
Abstract
Abstract
Background:
Laparoscopic splenectomy (LS) has become the most common approach for elective splenectomy, but use of LS for patients with massive splenomegaly (MS) remains controversial. By the 2008 European guidelines, LS for MS (spleen size >20 cm) is generally not recommended.
Methods:
We performed a retrospective analysis of 229 consecutive patients undergoing LS, hand-assist (HALS), and open splenectomy (OS) at our institution from January 1, 1995 to December 2016. Eighty-six (38%) had MS. Patient demographics, comorbidities, operative details, and outcomes were analyzed.
Results:
Of 86 patients with MS, 27 (31%) underwent LS, 12 (14%) HALS, and 47 (55%) OS. No significant difference was revealed in patient demographics, comorbidities, American Society of Anesthesiologists class, and spleen size (24.2 cm vs. 23.7 cm vs. 26.6 cm, P = .06). Benign spleen diseases (23), malignancy (57%), and miscellaneous (20%) were indications for surgery. The mean operative time and estimated blood loss in LS, HALS, and OS were 153, 168, and 131 minutes (P = .17) and 100, 162, and 278 mL (P = .24), respectively. Three patients (11.1%) with LS and 1 (8.3%) with HALS required conversion to OS for different reasons (spleen size, technical difficulties, bleeding). Morbidity was similar in all three groups (P = .99). One mortality (1.1%) was noted after OS. Six (7%) patients in the LS group and three (3.5%) in the OS group developed postsplenectomy thrombosis of splenic, mesenteric, and portal veins. Length of stay was shorter in patients with LS and almost reached clinical significance (3.2 vs. 4.9 vs. 5.2 days; P = .06).
Conclusion:
LS is safe, feasible, and associated with shorter hospital stay than HALS and OS for MS.
Introduction
L
The clinical practice guidelines of the European Association for Endoscopic Surgery (EAES) 4 recommend defining splenomegaly in metric terms by preoperative imaging. Splenomegaly is diagnosed when maximum spleen diameter is larger than 15 cm, with massive splenomegaly (MS) having a maximum diameter larger than 20 cm. LS has been deemed safe and feasible approach for splenomegaly in experienced hands, 4 but controversy remains regarding the best approach for MS.
Most studies of LS for MS demonstrate longer operative time, increased blood loss, more perioperative complications, prolonged hospital stay, and higher conversion rate than LS for normal-sized spleens.5,7 Terrosu et al. 6 do not recommend performing LS in patients with spleens weighing 2000 g or more or those exceeding 23 cm in diameter. Boddy et al. 7 consider preferable OS for spleens with detected weight exceeding 1000 g or longitudinal diameter larger than 20 cm. According to EAES guidelines, hand-assist LS (HALS) or OS are preferable in cases of MS due to expected complications with LS. 4 The reasons for these recommendations are limited space for laparoscopy in the abdominal cavity due to splenomegaly and difficult manipulation of enlarged spleens. 8
The goal of this study was to analyze the 21-year experience of our institution with LS, HALS, and OS for splenomegaly and MS.
Materials and Methods
From January 1, 1995 to December 31, 2016, 229 consecutive patients underwent splenectomy for different types of splenic disorders in the General Surgery Department of Mayo Clinic in Jacksonville, Florida. A retrospective review of the medical records was approved by our institutional review board. Data collection consisted of patient demographics, diagnoses, American Society of Anesthesiologists classification scores, operative details, and postoperative morbidity and mortality. Complications were graded by the Clavien–Dindo classification system as minor (Grade I and II) or major (Grade III–V). 9
Splenic size was measured using preoperative imaging. Patients with spleen size exceeding 20 cm were included. Patients undergoing splenectomy for trauma, bleeding varices, or incidental splenectomy performed during other major procedures were excluded. In total, 86 patients (38%) with MS were included in this study; 27 underwent LS, 12 HALS, and 47 OS. Patients were vaccinated for pneumococcus, Haemophilus influenzae, and meningococcus before or after surgery according to protocol. A first-generation cephalosporin was given perioperatively within 1 hour of incision time. No patient underwent preoperative splenic artery embolization.
