
Abstract
Abstract
Morgagni hernias are a rare form of congenital diaphragmatic hernia, accounting for 2%–3% of cases. The presence of a simultaneous Morgagni hernia and paraesophageal hernia (PEH) is even more rare, with only a few reported cases in the surgical literature. Both open and laparoscopic surgical approaches have been previously described. Herein we discuss a robotic-assisted surgical approach to the repair of simultaneous Morgagni hernia and PEH in a 65-year-old woman. Simultaneous repair of Morgagni hernia and PEH is indicated mainly when symptoms are generally indistinctive. The use of robotic technology allowed for both hernias to be repaired both primarily and with mesh reinforcement.
Introduction
M
The combination of both a PEH and Morgagni hernia is exceedingly rare. To our knowledge, only 9 reported cases in the literature exist, 7 of which underwent successful surgical treatment.5–13 A variety of surgical approaches have been described, including both open and laparoscopic techniques; the use of robotic approaches has not been reported to date. This technical report describes the first use of robotic technology to simultaneously repair both a Morgagni hernia and PEH. The flexibility afforded by the robotic platform provides the minimally invasive surgeon considerable dexterity to tackle these complex hernia repairs, to perform the intracorporeal closure of the hernia defects, and to suture mesh in place to reinforce the repairs.
Technical Report
The operation was carried out in a 67-year-old woman who presented to her primary care physician with complaints of progressive shortness of breath and worsening chest and back pain. Additional symptoms included mild dysphagia to solids with occasional heartburn, but no nausea or vomiting. Computed tomography of the chest demonstrated both a sizeable Morgagni hernia and a PEH (Fig. 1). Preoperative workup included cardiac risk assessment with an electrocardiogram and 2D transthoracic echocardiogram. Esophagogastroduodenoscopy (EGD) demonstrated a large 6-cm hiatal hernia, Los Angeles Classification grade B reflux esophagitis, and chronic gastritis. At the author's institution, we routinely perform high-resolution esophageal manometry in all patients undergoing PEH repair to test for esophageal dysmotility and to tailor our fundoplication; in this case, esophageal manometry demonstrated normal esophageal peristalsis with esophagogastric junction outflow obstruction (elevated integrated relaxation pressure). Given these findings, the patient was offered robotic-assisted simultaneous repair of her Morgagni hernia and PEH, with Nissen fundoplication.

Patient position and port placement
The use of robotic technology was instrumental in allowing us to perform tension-free, mesh-reinforced repairs of both large diaphragmatic hernias. The same ports were used for both repairs. The patient was placed in supine split-leg position, with a nasogastric tube and Foley catheter placed before incision. We entered the abdominal cavity with an 8-mm optical access robotic trocar, placed just to the left of midline about 5-cm superior to the umbilicus. This port was used to establish pneumoperitoneum, and used as our camera port. Two additional 8-mm robotic trocars were placed in the left upper quadrant below the costal margin, one at the midclavicular line and another at the anterior axillary line. Another 8-mm robotic trocar was placed in the right upper quadrant at the midclavicular line. A 12-mm assistant port was placed medially in the left upper quadrant, at the level of the camera port. A small 5-mm incision was made in the subxiphoid area, and the left lobe of the liver was retracted anteriorly using a Nathanson retractor (Cook Medical, Bloomington, IN) (Fig. 2).
