
Abstract
Abstract
Introduction:
Laparoscopic sleeve gastrectomy (LSG) has shown excellent results in terms of weight loss and resolution of comorbidities. Despite that, the effect of LSG on gastroesophageal reflux disease (GERD) is still a controversial topic. Our objective was to evaluate the presence of gastroesophageal reflux symptoms, erosive esophagitis (EE), and hiatal hernia (HH) in obese patients undergoing LSG.
Methods:
Prospective observational study. LSG patients were studied before and at 18-month follow-up. Demographics, anthropometrics, status of comorbidities, perioperative data, GERD symptoms, and esophagogastroduodenoscopy (EGD) findings were evaluated.
Results:
Between June 2012 and July 2014, 285 patients underwent LSG. Pre- and postoperative data were available in 109 patients; therefore, they were included in the study. There were 72 women (66%), age 40 ± 9 years. Preoperative body mass index (BMI) was 47.8 ± 16 kg/m2. At 18-month follow-up, body mass index and percentage excess weight loss were 29.3 ± 6 kg/m2 and 64% ± 9.4%, respectively. Resolution/improvement of comorbidities was as follows: diabetes 73%, hypertension 57.5%, and obstructive sleep apnea 89%.
GERD symptoms increased from 33% to 44% (P = no statistical significance), EE from 20.1% (100% grade A) to 33.9% (74% grade A) (P < .001), and HH from 22% to 34.8% (P < .001). Postoperative findings on symptomatic patients were as follows: EE was found in 64.5%, HH in 23%, while 12.5% had normal EGD. There was a significant association between manifestation of GERD symptoms and the presence of EE on EGD (P < .05). Symptoms de novo were observed in 36.9% of patients, EE in 28.7%, and HH in 16.4%. Complication rate was 3.5%; there was no mortality.
Conclusion:
The prevalence of GERD symptoms, EE, and HH was increased after LSG. At 18-month follow-up, severity of esophagitis was mild, the majority of them being Grade A esophagitis. There was good correlation between manifestation of GERD symptoms and the presence of EE on EGD.
Introduction
L
Upon literature review, we found difficulties while analyzing results due to disparity in patient evaluation parameters. Interestingly, there are some objective studies based on esophageal function test (EFT) such as manometry and 24-hour pH monitoring or impedance that demonstrate a strong association between LSG and postoperative GERD.3–5
A normal esophagogastroduodenoscopy (EGD) does not exclude the absence of GERD since 50%–60% of the patients with documented GERD by pH monitoring do not have esophagitis. Conversely, the presence of esophagitis is an unequivocal sign of GERD.6,7 An increased incidence of low-grade esophagitis after LSG has been recognized by several authors, although progression to more severe grades or even Barrett's esophagus (BE) has also been published.8–12
Another controversial aspect includes the identification and simultaneous repair of hiatal hernias (HHs) during LSG. The prevalence of HH in obese patients is around 40%–50%.13,14 Many surgeons consider that simultaneous HH repair is safe and reduces the incidence of postoperative GERD, although others do not agree with this position.14–22
Our objective was to evaluate the presence of GERD symptoms, prevalence and evolution of erosive esophagitis (EE), and HH in obese patients undergoing LSG at 18-month follow-up.
Methods and Procedures
This was a prospective observational study. Data on patients undergoing LSG for the treatment of obesity at the Bariatric Surgery Department, Hospital Privado Córdoba, Argentina were analyzed.
Demographic data, preoperative, and 6-, 12-, and 18-month follow-up body mass index (BMI), percentage excess weight loss (%EWL), resolution/improvement of comorbidities were evaluated. The following criteria were used to assess comorbidity status: Brethauer criteria were considered for hypertension (HT), 23 American Diabetes Association for diabetes (DBT), 24 and clinic criteria for obstructive sleep apnea (OSA) such as decrease in daytime sleepiness and nocturnal snoring.
