
Abstract
Abstract
Background:
Patients' selection for transanal endoscopic microsurgery (TEM) depends on diagnostic modalities; however, there are still some limitations in the preoperative diagnosis of rectal lesions, and in some reports, up to third of the adenomas resected by TEM were found to be adenocarcinoma; therefore, salvage radical resection (RR) remains necessary for achieving oncological resection. Salvage RR may encounter some technical problems as the violation of the mesorectum and the scar formation. In this study, we aimed to report the outcome in patients undergoing salvage RR in terms of morbidity and oncological results.
Materials and Methods:
Demographic and clinical data pertaining to patients undergoing RR following TEM between 2004 and 2014 were retrospectively collected.
Results:
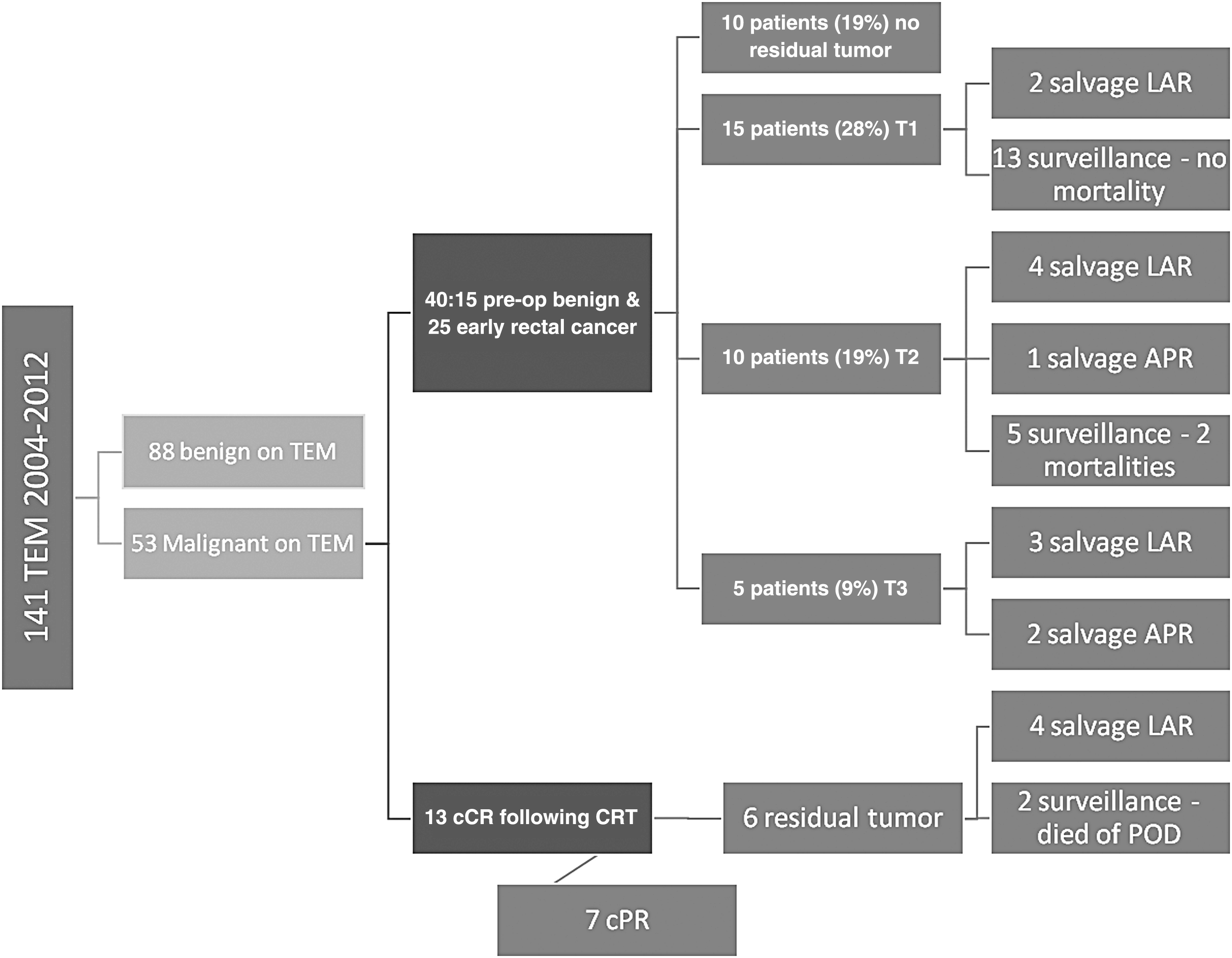
One hundred forty one TEM were performed in the study period, 53 (38%) for malignant rectal lesions. Indication for TEM: 15 (28%) benign adenoma, 25 (47%) early rectal cancer, and 13 (25%) had clinical complete response after neoadjuvant radiochemotherapy. Ten (19%) patients had no residual tumor in TEM specimen, 15 (28%) had T1, and 2 of them underwent salvage low anterior resection (LAR). Ten (19%) had T2, 4 had LAR, and 1 had abdominoperineal resection (APR). Five (9%) had a T3, 3 underwent LAR, and 2 had APR. Among the 13 (25%) after chemo-radiotherapy (CRT), 4 had salvage AR. The time from TEM to RR was 47 days (range32–70). Of 16 salvage surgeries, 8 (50%) were laparoscopic. The median operative time was 210 minutes (range165–360). Five patients had protective ileostomy. Rectal perforation occurred in 2 (12%) patients; both had a posterior location, one after CRT. Two (12%) postoperative small-bowl obstruction and three wound infections occurred. There was no perioperative mortality in any of the patients who underwent RR. The final pathology was no residual disease in 9, T3N1 in 1, T3N0 in 3, T2N1 in 1, and T2N0 in 2 patients. Eight (50%) had adjuvant chemotherapy.