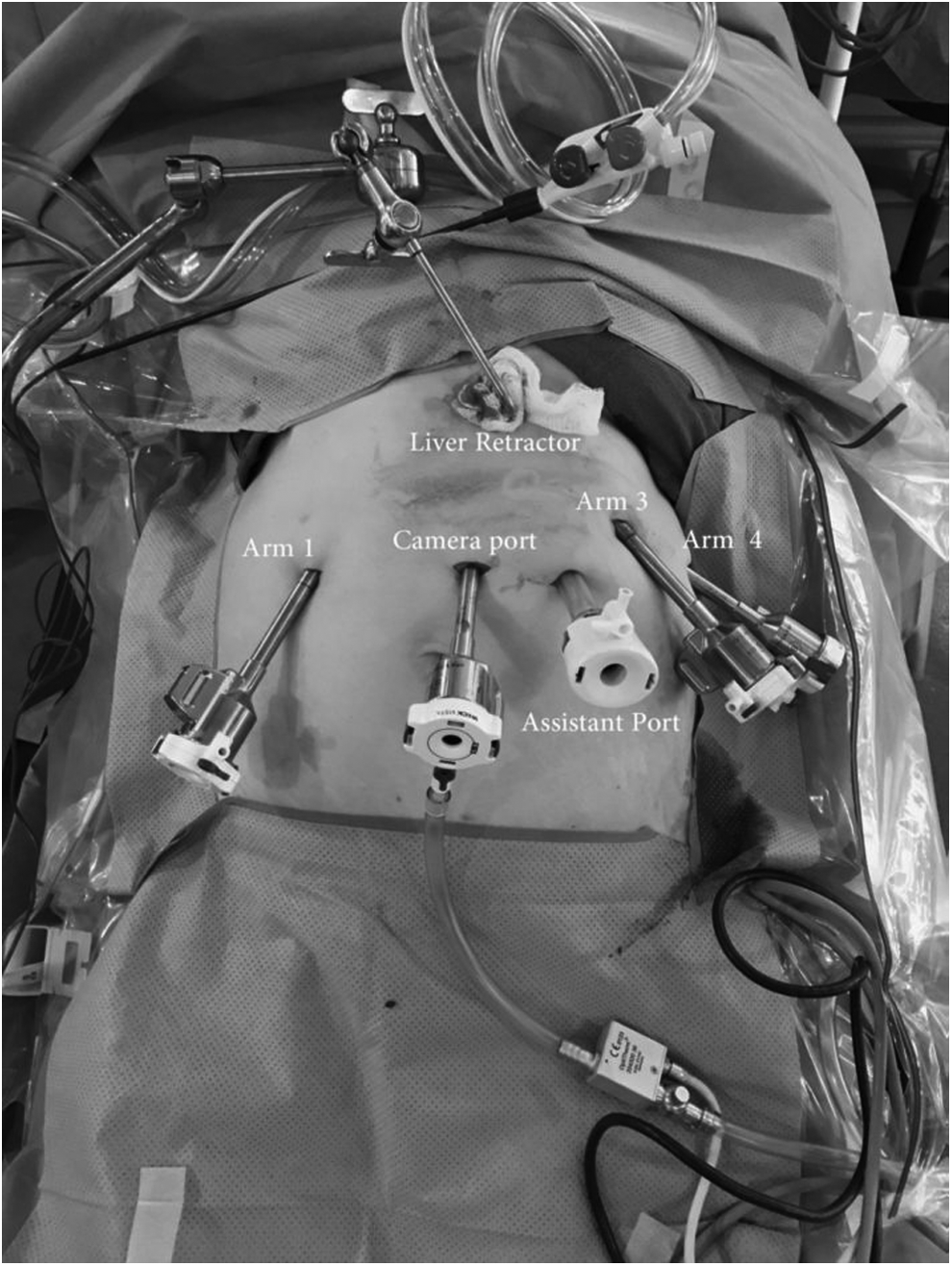
Placement of four robotic trocars, an assistant port, and a liver retractor used in this operation.