Study results included patient characteristics, diagnoses, maximum diameter of the spleen measured by preoperative imaging, operation time, estimated blood loss, conversion rates, complications, outcome, and length of stay. Blood loss was based on surgeon and anesthesiologist estimates. Lack of ability to complete the procedure by LS or HALS approach, requiring incision at the midline or left subcostal area, was defined as conversion. Operation time was calculated from first incision to skin closure and postoperative length of stay from postoperative day 1 to discharge. We followed up with all patients for at least 3 months after surgery.
LS was performed by anterior or lateral approach, generally using four trocars. Lateral patient positioning allowed gravity to assist in exposing the retroperitoneal, diaphragmatic, and perihilar attachments. The spleen was turned onto its convex surface after complete disconnection of the spleen from the vessels and surrounding structures. A puncture-resistant, appropriately sized retrieval bag (most frequently used 8 × 10 inch endobag) was introduced through the left subcostal 12 mm trocar. The bag was directed toward the diaphragm and held open facing the camera. Placing the patient in a Trendelenburg position simplified the introduction of the spleen into the bag while pushing gently with graspers. The end of the closed bag was brought outside the abdomen through the trocar site, and the abdomen was desufflated. Subsequently, the spleen was fragmented with finger fracture within the bag, and the resulting blood was suctioned.
Morcellated pieces and aspirated splenic pulp were sent for histological analysis. Enlarging the trocar incisions to more than 3 cm was rarely necessary. In cases of splenic tumor requiring intact organ retrieval, the spleen was removed through an extended trocar incision or accessory Pfannenstiel incision in women for better cosmetic result. In HALS technique, the incision for the hand port was 6.5–7 cm and was located in the left subcostal area. Midline or subcostal incision was used for performing OS. Frequently in MS, the splenic artery was ligated before spleen mobilization in all three techniques.
Continuous variables were shown as mean plus range, and categorical variables were reported as number and percent. Standard statistical analysis was performed, and significance was noted at P < .05.
Results
The evolution of three surgical approaches for splenectomy (OS, HALS, LS) at our institution in two periods of time (1995–2005 and 2006–2016) is shown in Figure 1. The changes in use of OS and HALS between the two time periods were not statistically significant, but the use of LS increased significantly (P < .01).