GERD was defined according to the Montreal Consensus 25 ; GERD-like symptoms were assessed based on a designed questionnaire implemented during preoperative evaluation and at 18-month follow-up 22 (Table 1). EGD was performed preoperatively and at 18-month follow-up. Findings such as presence of EE and HH were evaluated. Los Angeles classification was used for EE. 26 HH was diagnosed based on HH Society of American Gastrointestinal and Endoscopic Surgeons guidelines. 27 HH was diagnosed either during preoperative endoscopy and/or intraoperative visual assessment of the anterior hiatus. The crura was not dissected systematically looking for HH. Correlation between preoperative EGD and intraoperative findings was 100%.
Proton pump inhibitors (PPIs) were prescribed routinely after LSG for 12 months, independently from the presence/absence of symptoms. If EE was found during the 18-month follow-up EGD, the patient was prescribed PPIs again for 12 weeks (omeprazole 80 mg/day). EGD was repeated after that period of time only in patients with EE grade B or C. Helicobacter pylori (HP) was investigated by taking gastric biopsies according to the Sydney protocol. 28 If HP tested positive, patients were treated with amoxicillin 2 g/day, clarithromycin 500 mg/day, and omeprazole 20 mg/day for 14 days before LSG. Esophageal biopsies were taken only if BE was suspected, following the Seattle protocol. 29 Morbidity and mortality were analyzed as well.
Surgical technique
A 12-mm optical trocar was inserted (XCEL® Endopath; Ethicon Endosurgery, Cincinnati, OH) for the camera in the midline supraumbilical position under direct vision; then, two 5-mm trocars were inserted: one on the left upper quadrant and the other one on the right upper quadrant; and a 10-mm trocar was introduced on the left flank. The Nathanson liver retractor was placed in epigastrium. The short gastric vessels were all divided using the harmonic scalpel (HARMONIC ACE®; Ethicon Endosurgery). Dissection of the greater curvature of the stomach continued toward the left pillar of the crus. The gastric sleeve was calibrated with a 42 Fr bougie. Then, using between 4 and 5 linear staplers (ECHELON 60; Ethicon Endosurgery) the stomach was divided vertically starting on the greater curvature about 4–6 cm from the pylorus parallel to the lesser curvature and from this position toward the angle of His. Black (4.4 mm), green (4.1 mm), gold (3.8 mm), or blue (3.5 mm) cartridges were chosen depending on the thickness of the stomach wall. Staple line was reinforced with running stitches of absorbable suture. The specimen was retrieved in a plastic bag. A multilumen drain was left.
If a HH was identified the repair was performed by dissecting the crura, returning the stomach to its abdominal position, and closing the crura defect posteriorly with 2-0 Polyester (ETHIBOND® 2-0; Ethicon) interrupted stitches. The same 42 Fr bougie was used for calibration.
Results
Between June 2012 and July 2014, 285 patients underwent LSG at our Institution. Pre- and postoperative data were available in 109 patients; therefore, they were included in the study. There were 72 women (66%); the average age was 40 ± 9 years. Preoperative BMI was 47.8 ± 16 kg/m2. At 18-month follow-up, BMI and %EWL were 29.3 ± 6 kg/m2 and 64% ± 9.4%, respectively. Changes in BMI and %EWL are shown in Table 2. Thirty-three patients (30.2%) tested positive for HP during their preoperative evaluation and received treatment before the operation.
P < .001.
BMI, body mass index; %EWL, percentage excess weight loss.
Evolution of comorbidities after LSG
Preoperatively, there were 26 patients (23.8%) with type 2 DBT, 40 (36.6%) with HT, and 19 (17.4%) with OSA. After LSG, resolution/improvement of comorbidities was as follows: DBT 73%, HT 57.5%, and OSA 89% (Table 3).
DBT, diabetes; HT, hypertension; LSG, laparoscopic sleeve gastrectomy; OSA, obstructive sleep apnea.