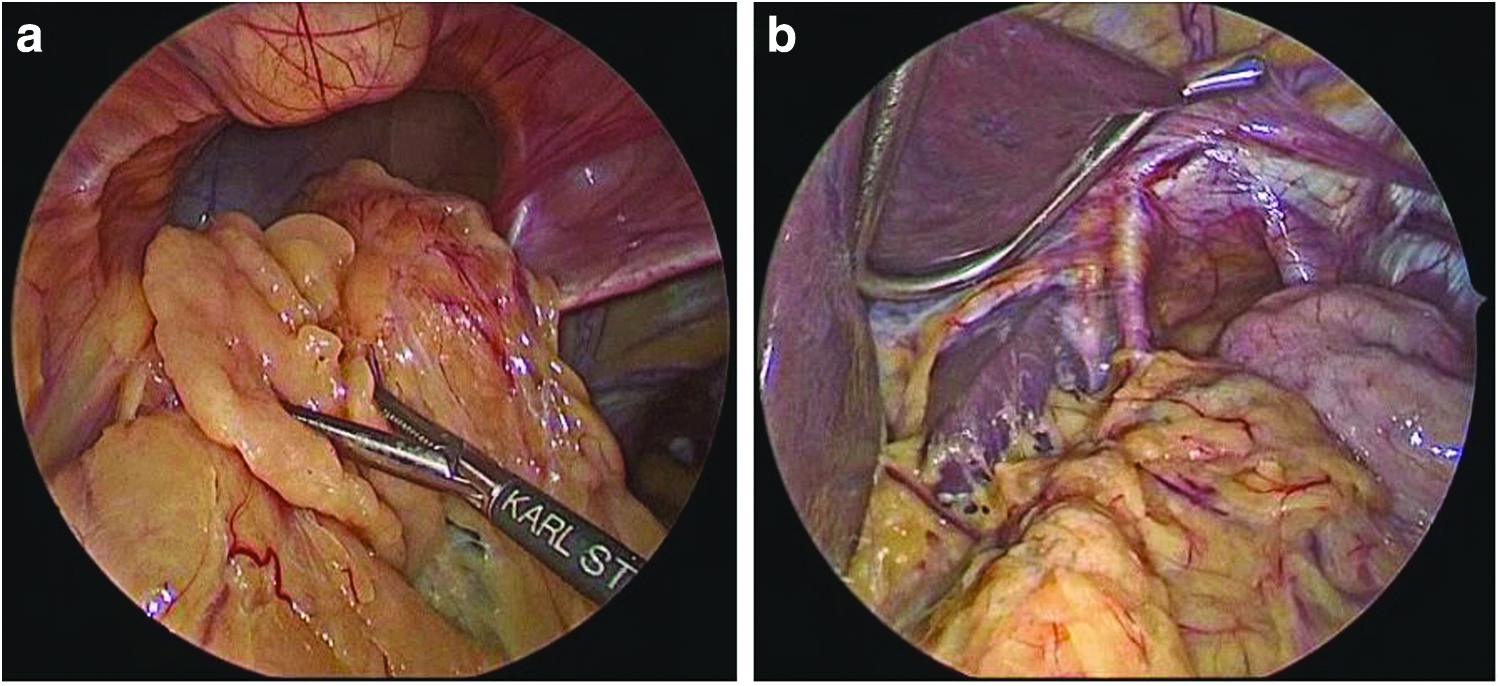
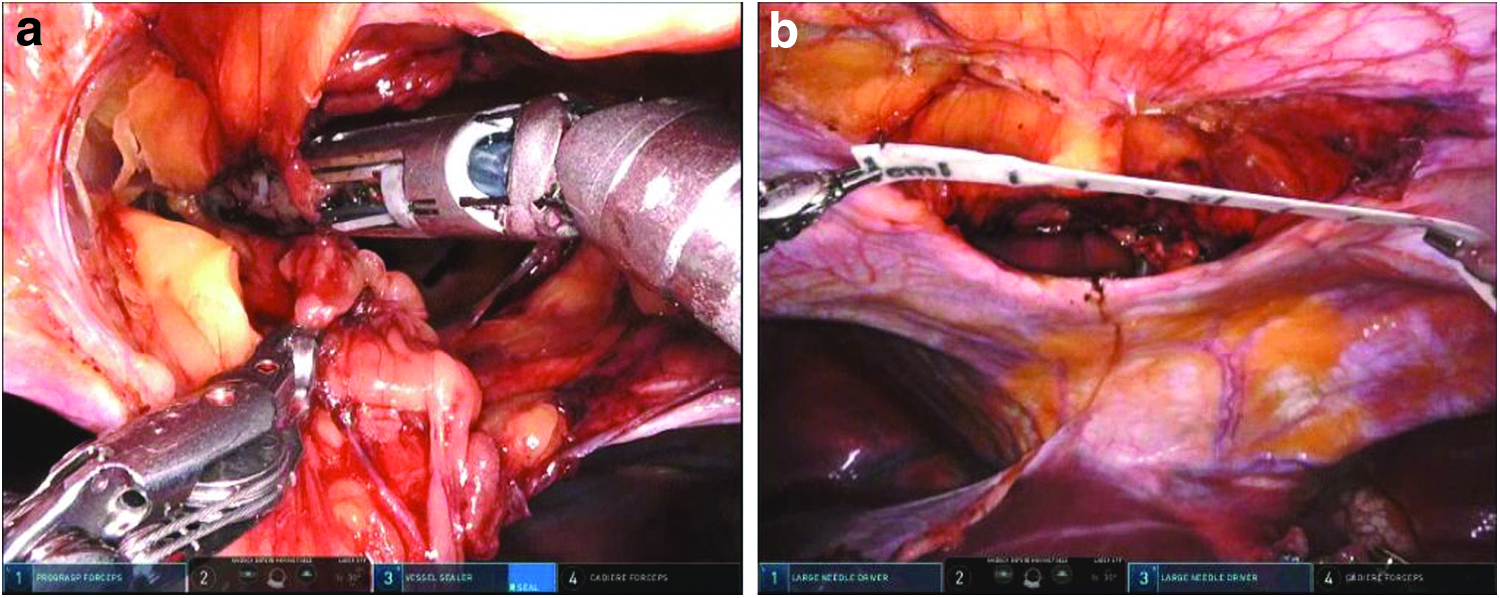
Upon entering the abdominal cavity, a large portion of greater omentum was discovered stretching anteriorly, incarcerated within the Morgagni hernia. The patient was placed in steep reverse Trendelenberg position, using gravity to help reduce the hernia contents. The omentum was gently reduced with laparoscopic graspers, revealing a large anterior diaphragmatic defect (Fig. 3a). Next, the esophageal hiatus was explored, and a large PEH was confirmed with half of the stomach herniated into the posterior mediastinum (Fig. 3b). The Da Vinci Xi robotic system (Intuitive Surgical, Inc., Sunnyvale, CA) was then brought into the operative field and attached to the specific trocars.
PEH repair with mesh
We began by repairing the PEH. Our approach for robotic-assisted repair of PEHs has been described previously in the literature. 14 Robotic Cadiere forceps (Intuitive Surgical, Inc.) were used to gently retract the herniated portion of stomach, and early division of the short gastric vessels was carried out with a robotic vessel sealer device. We used the vessel sealer to divide the pars flaccida and expose the left diaphragmatic crura. Incision of the hernia sac was started at its junction with the left crura, and continued in a circular manner around the esophageal hiatus. The hernia sac was carefully dissected circumferentially off its mediastinal attachments and fully separated from the pleura. Cephalad dissection of the esophagus was carried into the posterior mediastinum, until the gastroesophageal junction was mobilized 2–3 cm below the level of the diaphragm, without retraction or tension. The vessel sealer was then exchanged for robotic needle drivers, which allow the surgeon considerable dexterity and the ability to suture in multiple directions. Primary closure of the diaphragmatic crura was performed with 2-0 nonabsorbable barbed V-loc sutures (V-loc; Medtronic, Dublin, Ireland), placed posteriorly along the left and right crura in a running manner. The cruraplasty was then reinforced with a 10 cm by 7 cm absorbable biosynthetic mesh (Bio-A; W. L. Gore & Associates, Inc., Newark, DE), with an anterior opening to accommodate the esophagus. Interrupted 2-0 silk sutures were placed around the esophageal hiatus and posteriorly through the cruraplasty, affixing the mesh in place (Fig. 4). A floppy Nissen 360° fundoplication was created over a 56-French bougie (Fig. 5).