Conclusion:
Laparoscopic total mesorectal excision following TEM seems to be safe, and with no negative impact of the completeness of the resection. The concern of intraoperative specimen perforation is real, and should be dealt with meticulous technique and careful dissection, particularly after CRT.
Introduction
T
Recently, several reports suggested a role for TEM in more advanced rectal cancer due to recent advances in chemoradiation therapy. Local excision by TEM is proposed selectively for T2 and T3 lesions when augmented by neoadjuvant or adjuvant therapy.5–7
Patients' selection for TEM depends largely on various diagnostic modalities, such as transrectal ultrasound, CT, and MRI. Unfortunately, there are still some limitations to the preoperative diagnosis of large rectal adenomas using these modalities, and in some reports, up to 26% of the adenomas resected by TEM were found, at the definitive pathological examination, to be invasive adenocarcinoma. 8 The accuracy of available diagnostic modalities in predicting nodal involvement is also distressingly low. 9 This is problematic because TEM does not include removal of regional LNs and therefore eliminates the ability to obtain important prognostic information or provide local control for patients with positive nodes.
Although some reports showed low locoregional recurrence in patients treated with adjuvant radiotherapy following TEM resection of T2 rectal cancer, 6 radical resection (RR), either by low anterior resection (LAR) or by abdominoperineal resection (APR) with total mesorectal excision (TME) after TEM, whenever definitive specimen pathology reveals “non early” rectal cancer with unfavorable histologic characteristics, remains indispensable for achieving acceptable oncological outcomes. 6
Full-thickness local excision by TEM of rectal cancer after a complete clinical response following neoadjuvant radiochemotherapy (RCT) is considered the best method to determine the pathological response of the tumor and correlates with a disease-free mesorectum in 94% of the times.10,11 On the contrary, poor pathological response with TEM following neoadjuvant RCT requires completion TME. 5
Salvage TME (sTME) following TEM is required in 4%–23% of patients due to locoregional recurrence, which may reflect the controversies surrounding the treatment of certain early malignant lesions, different indications for TEM, and matters of patient selection.9,12
Regardless of the increased morbidity performing the two procedures, completion TME may prove difficult due to the previous violation of the mesorectum and the scar formation. This may pose difficulty in maintaining the dissection in the correct surgical plain, which, in turn, may compromise oncological outcome. This is the main point of contention between authors who support the use of completion TME for unfavorable pathologic results following TEM versus those who support upfront radical resection.13,14
In this retrospective study, we aimed to report the outcome in patients undergoing radical rectal resection following TEM in terms of morbidity and oncological results.
Materials and Methods
The data of all patients with rectal tumor treated by TEM procedure at the department of Surgery Hasharon Hospital Rabin Medical Center were collected retrospectively.
Only patients whose pathologic examination of the specimen showed rectal cancer were included in the study. Patients who underwent radical rectal resection LAR or APR after the TEM procedure were also included. The full medical records of the patients were obtained and collectively reviewed and recorded.
In our department, patients were offered TEM if they had benign rectal lesions, or superficial adenocarcinoma arising from adenoma with negative LN. Patients were also offered TEM if they had a clinical complete response (cCR) and with disappearance of the rectal tumor after neoadjuvant RCT.