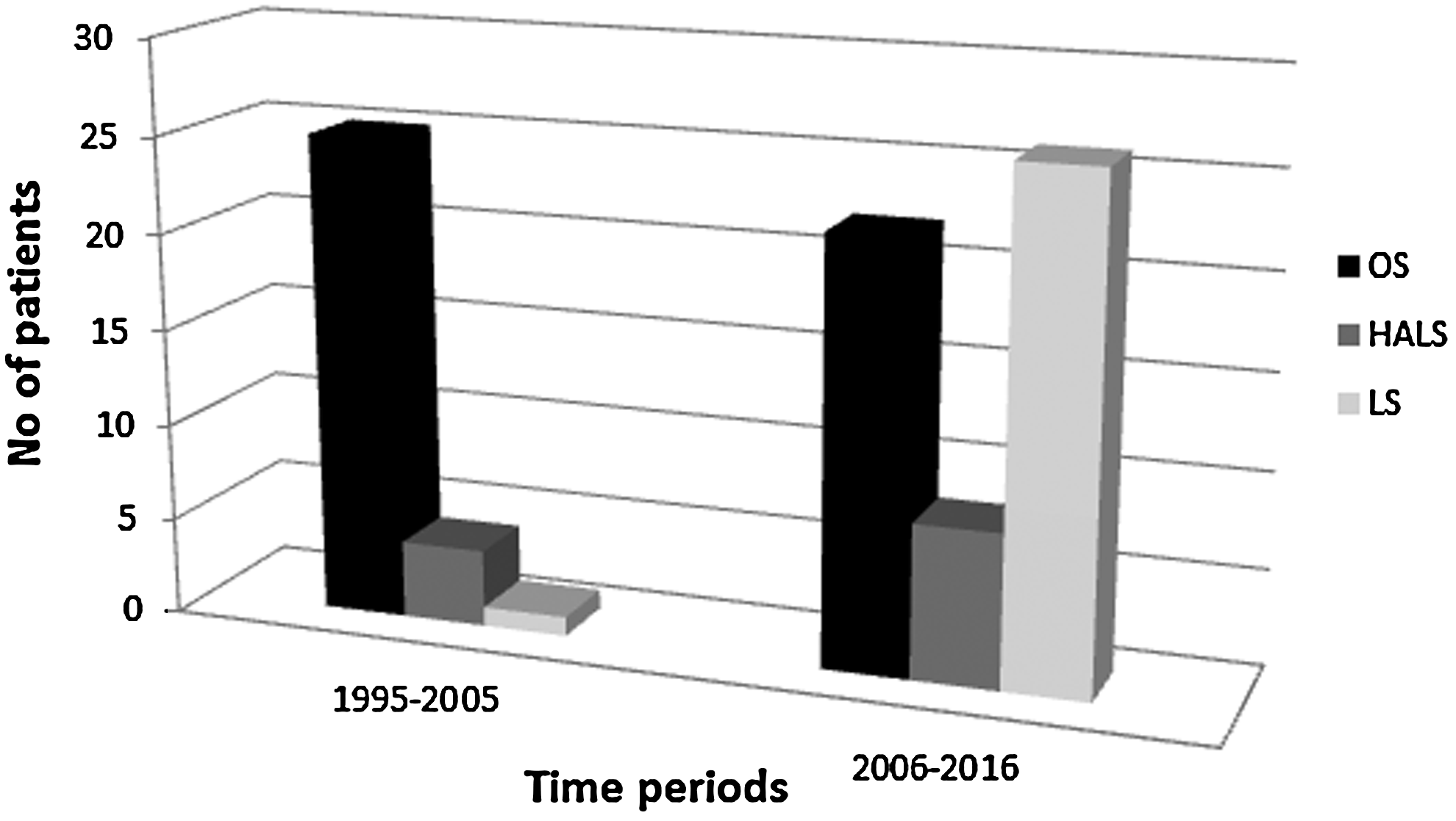
Splenectomy approach for 86 patients with massive splenomegaly during two time periods using OS, HALS, and LS. HALS, hand-assisted laparoscopic splenectomy; LS, laparoscopic splenectomy; OS, open splenectomy.
Patient characteristics according to operative approach are shown in Table 1. No meaningful differences in age, body mass index, comorbidities, previous abdominal surgeries, or American Society of Anesthesiologists class were detected between the three groups. Spleen size was larger for OS compared with HALS and LS (26.6 vs. 23.7 and 24.2, respectively), but did not reach significance (P = .06).
No. (%) unless otherwise indicated.
ASA classification scores of 3 patients were not reported in the charts from 1995.
ASA, American Society of Anesthesiologists score; HALS, hand-assisted laparoscopic splenectomy; LS, laparoscopic splenectomy; MS, massive splenomegaly; OS, open splenectomy; SD, standard deviation.
Perioperative outcomes for the whole cohort are reported in Table 2. OS required less operative time compared with LS and HALS (131 vs. 153 min and 168 min, respectively), but was not significant. Estimated intraoperative blood loss was almost three times higher in OS (278 vs. 100 mL; P = .246) and a higher but not significant rate of blood and platelet transfusions were needed compared with the LS group (Table 2). Conversion to OS from LS was required in 3 patients (11%), 2 due to spleen size (27 cm and 35 cm) and one for other technical difficulties. No conversions were performed for hemorrhage. One case of HALS was converted to OS for bleeding from the vessels of upper pole of the spleen (spleen size of 28 cm).
No. (%) unless otherwise indicated.
NA, not applicable; pRBC, packed red blood cell.
A subgroup analysis of those patients undergoing splenectomy for spleen size ≥30 cm was performed (Table 3). Most (88%) undergoing splenectomy with spleen size of 30 cm or larger underwent OS, which required significantly less operative time than LS (124 vs. 202 min; P = .052). Mean blood loss for patients undergoing OS was 243 mL versus 140 mL in LS. Both of these differences were mostly related to technical difficulties of removing larger spleens through a small abdominal incision. Indications for splenectomy in this group were: lymphoma (n = 8), myeloproliferative disorders (n = 6), Tangier disease (n = 2), and Castleman disease (n = 1).
No. (%) unless otherwise indicated.
