annually after this period. Monitoring included physical examination, blood count, and serum biochemistry, including AFP, β-HCG, and LDH, and imaging examinations (CT or chest X-ray combined with abdominal ultrasound). An urologist evaluated the rate of antegrade ejaculation.
The ethics committee approved this study under the number 984/2015 on September 10, 2015. The study was designed according to STROBE (Strengthening the Reporting of Observational Studies in Epidemiology).
Surgical technique
The patients received a low-fat diet for 2 weeks before and 2 weeks after the surgery and a restricted liquid diet the day before surgery, without solutions for bowel preparation.
The patients were placed in a 70° lateral position and ports were placed as shown in Figure 1, using a transperitoneal approach.
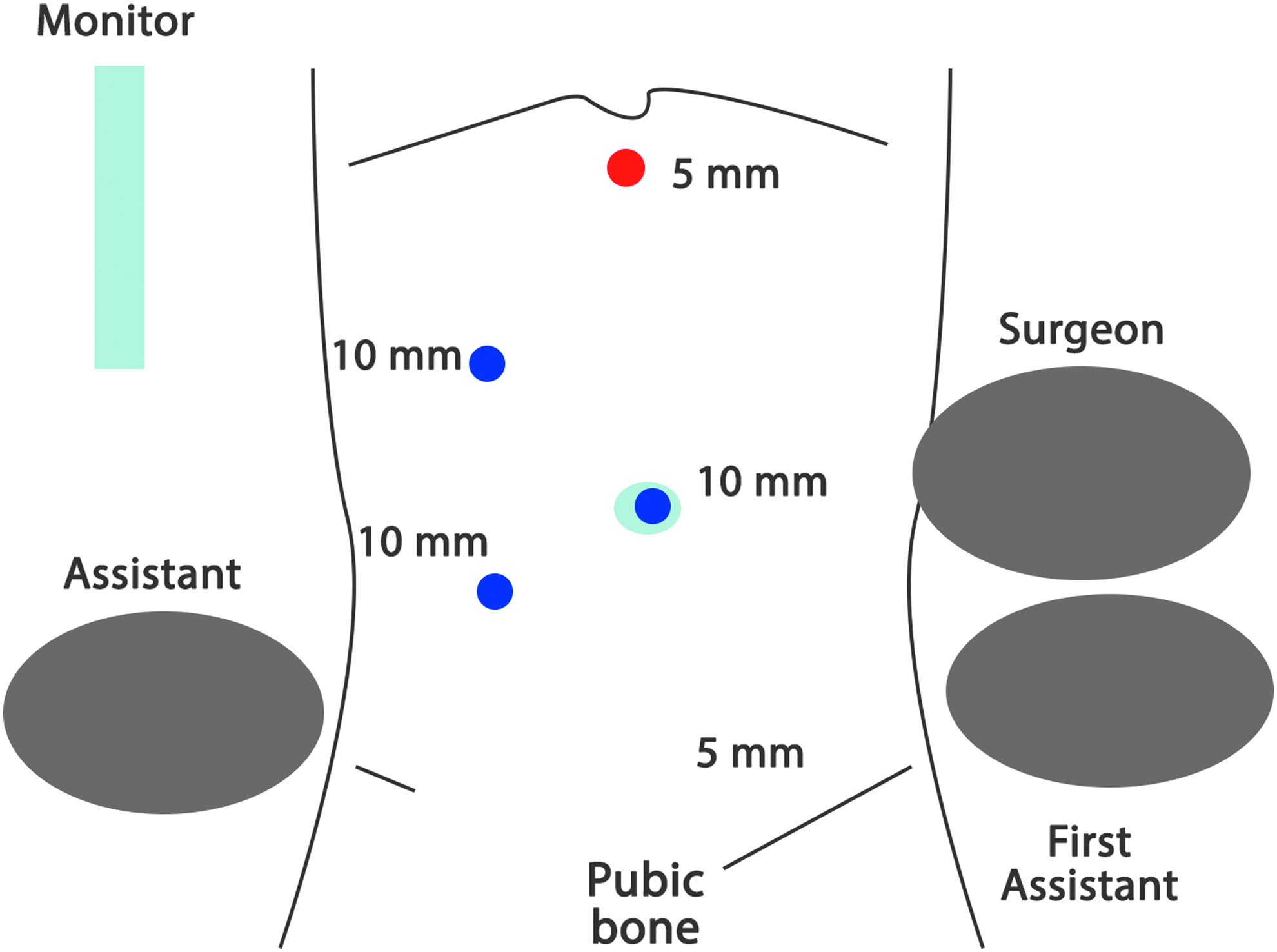
Positioning of team members and laparoscopic ports for right-sided retroperitoneal lymph node dissection.