Patients were evaluated according to a regular protocol that included clinical examination with digital rectal examination, colonoscopy with biopsy, rigid proctoscopy, and endorectal ultrasound (EUS). For each patient, both the distance and the location of the tumor were assessed, as well as the tumor size. Distance was defined as the distance from the dentate line to the lower margin of the tumor. The location of the tumor was assessed because the patient should be positioned with the tumor downward during surgery.
Patients, who underwent preoperative chemoradiation therapy for advanced rectal cancer, were assessed for the tumor clinical response by digital rectal examination and rigid rectoscopy, and by EUS 4 to 6 weeks after the completion of the neoadjuvant therapy. Patients were also restaged before surgery with abdominal and pelvic CT, and some patients also had an FDG-PET. Patients who had no detectable tumor on rectal examination or rectoscopy were defined as having a cCR. Lesions reduced to small scars or ulcers were marked before surgery for accurate identification and localization.
Patients with cCR after neoadjuvant therapy underwent TEM instead of radical resection if they were considered to have prohibitive comorbidities, or those who refused to undergo an operation that carried the risk of stoma formation.
The procedure was performed with original Richard Wolf (Knittlingen, Germany) TEM equipment, under spinal or general anesthesia. The patients were placed in a prone jackknife or lithotomy position, depending on the tumor location. The tumor site was removed by excising the full-thickness rectal wall with a 1-cm margin around the tumor. The underlying mesorectal fat was included with the specimen. The specimens were pinned and marked for orientation by the surgeon. The rectal defect was closed primarily in a transverse manner with absorbable sutures.
All patients had a urinary catheter in place at the time of surgery, which was removed the day after surgery.
Postoperative pain management for all patients included orally dypirone or paracetamol, and oral narcotics (tramadol) on demand. Patients were allowed to resume eating the following day and were discharged from the hospital 2 to 3 days after the operation.
Patients were referred to radical rectal resection whenever pathology specimen of the TEM showed “non-early rectal cancer,” which included the following high risk features: pT1sm2-3, lymphovascular invasion, pT2, or pT3.
For rectal lesions located ≤10 cm from the anal verge, the surgery (open or laparoscopic approach depending on the surgeon's preference) was performed according to accepted TME principles, maintaining the integrity of the mesorectum down to the pelvic floor to achieve a meticulous clearance of the pelvis, while preserving the autonomic nerves. The decision to preserve the sphincters or complete an APR was based on the ability to achieve clear distal margins and to maintain a good functional outcome.
For high rectal tumors >10 cm from the anal verge, anterior resection of the rectum with partial mesorectal excision was performed, aiming for a distal margin of 5 cm below the tumor. An end-to-end anastomosis stapler was used to restore the continuity. A diverting ileostomy was commonly created after performing a low colorectal anastomosis, or after neoadjuvant RCT, or for higher anastomosis if technical difficulties or other factors suggested a high risk for anastomotic breakdown.
Patients were evaluated 2 weeks after the operation and were reexamined at 3-month intervals for the first 2 postoperative years, and every 6 months thereafter.
Clinical examination and rectoscopy were performed in each of the follow-up sessions. Metastasis workup also was performed periodically. Colonoscopy was performed at 2 years after surgery, and then every 3 years thereafter.
Data regarding demographics, perioperative evaluation, operative details of the two procedures, tumor characteristics, postoperative complications, follow-up period, and mortality were collected.
The local ethics committee of Rabin Medical Center approved the study protocol and the data collection.
Results
Between March 2004 and December 2014, 141 TEM procedures were performed in the Department of Surgery “B,” Hasharon Hospital. Fifty-three (37%) of the procedures were performed for rectal malignancy and were included in the study; 15 (28%) of them had a preoperative diagnosis of benign adenoma, 25 (47%) patients had early rectal cancer preoperatively, and 13 (24%) patients had cCR following neoadjuvant RCT therapy for locally advanced rectal cancer.
There were 29 (55%) males and 24 females (45%) with median age of 60 years (range 37–86). The mean tumor size was of 2.1 cm (0.5–4.5), and the distance of the lesion from the anal verge was 8.5 ± 3.5 cm.
The mean operative time for the TEM procedure was 105 minutes (with a range of 65 to 160 minutes). Hospitalization time was 3 days (range 2–5). Two patients had urinary retention postoperatively, which was treated with a catheter, and another patient developed pneumonia on the third postoperative day. No cases of rectal bleeding or suture dehiscence, or other major complications were observed.