Morbidity and mortality
Complications occurred in 4 patients (3.6%). They all presented postoperative hematoma although only one of them required percutaneous drainage; the remaining 3 patients were managed conservatively. There was no mortality in this series.
None of the patients required conversion to Roux-en-Y gastric bypass (RYGB) due to GERD symptoms or EGD findings.
Evolution of GERD symptoms after LSG
The number of patients reporting GERD symptoms increased from 36 (33%) before the surgery to 48 patients (44%) after the operation (P = no statistical significance). Specifically, 15 out of 36 patients (41.6%) who had preoperative symptoms reported resolution of them after LSG, and 21 out of 36 (58.4%) remained the same. Interestingly, 27 out of 73 patients (36.9%), who did not have symptoms preoperatively, reported having de novo symptoms after LSG (Fig. 1).
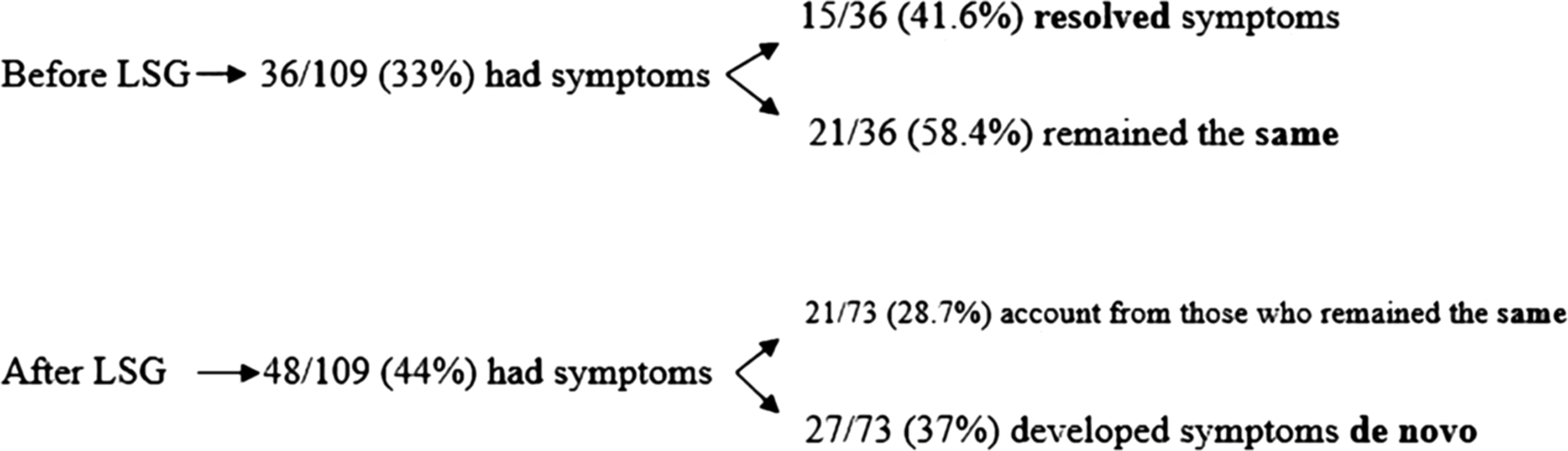
Evolution of symptoms. LSG, laparoscopic sleeve gastrectomy.
For those 36 patients with preoperative symptoms, preoperative findings were as follows: EE was observed in 38% of them, HH in 45%, while 17% had normal EGD. Postoperative findings on those 48 symptomatic patients were as follows: EE was found in 31 patients (64.5%), 11 (23%) had HH, and 6 (12.5%) had normal EGD. There was a significant association between manifestation of GERD symptoms and the presence of EE on EGD (P < .05). The most frequently reported symptom was heartburn (40 patients = 84%) followed by regurgitation (8 patients = 16%).