Modified L-RPLND similar to open (conventional) dissection was performed. 7 Dissection of right-sided tumors included paracaval, precaval, retrocaval, and interaortocaval lymph nodes, from the right renal artery to the bifurcation of the inferior vena cava and the area of the right common iliac vessels, in addition to the preaortic lymph nodes between the renal vessels and the inferior mesenteric artery. For left-sided testicular tumors, dissection included paraortic lymph nodes from the renal vessels to the aortic bifurcation and the area of the left common iliac artery, as well as the preaortic lymphatic tissue up to the inferior mesenteric artery.
Results
The mean age of the operated patients was 27.6 years (14–62). Of 25 patients, 2 (8%) presented cryptorchidism ipsilateral to the tumor. Only 2 (8%) patients were classified as American Society of Anesthesiologists (ASA) 2 according to the American Society of Anesthesiology Physical Status classification system. The remaining 23 (92%) patients were ASA 1 (Table 1).
AFP, α-fetoprotein; ASA, American Society of Anesthesiologists; β-HCG, human chorionic β-gonadotropin; LDH, lactic dehydrogenase.
L-RPLND was performed ∼4–6 weeks after chemotherapy and successfully completed in 24 (96%) patients; 1 patient (4%) required conversion to open surgery due to intense adhesion of the mass to the large vessels and risk of bleeding because of rupture of the vena cava (this case was stage IIB seminoma and an elective supraumbilical incision was performed). The mean tumor diameter after chemotherapy, estimated by CT, the mean operation time, the estimated blood loss, and the mean length of hospital are described in Table 1.
Unilateral template resection was performed in all patients. No major complications were observed, except for occasional bleeding of the lumbar vessels or vena cava, which was resolved by laparoscopy. Two patients required a correction of the inferior vena cava lesion with metallic clips and laparoscopic suture and 1 patient required the suture of the aorta. No major intraoperative complications occurred.
The overall complication rate was 12% (3 of 25 patients; Table 2). Three minor complications occurred: osteomuscular pain (related to position and without short-term sequelae) in 2 patients and chylous ascites in 1 patient. The latter was managed with a low-fat diet and drainage maintenance, and resolved after 18 days. Normal antegrade ejaculation was preserved in all patients. No hospital readmissions due to late surgery complications occurred.
CT, computed tomography.
The histopathology tests showed 9 cases of necrosis/fibrosis, 9 of teratoma, 6 of viable tumor (2 of these were associated with teratoma), and 1 of Castleman disease (Table 3). Of the 4 patients with seminoma, 1 had a viable tumor in the RPLND specimen. During the mean follow-up period of 30 months (12–36), 2 patients with viable tumors (mixed tumors, both associated with teratoma) had relapse outside of the classical retroperitoneal template. One of them had mediastinal lesion and the other local recurrence above the ipsilateral renal hilum, near the diaphragmatic pillar. Both of them received salvage chemotherapy (1 received two cycles of cisplatin, etoposide, and bleomycin [PEB], and the other received three cycles of PEB) and their diseases are under control with normal tumor marker levels.
Two of the mixed cases had associated teratoma.
Anatomopathological test (immunohistochemistry) showed Castleman hyaline vascular type disease.
Discussion
The aim of implementing laparoscopy in the treatment of testicular cancer is to improve quality of life (QoL) and reduce surgical morbidity in these patients. However, no prospective randomized studies are currently available and long-term oncological data are scarce. The main disadvantage of L-RPLND is a steep learning curve. 8 Poulakis et al. 9 reported that the length of hospital stay was shorter for patients undergoing L-RPLND, their QoL was improved, and they returned earlier to their activities than patients undergoing open RPLND. Other authors state that this difference may be less pronounced when recent series of open RPLND are considered. 10
Postchemotherapy RPLND offers benefits of both tumor staging and treatment. The presence of teratoma in the primary tumor site, negative tumor markers, and degree of tumor size reduction after chemotherapy are important predictors. 11 The presence of a viable tumor in the residual retroperitoneal mass is associated with a high recurrence rate. 12
No evidence suggested that oncological efficacy is compromised by L-RPLND. Heidenreich et al. 13 reviewed 34 articles published between 2000 and 2008 that included 800 patients and concluded that L-RPLND added precision to tumor staging and long-term survival rates were similar to those associated with open RPLND. This showed that modified templates did not affect the management of residual masses smaller than 5 cm. 13 Our study showed 2 patients who had recurrence outside of the classical template, even if bilateral dissection had been performed.