The pathology of the TEM specimens showed that 10 (19%) patients had no residual tumor, and they were followed without further surgical interventions. Fifteen patients (28%) had a T1 carcinoma, 2 of whom had a submucosal invasion at the level of sm2 (15) and therefore underwent sTME surgery by LAR; 1 of these 15 patients had a T1sm3 and elected to undergo follow-up surveillance only. Ten patients (19%) had a T2 carcinoma, 4 had sTME by LAR and 1 by APR for involved margins; 2 of the remainder 5 patients who refused sTME surgery had died of progression of disease (POD). Five (9%) had a T3 after TEM, 3 had LAR, and 2 APR; 1 patient who underwent an sTME by APR and 1 who underwent an sTME by LAR for T3 after TEM, also received adjuvant chemo-radiotherapy (CRT). The other 13 (25%) underwent TEM after neoadjuvant RCT, 7 had a complete pathologic response at TEM; of the 6 who had residual disease, 4 had sTME by LAR and 2 elected to undergo surveillance and died of POD (Fig. 1).
Population study.
Overall, 16 patients had sTME surgeries, 8 were laparoscopic and 1 of them was APR. The time from TEM to TME was 47 days (range 32–70). The median operative time was 210 minutes (range 165–360), which was statistically significantly longer for laparoscopic versus open. Protective loop ileostomy was performed in 6 patients, 4 of them were planned for the ileostomy preoperatively since they had the TEM following neoadjuvant RCT. Five of the patients who had a protective ileostomy were operated laparoscopically. Perforation of rectal tumor site occurred in 2 (12%) patients who underwent sTME surgery by the open approach—one underwent an LAR with a diverting ileostomy and the other a planned APR. The location of the rectal perforation was posterior in both cases. Hospitalization time was 7 days.1,4–15 Two (12%) patients had an early postoperative small bowl obstruction, and 1 was operated. Two abdominal and one perineal superficial surgical site infections were noted. There was no perioperative mortality in any of the patients who underwent sTME surgery.
The final sTME pathology was no residual disease in 9 patients, T3N1 in 1 patient, T3N0 in 3 patients, T2N1 in 1 patient, and T2N0 in 2 patients. The surgical margins of the TME specimens were negative, and the average number of LNs harvested was 8 (range 4–13). Eight (50%) patients had adjuvant chemotherapy (Fig. 2).

Study outcome.
Discussion
Local excision by TEM is considered a valid alternative to the traditional surgical treatment of adenomas and low-risk (T1) rectal tumors. 1 However, it is certainly an oncologic compromise, in cases of more advanced and high-risk rectal lesions, for which rectal resection by TME is considered the standard of care. 13 Nonetheless, radical rectal resection carries a considerable postoperative morbidity when performed within a short period of time following TEM, and therefore, it is justifiable to opt for TEM instead.16,17
Occasionally, the pathologic result after TEM demonstrates an unfavorable pathology for local excision due to the high correlation with LN metastasis, as is with T2-3 lesions, T1sm2-3 lesions, lymphovascular invasion, or positive margins. In these cases sTME is indicated and can be performed either laparoscopically or through the open approach. The outcomes of sTME following TEM have not been studied comprehensively. We present our experience.
We observed that rectal perforation is certainly a risk when performing TME following TEM. Rectal perforation occurred in two cases (12.5%), one of them within LAR after neoadjuvant RCT at the site of the previous TEM resection, and the second case was an inadvertent perforation in APR. Fortunately, the final pathology report in both was no residual tumor and with negative LNs. Both cases of perforation were with posterior rectal wall TEM resection, and both were after an open rectal resection procedure. Levic et al. 18 report that 5 of 25 patients experienced perforation after sTME following TEM for unfavorable pathology. None of the patients in that series underwent neoadjuvant RCT. One patient experienced perforation at laparoscopy and the remaining 4 underwent open surgery. In total, 6 (24%) of the 25 patients in this group had the procedure performed laparoscopically. Of the perforations, 3 patients perforated the posterior bowel wall and 2 patients perforated the residual tumor field. The surgical technique used for the patients with perforation into the peritoneal cavity was APR in 2 patients and LAR in 1 patient. All three were open procedures. All 25 cases in this series were matched for stage and comorbidities to cases that had undergone primary TME (pTME). No significant differences in postoperative complications were found on statistical analysis. 18 Van Gijn et al., in their series of 59 patients who underwent sTME after TEM, some of which had neoadjuvant CRT, do not report a perforation rate, but do report that perforations into the original operating field regularly occur in their experience due to fibrotic changes to the bowel wall, which might allow microscopic tumor spill. 19
The risk of perforation of the rectal wall or the tumor is real in TME following TEM, especially after neoadjuvant CRT. We posit that laparoscopy may reduce the risk of perforation due to better visualization and a more meticulous dissection of the mesorectum.