Thirty-eight (79%) patients reported their postoperative symptoms as mild in intensity and low in frequency (mild), and they all had complete response to standard doses of PPIs. Six patients (12.5%) reported experiencing symptoms at least thrice per week (moderate) and they also responded to standard doses of PPIs. The remaining 4 patients (8.5%) reported having daily symptoms (severe). They were prescribed double doses of PPIs for 6 months, with good response in all cases.
Evolution of EE after LSG
During preoperative evaluation, 22 patients (20.1%) had EE (all Grade A). All these patients were offered to have RYGB surgery, but they refused to have that kind of operation. Hence, they were all specifically informed about the risk of worsening their EE status after LSG. Despite that, they all preferred to have LSG. At 18-month follow-up, EGD findings were as follows: 37 patients (33.9%) showed EE (P < .001). Of those, 28 patients (74%) had Grade A esophagitis, 7 (20%) had Grade B, and 2 (6%) had Grade C.
Evolution of EE on those 22 patients who had this condition preoperatively was as follows: 10 patients (45.5%) resolved their EE after LSG, although the remaining 12 (54.5%) persisted with the same Grade of esophagitis they had before the operation.
Interestingly, 25 patients (28.7%) developed de novo EE. Of them, 16 (64%) had Grade A esophagitis, 7 (28%) Grade B, and 2 (8%) Grade C. PPIs were prescribed in all cases for 12 weeks. EGD was repeated only in patients with Grade B and C esophagitis upon treatment completion showing the following results: 5 out of 7 patients (71.4%) who had Grade B esophagitis resolved their condition; the other 2 (28.6%) remained the same, as well as those who had Grade C esophagitis. None of them had BE. The remaining 72 patients (66%) failed to show any signs of EE.
Evolution of HH after LSG
The number of patients with HH significantly increased from 24 (22%) to 38 (34.8%) after the operation (P < .001). Simultaneous repair during LSG was considered necessary in only 6 patients out of 24 (25%). Three of those 6 patients (50%) showed recurrence of their HH on EGD, although they were all about 2 cm in size. Remarkably, de novo HH was observed in 14 patients (16.4%). When analyzing the presence/absence of EE on these 38 patients, we found that 21 of them (55.2%) had normal findings, whereas the remaining 17 (44.8%) had EE.
Evolution of symptoms, EE, and HH are shown in Table 4.
EE, erosive esophagitis; GERD, gastroesophageal reflux disease; LSG, laparoscopic sleeve gastrectomy; NS, no statistical significance.
Discussion
LSG has gained popularity during the last decade. Ever since ASMBS accepted this operation as a primary bariatric procedure in 2012, results have been encouraging.30–39
Nevertheless, the relationship between LSG and postoperative GERD is still a matter of debate. Prevalence of GERD within the general population has been estimated around 14%–28%.40–42 Obesity is a well-known risk factor for developing GERD with its consequent complications such as esophagitis, BE, and esophageal adenocarcinoma.43–48
Possible factors related to GERD after LSG have been well studied.49–53 These factors are enumerated in Table 5.54–62
GERD, gastroesophageal reflux disease; LSG, laparoscopic sleeve gastrectomy; LESP, lower esophageal sphincter pressure.