Postoperative outcomes are displayed in Table 4. The median length of stay for all patients with MS was 4.7 days. LS was noted to have a significantly shorter length of stay than OS and HALS (3.2 vs. 5.4 days and 4.9 days, respectively; P = .01). One patient from the HALS group required reoperation due to postoperative bleeding (with preoperative diagnosis of splenic artery aneurysm), but no obvious source of hemorrhage was found. Cardiac and pulmonary complications were higher in the OS group than in HALS and LS (12, 4, and 1, respectively). One intra-abdominal abscess was detected in the OS group (requiring percutaneous drainage). Five patients (5.5%) developed postoperative wound infection (4 in OS group and 1 in HALS).
No. (%) unless otherwise indicated.
PST-SMPv, postsplenectomy thrombosis of splenic, mesenteric, portal vein.
Intensive care was necessary for 10 patients (11.6%); just 1 (3.7%) was from the LS group, with pulmonary complications and postsplenectomy hemorrhage requiring transfusions. The morbidity rate was 49% and was lower for LS than OS and HALS (16.2%, 41.6%, and 59.5%, respectively). One mortality was noted in a 70-year-old man who underwent OS for symptomatic splenomegaly (30 cm) due to polycythemia vera and multiple medical comorbidities (congestive heart failure, chronic obstructive pulmonary disease). Other postoperative complications for this patient included pneumonia and multiorgan failure.
In total, 9 (10%) patients developed postsplenectomy thrombosis of splenic, mesenteric, and portal veins, 6 (22%) in the LS group, and 3 (6.4%) in the OS group. Four of these patients required hospitalization with additional therapy and 1 of them underwent an interventional procedure.
Table 5 shows indications for splenectomy in different groups. Almost half of splenectomies were performed for malignant diseases of the spleen (n = 49, 57%).
No. (%).
Discussion
Since the first LS in 1991, 1 the laparoscopic approach has increased in favor over OS because it allows substantial reduction of both mortality and morbidity rates.10,11 LS became the preferred approach in the elective surgical treatment of normal-to-moderately enlarged spleens with benign diseases such as idiopathic thrombocytopenic purpura.3,12
Regardless of the advantages of LS, there have been limitations for this approach in cases of MS (≥20 cm) and supramassive (≥30 cm) splenomegaly. This is explained by technical difficulties due to MS, including decreased working space, adherence with surrounding structures, challenges with retraction and retrieval, and possible trauma to dilated veins or the splenic capsule with subsequent bleeding.12,13 According to the clinical practice guidelines of the EAES, the use of LS should be limited to spleens smaller than 20 cm. 4 Despite this, some authors recommend LS for splenomegaly, regardless of spleen size.8,12,14,15
Intraoperative technical difficulties of LS for MS may require conversion to OS. Poulin and Mamazza 16 reported a 25% conversion rate, and 83% of patients with MS required transfusion. Patel et al. 13 reported a 23% conversion rate, significantly increased morbidity, and longer hospital stay for 27 patients undergoing LS for MS. Consequently, advantages of LS in patients with MS became questionable.
Grahn et al. 15 described 85 patients undergoing LS, 25 (29%) of whom had MS. The conversion rate was significantly higher in patients with supramassive spleens compared with those with massive and normal-sized spleens (P < .01 and P < .01, respectively). No reoperations for hemorrhage or mortality were reported for patients with massive or supramassive spleens undergoing LS, and the mean length of stay was significantly shorter (3.8 vs. 9.0 days; P < .01). The authors concluded that LS is highly recommended for elective splenectomy, despite spleen size. However, this report also gives minimal direction regarding the upper limits of spleen size suitable for LS.
Zhou et al. 14 compared 33 patients with MS undergoing LS (group I), 29 with MS undergoing OS (group II), and 48 with normal-sized spleens undergoing LS (group III). Increased operative time, fewer blood transfusions, and shorter postoperative hospital stay were seen in group I. Patients in group I also had less blood loss and fewer complications than those in group II. Mean spleen size in group I was 22.5 ± 4.9 cm, but no upper limit of spleen size removed by LS was given.