In our trial, the average number of LNs harvested during sTME was 8 (range 4–13). Levic et al. who compared sTME following TEM to pTME found no statistical difference in the number of LNs harvested: in the sTME, 12 LNs3–23 versus 10 LNs3–21 in the pTME group. 18 Morino et al., who compared 17 patients who underwent laparoscopic TME following TEM for unfavorable pathology to a matching group of patients who underwent a primary laparoscopic TME, report a median of 11 LNs harvested in the first group versus 12 LNs harvested in the latter group, which did not show a statistical difference. 20 Our experience and that of previous authors on the subject suggests that the number of LNs harvested during sTME following TEM is comparable to that of pTME.
Positive circumferential radial margins (CRM) have been previously demonstrated to be associated with a higher local recurrence rate, as reported by Balch et al. who show that with CRM >1 mm, the recurrence rate after TME is 5%, but when CRM <1 mm, the local recurrence rate is 20%. 21 Levic et al. report no difference in the rates of positive CRM in both the group that underwent sTME following TEM and the pTME group. Each of the groups that consisted of 25 patients had 1 positive CRM. 18 Morino et al. report no CRM involvement in either the sTME following TEM group (n = 17) or the pTME group (n = 34). 20 Our trial showed negative circumferential margins in all cases. The conclusion to be drawn is that the risk of weakening the rectal wall and compromising the mesorectal fascia after a previous TEM procedure can lead to an increased risk of positive CRM, compromising oncological safety.
The completeness of the mesorectal fascia (CMF) during TME dissection has been considered an indicator for the quality of resection. 22 However, the scar formation in the rectal wall after the full-thickness resection by TEM may pose difficulty for correct interpretation of this indicator; in actual fact, only 4 patients in our group had a CMF report in their pathology. Morino et al. report lower rates of complete mesorectal excision in TME performed after full-thickness TEM, probably secondary to traction on the rectum during the mobilization that may cause a tear in the mesorectum. 20 The CMF was also evaluated by Levic et al. who report that 6/25 patients in the sTME following TEM group and 4/25 patients in the pTME group did not have this element in the final pathology report. 18
The completeness of the mesorectal excision in sTME following TEM should be interpreted with caution and seen alongside through comprehensive pathological parameters of the specimen.
The rates of no residual disease found in specimens of sTME in our study were 9/16 (56%) and appear to range from 48% to 53% in the other 3 studies cited here.17,20,23 These patients are being overtreated, which reflects the still relatively low accuracy of EUS and MRI in the evaluation of the rectal wall invasion and LN involvement before and after TEM, even in high-volume centers.
The rate of APR, and end colostomy, during sTME in our study was comparable between the open approach 2/8 and the laparoscopic approach 1/8. Van Gijn et al. who compared 59 patients who underwent sTME following TEM for unfavorable pathology and compared them to 881 patients from the Dutch TME trial who underwent pTME, showed a significantly higher rate of colostomy creations in the sTME group. 19 They pose that a TEM procedure results in a scar that has to be totally resected during sTME, likely leading to a more distal resection margin than would be necessary in primary TME surgery. This factor combined with the fact that a reoperation is generally technically challenging might explain the higher frequency of colostomy creation in the sTME group in that trial, in comparison to the pTME. In the study by Morino et al., the sTME group too underwent APR with end colostomy more frequently than the pTME group. 20 It appears that the odds of performing an end colostomy in sTME increased in comparison to pTME, but laparoscopy does not increase this rate.
The small number of patients in this study may result in an overestimation of the results and an increased risk of type II errors. Other limitations of our study are the follow-up time and the retrospective nature of the study. The long accrual periods in our trial introduce variability in the perioperative care as it evolves over the years. Another limitation in our study is the lack of randomization to laparoscopic versus open approach. The approach was based on surgeon preference and therefore subjects the study to a selection bias. Last, diagnostic modalities were not uniform for all patients and those have previously shown to have a significant impact on the choice of surgical approach.
To the best of our knowledge, this is the first trial that reports outcomes of sTME following unfavorable pathology on TEM for early rectal cancer, stratified by the open versus the laparoscopic approach. We conclude that laparoscopic rectal surgery following TEM is safe, and with no negative impact on the completeness of the resection. Nonetheless, the concern of intraoperative specimen perforation is real and should be dealt with meticulous technique and careful dissection, particularly after neoadjuvant CRT.
Footnotes
Disclosure Statement
No competing financial interests exist.