There is general agreement in that GERD diagnosis must be based on four pillars: symptoms, EGD, barium swallow, and EFTs such as esophageal manometry and 24-hour pH monitoring. EFTs have demonstrated high sensitivity and specificity, and they are the only objective test available for diagnosis of this disease.63–65 Despite all the controversies found in the literature, when analyzing carefully objective data, there is no question that there is a strong association between LSG and the appearance of postoperative GERD.66–69 As such, Gorodner et al. reported a significant decrease in lower esophageal sphincter pressure (LESP), increase in the DeMeester score, and development of de novo GERD in 36% of patients after LSG, documented by objective studies. 3 Braghetto et al. also found a significant decrease in LESP, symptom worsening, and development of esophagitis. 4 Del Genio et al., performed high resolution manometry and impedance and pH monitoring on 25 patients (pre and post LSG). They were able to demonstrate a significant increase in esophageal acid exposure, number of nonacidic postprandial reflux events, and DeMeester score. 5 Contrariwise, Rebecchi et al. published their series showing a significant decrease in the DeMeester score in patients who were diagnosed with GERD preoperatively. They did not find any changes in LESP. However, the incidence of de novo GERD was still 5.4%. 10
Evolution of GERD symptoms after LSG
It is well documented that evaluation of symptoms by itself is not reliable when diagnosing GERD, 65 although several authors still base their diagnosis on symptoms. In 2012, the International Expert Consensus reported 12.1% incidence of postoperative GERD. 15 Carter et al., published their series showing an increase in postoperative symptoms from 34.6% to 49%. 66 Other authors experienced similar results.9,67–69 Inversely, Gibson et al., published their results on 500 patients undergoing LSG at 14-month follow-up. According to them the percentage of patients experiencing symptoms fell from 45% to 6%. 17 Other authors reported comparable outcomes.58,59,62,70
In our experience, the percentage of patients with postoperative symptoms was increased, although this number did not reach statistical significance. Remarkably, 41.6% of our patients reported resolution of their symptoms after the operation.
Evolution of EE after LSG
In agreement with the literature, we consider that endoscopic findings do not exclude the presence/absence of GERD. Mucosal lesions can be absent in up to 50%–60% of patients with documented GERD. Nevertheless, we believe that endoscopic findings are crucial not only during preoperative testing but also during follow-up, especially for those patients showing endoscopic abnormalities. Braghetto et al., found EE in 15.5% of their patients after LSG. 8 Likewise, Tai et al. observed a significant increment in the incidence of EE going from 16.7% to 66.7% (P < .001); the majority of patients had Grade A esophagitis. It is worth mentioning that 36% of them progressed either to Grade B or C esophagitis after LSG. 9 In our series, 20.1% of patients had EE preoperatively (all Grade A). This number rose to 33.9% after the operation. It is important to mention that 45.5% resolved their condition and that none of those who remained with EE worsened their status. However, for some reason, the severity was worse on those who showed de novo EE, since the only cases of Grade B or C esophagitis were found in this group. Half of these patients showed good response to PPIs, while the other half maintained their EE status.
These findings should not be underestimated, since one of the ominous complications of GERD is the development of BE and eventually adenocarcinoma of the esophagus. Literature about development of BE after bariatric surgery is scarce. Recently, Braghetto published their series of 231 post LSG patients at 6-year follow-up. They found an incidence of 1.2% of BE in this group of patients. 12 This experience arises concern, since the presence of BE increases the chances of having esophageal adenocarcinoma between 30 and 40 times.
Evolution of HH after LSG
Another controversial topic is whether HH should be a contraindication for LSG. If not, should it be repaired simultaneously? Prevalence of HH within the obese population has been reported at around 40%–50%.13,14 Many surgeons confirmed that simultaneous HH repair during LSG was safe and decreased the incidence of postoperative GERD, although others did not agree with this premise. Overall, the International Expert Consensus reflected that 83% of responders recommend aggressive identification of HH during surgery, while 82% believed it should be repaired at the same time. 15 Daes et al., published their series of 382 patients who underwent LSG. HH was seen during EGD in 51% of them and they all underwent LSG+HH repair. According to them, GERD was diagnosed preoperatively in 74% of these patients who had HH. It is worth mentioning that this diagnosis was based on symptoms, medication use, and presence of EE on EGD. After LSG+HH repair, the prevalence of GERD significantly decreased from 74% to 2.6%. 14 Conversely, Santonicola et al. compared results on 78 patients undergoing simultaneous LSG and HH repair versus 102 patients in whom only LSG was performed. They found that GERD was significantly decreased only in the last group. Surprisingly, the group with simultaneous LSG and HH repair reported an increased incidence of heartburn. 21 In our series, we found a significant growth in the number of HH after the operation that went from 22% to 34.8%. We considered that simultaneous repair was necessary in only 25% of those HH that were diagnosed preoperatively. This number is relatively low if we compare it with other experiences. We believe that our simultaneous repair rate might have been low due to discrepancies between preoperative diagnosis and intraoperative findings. Another cause might have been that we did not aggressively look for HH. The reason is that small HH seen during EGD might not have been visible during intraoperative assessment. Under these circumstances, we do not consider it necessary to dissect a normal hiatus having to repair it later, since it has not been demonstrated that this could result in any benefit. Still, our recurrence rate of 50% was high. In addition, despite being so careful and selectively repairing only those we considered necessary without disrupting any normal hiatus, our incidence of HH de novo of 16.4% was also high. We believe that this might be due to the existence of underdiagnosed cases during the preoperative evaluation or due to the presence of mild weaknesses within the hiatus that become larger after weight loss.