While experience with LS in the setting of MS is limited, Koshenkov et al. 12 shared their experience with treatment of MS. In their study, 22 patients with MS (12 supramassive) underwent LS versus 21 with MS (14 supramassive) who underwent OS. LS was associated with less blood loss (308 vs. 400 mL; P = .24), decreased length of stay (3 vs. 4.5 days; P = .054), and comparable morbidity (17% vs. 14%). Two reoperations and one mortality occurred with OS. Operative times were longer for LS (195 vs. 105 min; P = .008), and the conversion rate was 25%. According to this study, the upper size of the spleen being removed by LS was 30 cm versus 40 cm by OS.
Furthermore, Poulin and Mamazza 16 described LS for the removal of spleens up to 27 cm and 1785 g. The authors suggested preoperative splenic artery embolization as a compliment to LS at this upper size limit. We agree that OS may be most suitable for selected patients with spleens greater than 30 cm, and in general, attempts to remove spleens larger than 30 cm laparoscopically are less likely to be successful and should be applied to selected cases only
Boddy et al. 7 also reported on LS for MS and concluded that carefulness and common sense must be followed when the splenic weight exceeds 1 kg until more definitive evidence is available in the literature. In clinics with appropriate surgical experience, LS or HALS can be performed. Conversely, for the patients with supramassive spleens, OS can be performed quickly and safely without substantially increasing the length of hospital stay or morbidity.
Most patients with MS at our institution safely underwent LS, despite a higher body mass index. The LS approach has been favored in the latter half of the study time period (2006–2016), mainly due to increased experience with minimally invasive surgery and improved instrumentation.
Technical challenges in manipulation of considerably enlarged spleens appear during laparoscopic intervention. 8 Also, placing the spleen into the endobag and finding an optimal way to retrieve the specimen is challenging and the surgeon should have a plan of action.16,17 The open end of the retrieval bag should be placed caudally at the diaphragm. After moving the patient into the Trendelenburg position, the spleen is progressively directed into the bag. Once the spleen is placed into the bag, it is brought through the 12 mm port site or the hand-assist incision and the spleen is morcellated with scissors and ringed forceps. 17 It is important to avoid spillage of splenic tissue in the abdomen. Owera et al. 18 reported that extraction of the specimen through a small incision prolongs operation time by a median of 47 minutes.
In cases where massively enlarged spleens extend to the right hemiabdomen or enter pelvic space, it is difficult to place the spleen into a retrieval bag intracorporeally. For that reason, it is better to retrieve the specimen through an accessory incision. 3 Habermalz et al. 4 suggested extracting an intracorporeally fragmented spleen through a Pfannenstiel incision without using an endobag. This method is not accepted widely due to the risk of developing splenosis. 3 According to some authors, LS is technically difficult in splenomegaly, and the morcellated splenic tissue may be inadequate for histological study.19,20 However, Pugliese et al. 5 reported that morcellated splenic tissue has been considered adequate by their pathologists in all cases.
Several studies have demonstrated that HALS improves intraoperative manipulation of enlarged spleens compared with a totally laparoscopic approach.20,21 Some authors recommend preoperative splenic artery embolization as the first step with subsequent LS or HALS.22,23 Other authors oppose splenic artery embolization before surgery due to additional risks, expenses, and patient dicomfort. 24 Owera et al. 18 did not find preoperative embolization or HALS to be crucial for treatment of MS and this is our experience also.
Our study has two main limitations. First, selection bias was unavoidable due to retrospective design. Second, several different surgeons performed the splenectomies, which may have had an impact on the results of the study as surgeon experience and skills were not identical for the comparative groups. The decision to perform a laparoscopic, hand-assisted or open approach was determined by the surgeon's preference.
Development of minimally invasive surgery skills and revolution in technology have opened doors for a wide range of minimally invasive interventions to replace their open counterparts. Advances in technology offering better outcomes allow surgeons to use modern achievements for treatment of patients with conditions that previously were considered contraindications to LS. Based on our experience, LS is safe, feasible, and associated with better outcomes than HALS or OS for treatment of MS, with an upper limit maximum spleen diameter of 30 cm in skillful hands. In splenomegaly of 30–35 cm, advantages of LS may still be realized, but still debatable due to insufficient data. Splenomegaly of more than 35 cm is usually treated by OS. Surgeon's experience is paramount in deciding the approach.
Footnotes
Disclosure Statement
No competing financial interests exist.