
Abstract
Abstract
Background:
Surgical site infections (SSIs) remain a morbid and costly complication in abdominal surgery. Topical antibiotic delivery via intraoperative irrigation and barrier wound protection are strategies for preventing SSI. We tested the safety and efficacy of a novel wound protector device with an integrated fluid irrigation platform in a porcine model.
Methods:
A simulated colorectal resection model was designed and performed on adult female pigs with a standardized concentration of 109 colony-forming units (CFU) of Escherichia coli administered to the wound site in 10 mL of normal saline (n = 7). The device was tested intraoperatively with and without irrigation with gentamicin-containing irrigant solution. Swab and tissue samples were obtained in addition to peripheral blood samples. Quantitative culture analysis was performed in addition to histological and immunohistochemical analysis and gentamicin concentration measurements.
Results:
There were no adverse events observed in the animals. Tissue protected by the device yielded exponentially lower levels of E. coli growth compared to exposed tissue, with a mean 1 × 102 CFU/swab. Use of the device, both with and without irrigation, was associated with an exponential reduction in quantitative bacterial load compared to the control wounds with no device, with limited growth after wound closure in the pigs receiving irrigation. Histology and terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL) staining analysis revealed no significant damage to tissue. Serum gentamicin levels remained below the clinical threshold and decreased over time.
Conclusions:
This in vivo study suggests safety and efficacy of a novel device for the prevention of intraoperative wound contamination.
Introduction
S
There are many clinical variables that have been shown to increase the risk of SSI, many of which are related to the patient and hospital or operating room environment. However, contamination of the incisional wound surface by pathogenic bacteria is likely the most important because of its direct causal relationship; put simply, an infection cannot occur without the presence and invasion of a pathogenic microorganism. Thus, by extension, efforts to counteract or limit contamination should improve the likelihood of normal wound healing and prevention of SSI.
Two strategies that have demonstrated promise in preventing or counteracting the effects of contamination in the intraoperative period are barrier wound protection and topical antibiotic delivery. Barrier wound protection has been shown to reduce the load of local bacterial contamination at the time of wound closure, which has translated to decreased incidence of SSI in abdominal surgery.4–7 Topical antibiotic delivery, specifically intraoperative topical antibiotic irrigation, has also been shown to decrease SSI risk,8,9 but consistent benefits from topical antibiotics have varied widely depending on the methods of application and the specific antibiotic used. Both strategies depend on proper use and deployment, often difficult to ensure intraoperatively due to the wide variability in surgical practices, techniques, and scenarios. We invented a novel device that provides the ability to combine and better standardize both anticontamination strategies in one platform. This device, which we call the CleanCision™ (Prescient Surgical, San Carlos, CA), is a wound protector and retraction device with an integrated fluid irrigation and delivery platform (Fig. 1).
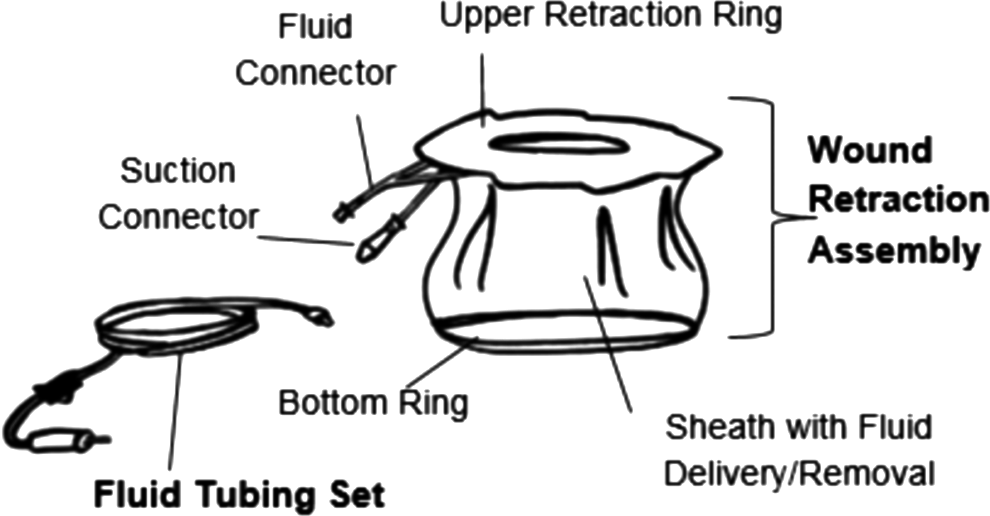
CleanCision™ Wound Retraction and Protection System.