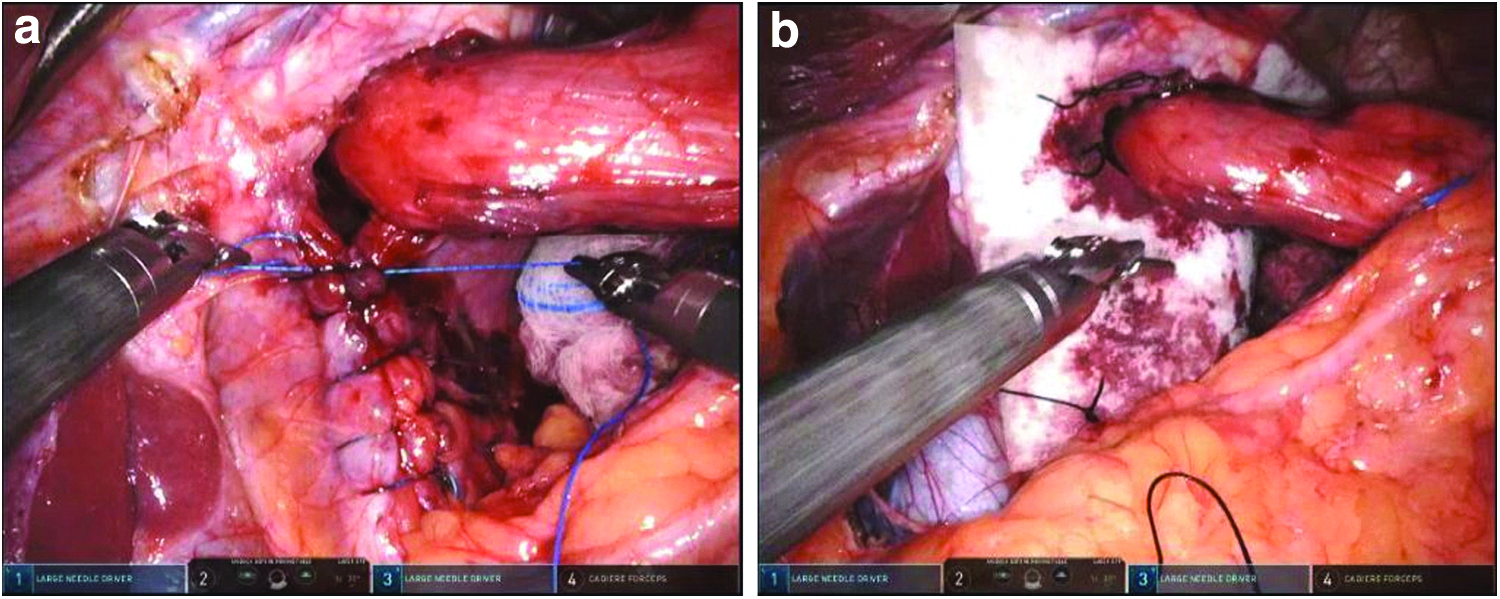
A 360° Nissen fundoplication was performed.
Morgagni hernia repair with mesh
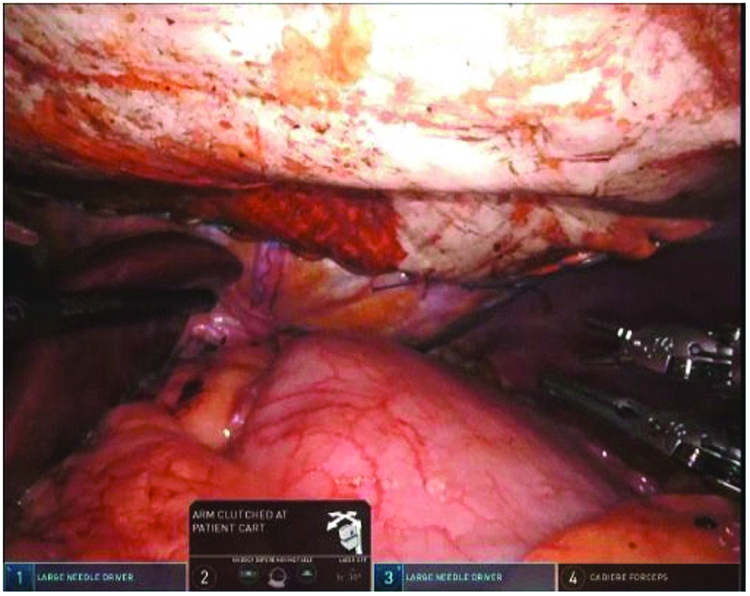
We then continued with the repair of the anterior Morgagni hernia defect. Using the same port placement, the robotic camera of the Xi robotic system was then rotated to a 30° up (anterior) view. The liver retractor was removed. The operation was begun by taking down the falciform ligament with the robotic vessel sealer. The hernia sac was then circumferentially mobilized from the anterior mediastinum and excised. Our goal for this repair was to perform a robotic intraperitoneal onlay mesh (IPOM) repair after closing the diaphragmatic defect primarily. The anterior diaphragmatic defect was measured to be 7 cm by 5 cm in size (Fig. 6).