Controversy still exists regarding the extension of postchemotherapy RPLND. Some authors contend that complete bilateral resection is necessary. 14 However, the bilateral procedure is associated with high complication rates. 4 In contrast, it has been demonstrated that dissection of the unilateral template provides adequate oncological outcomes, comparable with those obtained with the bilateral procedure. 15
Aufderklamm et al. 16 compared L-RPLND with unilateral and bilateral templates and showed that, in masses smaller than 5 cm, a modified template did not compromise the oncological outcome but reduced treatment-associated morbidity. The resection area was then delineated according to Weissbach and Boedefeld models. 7
In our cohort, we decided to perform unilateral template due to small retroperitoneal masses. However, the bilateral dissection is feasible using the same full-flank position. The feasibility of a bilateral approach using the same patient positioning is important, given that in one report in the literature, among 50 patients with residual disease after chemotherapy were treated with RPLND using the bilateral template technique the rate of contralateral right-sided tumor progression was 20%, whereas left-sided tumors progressed as expected. Another report found an incidence of disease outside the template of approximately 20%. 17 In right-sided resections, the inclusion of paraortic, preaortic, and right common iliac lymph nodes reduced the incidence of the disease outside the template to 2%. In left-sided tumors, inclusion of interaortocaval, precaval, paracaval, and left common iliac lymph nodes decreased the incidence of disease outside the template to 3%. 17
Postchemotherapy RPLND is associated with overall morbidity and mortality rates of 20.7% and 0.8%, respectively, according to the Indiana Group. 4 Other studies have determined a complication rate of 35% for postchemotherapy open RPLND. 18
In their literature review, Heidenreich et al. 13 obtained an overall complication rate of 15.6% (9.4–25.7), including retrograde ejaculation and reoperation rates of 2% (0–5) and 1.7% (0–6), respectively. They found a significantly longer operation time (204 versus 186 minutes) in the L-RPLND group (n = 499) than in the open LNDRP group (n = 524). However, the complication rate (15.6% versus 33%), reoperation rate (1.4% versus 6.6%), and length of hospital stay (3.3 versus 6.6 days) all favored L-RPLND.
Abdel-Aziz et al., 19 in a series of 28 patients, reported that L-RPLND was associated with less blood loss and shorter hospital stay, when compared with the open technique, but less lymph nodes were removed (17 versus 33). No significant difference was noted in operation time (313 minutes in L-RPLND versus 284 minutes in open RPLND). In our study, operation time, blood loss, and length of hospital stay were similar to these results.
Janetschek et al. 20 reported a lower morbidity in 24 patients with stage IIB nonseminomatous testicular carcinoma; the overall complication rate was 25% (5 patients had chylous ascites and 1 patient had small lymphocele).
Anejaculation is the most common long-term morbidity of RPLND. Nerve-sparing techniques have been developed to spare sympathetic postganglionic nerve fibers and some authors have proposed concepts of modified dissection templates. 21 The rate of antegrade ejaculation obtained in our sample of 25 patients was 100%, similar to that reported in open series, 22 probably because of the use of a unilateral template.
The need for conversion to open surgery has been decreasing over the years. Winfield 23 reported 4 cases of postchemotherapy L-RPLND for stage II nonseminomatous testicular tumors. Three patients required conversion to open surgery because of vascular lesions. Rassweiler et al. 24 reported postchemotherapy L-RPLND in 9 patients with stages IIB (n = 2) and IIC (n = 7) testicular carcinoma; the procedure was successfully completed in 2 patients (22%) because of an intense desmoplastic reaction. By contrast, Janetschek et al. did not report any case of conversion in their series. 20 The laparoscopic approach became safer and more standardized with the experience acquired over time.