Interestingly, EE was observed in 44.8% of those patients who presented HH after the LSG.
There were no conversions to RYGB in this series. Conversions would be considered appropriate under the following three circumstances:
1. Patients with severe GERD symptoms affecting their quality of life, with no response to medical treatment. 2. Young patients with esophagitis Grade C or D with no endoscopic response after medical treatment or patients showing progression of their esophagitis. 3. Presence of BE confirmed by pathology.
Although EFTs are the only objective tool for diagnosing GERD, we do not consider that an abnormal pH monitoring in an asymptomatic patient, without signs of esophagitis on EGD, is an indication for conversion.
Preliminary results of this study were enough reason for us to change our strategy. Based on preoperative evaluation results, if the patient complains about moderate/severe GERD symptoms, or esophagitis and/or HH >2 cm are observed on EGD, then the indication would be to perform a RYGB.
But, going back to the beginning, would GERD be a contraindication for LSG? In concordance to what has been previously discussed, we consider GERD as a relative contraindication for LSG. However, we do believe that BE is an absolute contraindication for LSG. Due to an increased risk of developing BE, we think that follow-up on patients who show postoperative EE grade B, C, or D should include annual EGD, regardless of the absence of symptoms. The objective of our study departed from the former premise, since the presence/absence of EE on EGD is a determinant to diagram our pre- and postoperative strategy. Preoperative EGD findings allow the surgeon to select the right operation for the right patient; moreover, postoperative EGD offers the possibility of changing the strategy during follow-up if considered necessary for the patient.
Here we summarize the important aspects of our results:
1. Regarding GERD symptoms (a) The prevalence of GERD symptoms scaled from 33% to 44%. (b) GERD symptoms resolved in 41.6% of cases after LSG. (c) De novo GERD symptoms appeared in 36.9% of patients. (d) Significant correlation was found between the presence of postoperative GERD symptoms and EE (64.5% of patients complaining of symptoms had EE on EGD). (e) Symptoms were mild and showed good response to medical treatment in 80% of patients. 2. Regarding EE (a) EE rates significantly increased from 20.1% to 33.9%. (b) De novo EE was seen in 28.7% of patients. (c) 74% of postoperative EE were Grade A. (d) Around 45% of preexisting EE resolved after LSG. (e) Around 60% of moderate-to-severe EE resolved after medical treatment; the remaining 40% did not show progression of their disease. (f) At 18-month follow-up there was no progression to BE in any case. 3. Regarding HH (a) HH rate increased from 22% to 34.8%. (b) De novo HH was observed in 16.4% of cases. (c) Simultaneous repair was performed in 25% of the HH diagnosed preoperatively. Of those, 50% showed recurrence of their HH. (d) Almost 45% of patients with postoperative HH presented EE on EGD.
Conclusion
The prevalence of GERD symptoms, EE, and HH was increased after LSG. At 18-month follow-up, severity of esophagitis was mild, the majority of them being Grade A esophagitis. There was good correlation between manifestation of GERD symptoms and the presence of EE on EGD.
Footnotes
Disclosure Statement
No competing financial interests exist.