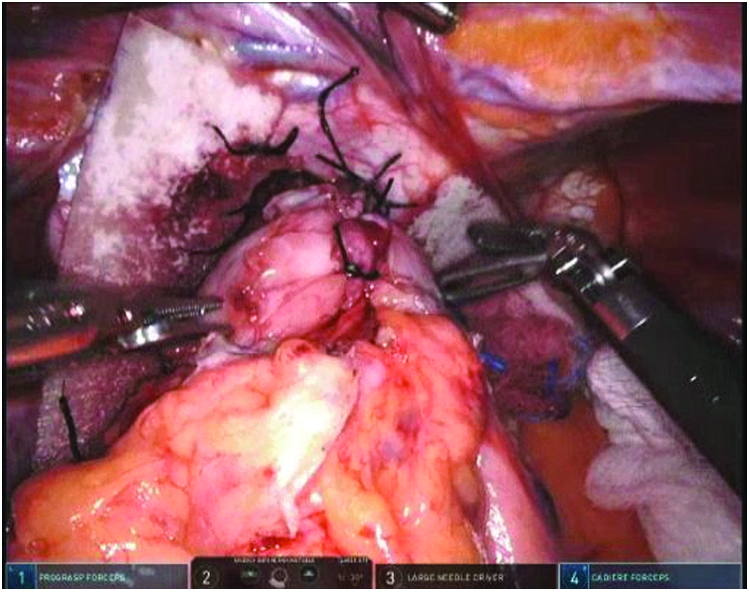
The defect was primarily closed in a continuous manner with 0 V-loc sutures running transversely along the hernia defect using two robotic needle drivers (Fig. 7). A large 10 cm by 15 cm expanded polytetrafluoroethylene mesh (Dual-Mesh; W. L. Gore & Associates, Inc.) was laid over the repaired defect and held in place by an assisting robotic arm. The mesh was then sutured in place along its entire circumference with two running nonabsorbable 2-0 V-loc sutures (Fig. 8). After this was accomplished, the hernia sac was removed from the abdomen. An intraoperative EGD was performed to confirm proper positioning and patency of the PEH repair and fundoplication. The trocars were all removed under vision, and the fascia at the 12-mm assistant port site was closed with suture.

The Morgagni diaphragmatic defect was primarily closed with nonabsorbable barbed suture.
The Morgagni hernia repair was reinforced with expanded polytetrafluoroethylene mesh.
Discussion
First described in 1769, the eponymous Morgagni hernia is a retrosternal defect between the sternal and costal attachments of the diaphragm. 2 These hernias are located anteromedially, and 90% hernias are found on the right side, with omentum, colon, and stomach being the most common hernia contents found.15,16 As a form of congenital diaphragmatic hernia, most Morgagni hernias present during childhood. Those that are discovered later in life usually present with nonspecific respiratory, gastrointestinal complaints, or dull chest or epigastric pain. 3
Once a Morgagni hernia has been identified, surgical repair is typically recommended, due to the risk of incarceration or strangulation of hernia contents. A variety of surgical approaches have been described, ranging from open midline laparotomy, open thoracotomy, or laparoscopic reduction and repair. 3 Some controversy exists regarding excision of the hernia sac; some surgeons advocate for its removal, whereas others argue that excision can lead to significant pneumomediastinum and increase the chances of damage to mediastinal structures.3,17 Repair of the anteromedial diaphragmatic defect can be performed either primarily or with mesh, as both have been described in the literature. 3 Our surgical approach followed the same general surgical principles popularized for ventral and incisional hernia repairs, utilizing both primary closure of hernia defects and mesh reinforcement.13,14 Recently, the use of robotic technology has been reported for the repair of Morgagni hernias alone. 20 The authors similarly performed both primary and mesh repair of the hernia defects, and pointed to the flexibility of the robotic platform to perform the complex suturing and dissections necessary for these repairs.