We designed an in vivo large animal model of a simulated open colorectal operation and tested the CleanCision device's safety and efficacy. The device was tested for efficacy with the following two hypotheses: (1) use of the CleanCision (both with and without irrigation) is associated with a significant decrease in bacterial contamination of the protected wound at the end of a simulated colorectal operation; and (2) use of the CleanCision with a clinically relevant dose of gentamicin irrigation delivered through the device is associated with a significant decrease in bacterial tissue concentration that is sustained 4 hours after the end of a simulated colorectal operation. The study also evaluated the safety of the device with the following two hypotheses: (1) use of CleanCision (both with and without irrigation) does not lead to an increased level of local tissue damage and cell death at the wound edges; and (2) topical irrigation for 4 hours of a clinically relevant dose of gentamicin delivered through the CleanCision is associated with minimal and clinically insignificant systemic absorption of gentamicin.
Materials and Methods
Animals
This study was performed at an accredited commercial animal research facility (PMI, San Carlos, CA). Seven adult female pigs (Sus scrofa domestica) weighing between 50 and 70 kg were housed at the facility and subjected to the study. The experimental protocol was approved by the facility's Institutional Animal Care and Use Committee (IACUC). All animal procedures were performed under conditions described in the guidelines for care and use of laboratory animals as published by the National Institutes of Health as well as the facility's Association of Assessment and Accreditation of Laboratory Animal Care-accredited standard operating procedures.
Simulated open total abdominal colectomy, experimental groups
Swine were placed under general anesthesia and monitored for the duration of the experimental protocol (Fig. 2a). The abdomen was shaved, prepared with chlorhexidine solution, and the surgical site was draped in a sterile manner. A 12-cm periumbilical midline incision was made and the abdominal cavity was entered.
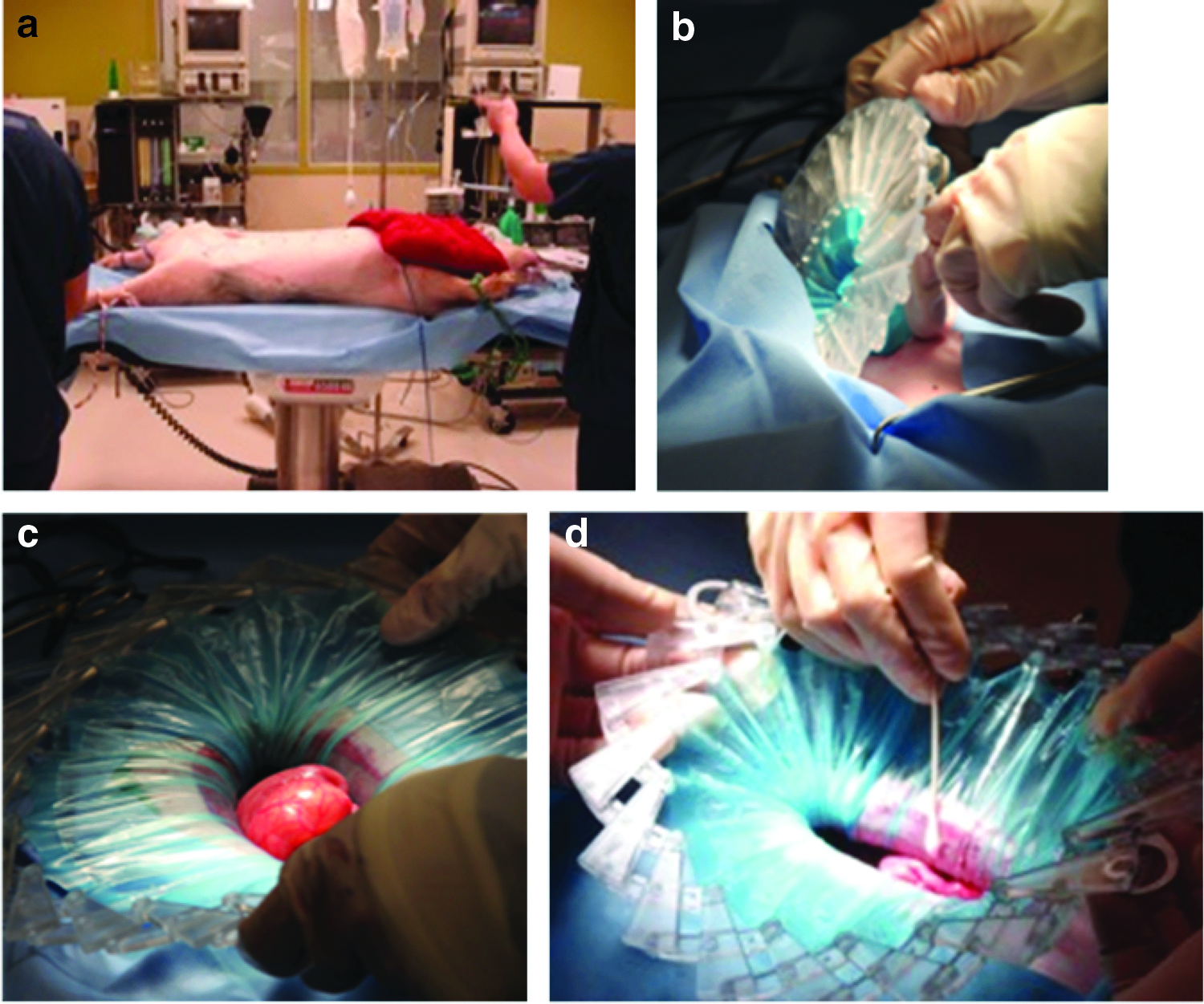