We did not find an increase in perioperative complications in postchemotherapy patients, although desmoplasia hindered dissection. We used a strategy to minimize vascular lesions, which involved the addition of gauze to the tip of the laparoscopic clamp to separate the tumor tissue from the large vessels. In our sample, only 3 patients (12%) had complications, all without short-term complications. One case needed conversion to open surgery due to the desmoplastic reaction.
In 2004, Tobias-Machado et al. 25 described for the first time the “hand-assisted” technique in L-RPLND for nonseminomatous testicular tumors. It is a feasible method to prevent conversion to open surgery by using a tamponade of the potential vascular lesion, thus reducing blood loss during surgery. This would be an intermediary approach to conversion and allow vascular repair in the case of bleeding. However, “hand-assisted” laparoscopic surgery also requires a learning curve, because the presence of the assistant's hand in the field may help or disturb an experienced surgeon. Furthermore, this procedure should only be performed by surgeons trained in laparoscopic suture.
In their series update, Janetschek et al. 8 confirmed the viability and low morbidity of postchemotherapy L-RPLND, especially in patients with solitary or unilateral nodules. Although L-RPLND is technically feasible for stage IIC tumors, the risk of contralateral progression associated with tumor size was too elevated for unilateral dissection by laparoscopy to be recommended. Our study confirmed the viability of L-RPLND for postchemotherapy residual masses based on the results of operation time and conversion, blood loss, and complication rates.
The first report on robot-assisted RPLND (RA-RPLND) was published in 2006, by Davol.17,26 The largest published series of RA-RPLND included 18 patients of the Mayo Clinic Arizona and 8 of these procedures were performed after chemotherapy. 27 RA-RPLND was completed in 15 patients. Three cases needed conversion to open technique due to robot malfunctioning, poor exposure, and bleeding. The mean operation time was 329 minutes; mean blood loss, 103 mL; and mean length of hospital stay, 2.4 days. No major complications occurred (Clavien III). The rate of minor complications was 17%. The mean number of lymph nodes removed by RA-RPLND was 22, of which 18 (44%) were positive (5 patients had postchemotherapy RA-RPLND and 3 had primary RA-RPLND). Antegrade ejaculation was preserved in 91% of the patients receiving nerve-sparing surgery. Primary RPLND patients benefited from shorter operation times than postchemotherapy RPLND patients, but no differences were reported in transfusion and complication rates, length of hospital stay, or number of resected lymph nodes. Although the report by Cheney et al. was limited by its retrospective nature, it showed that this procedure can be safely performed with the help of a robot in both primary and postchemotherapy settings. 27
A recent study comparing 16 patients treated using RA-RPLND with 21 patients undergoing L-RPLND, with dissection of unilateral templates without previous chemotherapy, did not find differences in perioperative outcomes. 29
Literature is limited by the small number of series published and of patients included in these series.
To achieve a satisfactory oncological outcome, the patients must be treated in centers experienced in postchemotherapy RPLND. Otherwise, the morbidity associated with this procedure may be too elevated for the procedure to be indicated. We believe that the decision for laparoscopic approach depends upon size criteria, vascular involvement, and masses position. Lesions up to 5–6 cm and without extensive vascular involvement are feasible to perform by laparoscopic approach.
Conclusion
Postchemotherapy L-RPLND in patients with GCT and residual masses is a safe, feasible, and low-morbidity procedure. However, it remains challenging, as it requires a long steep learning curve and should only be performed in centers with surgeons experienced in laparoscopy. The oncological efficacy of this approach is similar to that obtained in series of open surgery; however, a long-term follow-up is necessary to confirm these data, as well as randomized studies to demonstrate the superiority of L-RPLND.
Ethical Standards
Our study was approved by ethic committee number: CAAE: 47713315.0.0000.5437
Footnotes
Authors' Contributions
E.F.F. was involved in protocol/project development, data collection or management, data analysis, and article writing/editing. H.S.N. was involved in data collection or management, data analysis, and article writing/editing. B.D. wrote and edited the article. R.D.M. developed protocol/project and edited and wrote the article. W.J.M. wrote and edited the article. R.L.M. wrote and edited the article. A.C.S. was involved in data analysis and article writing/editing. M.T.-M. was involved in protocol/project development, data collection or management, data analysis, and article writing/editing.
Disclosure Statement
No competing financial interests exist.