In contrast, PEHs are more commonly encountered than Morgagni hernias, but still represent only 5% of diaphragmatic hiatal hernias. 4 The large majority are found in elderly patients, typically female. 21 Similar to Morgagni hernias, they present with a variety of nonspecific gastrointestinal complaints, reflux symptoms, chest or epigastric discomfort, or respiratory symptoms. 21 Recent population-based studies have estimated the risk of emergency surgery to be 1.16% per year, with a lifetime risk of 18% at 65 years of age. 22 Based on these findings, watchful waiting is now considered a reasonable option in truly asymptomatic patients. 23 The laparoscopic approach is increasingly being used, and has been suggested as the standard of care for these PEH repairs. 24 Again, the use of robotic technology has been described in the repair of these complex hernias as well, allowing for increased flexibility in mediastinal dissection and the suturing of mesh to reinforce the hernia repair. It has previously been demonstrated that the use of robotic technology for the treatment of PEH provides perioperative results equivalent to its laparoscopic counterpart. 14
The coexistence of two nontraumatic diaphragmatic hernias is exceedingly rare, and the presence of both a Morgagni hernia and PEH simultaneously has only been reported a handful of times.5–13 Owing to the similarities and nonspecific nature of presenting symptoms, it is often difficult to determine which hernia is chiefly responsible for the patient's complaints. Indeed, our patient experienced symptoms that could be attributed to either hernia, and thus, she was offered simultaneous repair of both hernias. Likewise, in all of the cases reported in the surgical literature, both hernias were fixed simultaneously. The surgical techniques that were utilized have varied, but open5,7,8,11 and laparoscopic9,10,12 approaches have been performed. To our knowledge, this report represents the first description of robotic-assisted repair of simultaneous Morgagni hernia and PEH.
As surgeons become increasingly familiar with the technology, robotic surgery is being applied to a wider set of clinical situations. Robotic-assisted repairs of ventral hernia,18,19 PEH, 14 and Morgagni 20 hernia have all been described. Despite the variety of applications, all of these repairs follow similar surgical principles: careful dissection, minimizing tension on repairs, and the frequent combination of primary closure of hernia defects along with mesh reinforcement. The robotic IPOM technique is well suited for the repair of Morgagni hernias, as it allows for straightforward primary closure of the fascial defect as well as precise mesh fixation over the hernia, especially useful given their proximity to the pericardium. In this case, the robotic approach was not only shown to be feasible but also flexible enough to approach both the PEH and Morgagni hernia with excellent visualization. Furthermore, the robotic approach maintained many of the benefits of performing minimally invasive surgery, with reduced postoperative pain and length of stay.
In this case, the patient was started on clear liquids on postoperative day 1 without difficulty, and was discharged home later that day on an esophageal diet. The patient was seen in follow-up 3 months later, tolerating a soft diet without issue, and reporting none of her preoperative symptoms.
Conclusion
Simultaneous repair of Morgagni hernia and PEH is indicated when both hernias are discovered, as their symptoms are often indistinctive. The use of robotic technology facilitates primary closure of the defects and mesh placement in these complex diaphragmatic hernia defects. This case illustrates yet another novel application of robotic surgery in tackling an unusual and rare surgical condition.
Footnotes
Disclosure Statement
Dr. Carlos Galvani is a consultant for Intuitive Surgical, Inc. For all other authors, no competing financial interests exist.