Once the incision was made, the CleanCision was placed in the wound for animals treated with the device (Table 1) and expanded to retract the wound edges (Fig. 2b, c). Wounds were retracted for ∼2.5 hours to simulate a prototypical length of time for colonic dissection.
Estimates of the inoculum of bacteria released during colorectal surgery typically range from 106 to 108 organisms per gram.10,11 To simulate contamination that occurs during colonic division and anastomosis, a gentamicin-sensitive Escherichia coli suspension (American Type Culture Collection, Manassas, VA) at a standardized concentration of 109 colony-forming units (CFU) in 10 mL normal saline was dripped onto the central colon in all pigs. The colon was grasped with a Babcock clamp and exteriorized out of the abdomen and allowed to rest on the superior, left, inferior, and right aspects of the incision for 20 minutes each.
In a single control pig, no CleanCision device was used (n = 1). Among the other animals, one experimental group (E-NF group, n = 3) had the CleanCision device used during the procedure as a barrier protection device only, without any irrigation delivered through the device. In the other experimental group (E-F group, n = 3), 240 mg gentamicin sulfate (Butler Schein, Dublin, OH) in 1 L normal saline solution was delivered through the CleanCision device to the circumference of the retracted wound at a rate of ∼5 mL/min. The irrigant fluid was delivered via gravity drainage from an IV bag hung from a 6 ft IV pole, and retrieval of fluid from the device was achieved via wall suction into a standard surgical canister. The fluid delivery and retrieval mechanisms are integrated into the CleanCision through separate tubing connections. The total irrigation time for this group averaged ∼4 hours, ∼2.5 hours before inoculation of bacteria and 1.5 hours following inoculation.
At the end of this 4-hour period, the abdominal cavity was then irrigated with 1 L of normal saline at the end of the simulated operation, and the CleanCision was removed. Fascial closure was performed with a 0 PDS monofilament running suture and the skin was closed with staples.
Specimen collection
Specimens were gathered at two primary time points: at device removal before fascial closure (denoted as Time 1) and 4 hours after wound closure when the incision and fascia was reopened (denoted as Time 2). During the 4 hours before reopening of the incision, the pigs were kept anesthetized.
At each time point, 1 × 1 cm full-thickness abdominal wall tissue blocks (from skin to peritoneum) were obtained from the midpoint for the incision from opposite sides of the incision. The histology/immunohistochemistry (IHC) samples were placed in 10% neutral buffered formalin. In the group receiving the irrigation fluid, peripheral blood samples were drawn at each time point for measurement of gentamicin levels.
Culture analysis for E. coli from tissue and swab samples
Just before device removal, cotton swabs were taken at two distinct locations (Fig. 2d). A “protected swab” sample was taken throughout the entire circumference of the protected wound surface on the side of the sheath that is directly contacting the incision. An “exposed swab” sample was taken along the entire circumference of the inner exposed sheath, presumably where most of the contact with bacteria would occur.
Quantitative culture analysis was performed on both the abdominal wall tissue blocks and the swab samples (MicroQA, Concord, CA). The tissue and swab samples were vortexed in phosphate-buffered saline and serially diluted onto plates in duplicate on trypticase soy agar (TSA) media. The plates were incubated at 30°C–35°C for 18 hours. E. coli colonies were identified and enumerated. The standardized concentration of the original sourced E. coli at 109 CFU/mg was obtained as a positive control. In addition, a tissue sample taken from the wound edge of the control pig during the early part of the experimental protocol before E. coli contamination was used as a negative control.
Histology and IHC analysis of tissue samples for cell viability
Histology and IHC analysis was performed for the tissue blocks (HistoTox Labs, Boulder, CA). Tissues were fixed in 10% neutral buffered formalin. Medial and lateral orientation was maintained and assured on glass slides. Sections stained with hematoxylin and eosin (H&E) were evaluated by light microscopy for identification of cellular necrosis. Sections processed with a terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL) assay kit were examined for cellular apoptosis via fluorescent microscopy.
Serum gentamicin concentration measurements
In the group receiving gentamicin irrigation fluid, peripheral blood samples were drawn at the time of device removal (Time 1, before fascial closure) and at the time of wound reopening 4 hours after the initial closure (Time 2). The blood was collected in serum separator tubes and centrifuged, and the serum was isolated. The samples were serially diluted and analyzed with an indirect competitive gentamicin ELISA kit (Creative Diagnostics, Shirley, NY) for quantitation of gentamicin concentration.
Statistical analysis
Quantitative culture results are expressed in mean ± standard deviation. Statistical comparisons of quantitative culture results were performed by Student's t-test. Significance was based on a value of P < .05.
Results
Quantitative swab cultures of exposed versus protected side of the CleanCision at the time of fascial closure
At the time of fascial closure (Time 1), swabs of the exposed side of the device sheath led to high levels of E. coli growth over the course of the procedure, with a mean of 1.68 ± 1.71 × 104 CFU/swab. The protected side yielded exponentially lower levels of E. coli growth, with a mean of 1.00 ± 0 × 102 CFU/swab. Three out of four protected-side samples showed no growth at maximum dilution; therefore, the values for these three samples were documented as 1 × 102 CFU/swab, the minimal detectable limit for this assay. The remaining fourth sample, from an animal receiving CleanCision without irrigation, demonstrated 1 × 102 CFU/swab. The difference between the two groups approached statistical significance (P = .099).
Quantitative tissue cultures over time after use of the CleanCision
Use of the CleanCision device intraoperatively, both with and without irrigation, was associated with an exponential reduction in quantitative wound culture compared to the control with no device. Both experimental groups using the CleanCision had minimal bacterial growth at Time 1 (2.04 ± 0.61 × 102 CFU/g in E-NF versus 1.25 ± 1.55 × 102 CFU/g in E-F, P = ns). However, the group without irrigation (E-NF) developed exponential bacterial growth after Time 2, 4 hours when the wound was reopened (2.60 ± 1.41 × 104 CFU/g), compared to Time 1. This difference was statistically significant (P = .041). The group that received the antibiotic solution (E-F) exhibited a durable, sustained suppression of bacterial growth at both time points (2.08 ± 3.01 × 102 CFU/g). The difference between the E-F and E-NF groups at Time 2 was statistically significant (P = .041). The results are summarized in Figure 3.
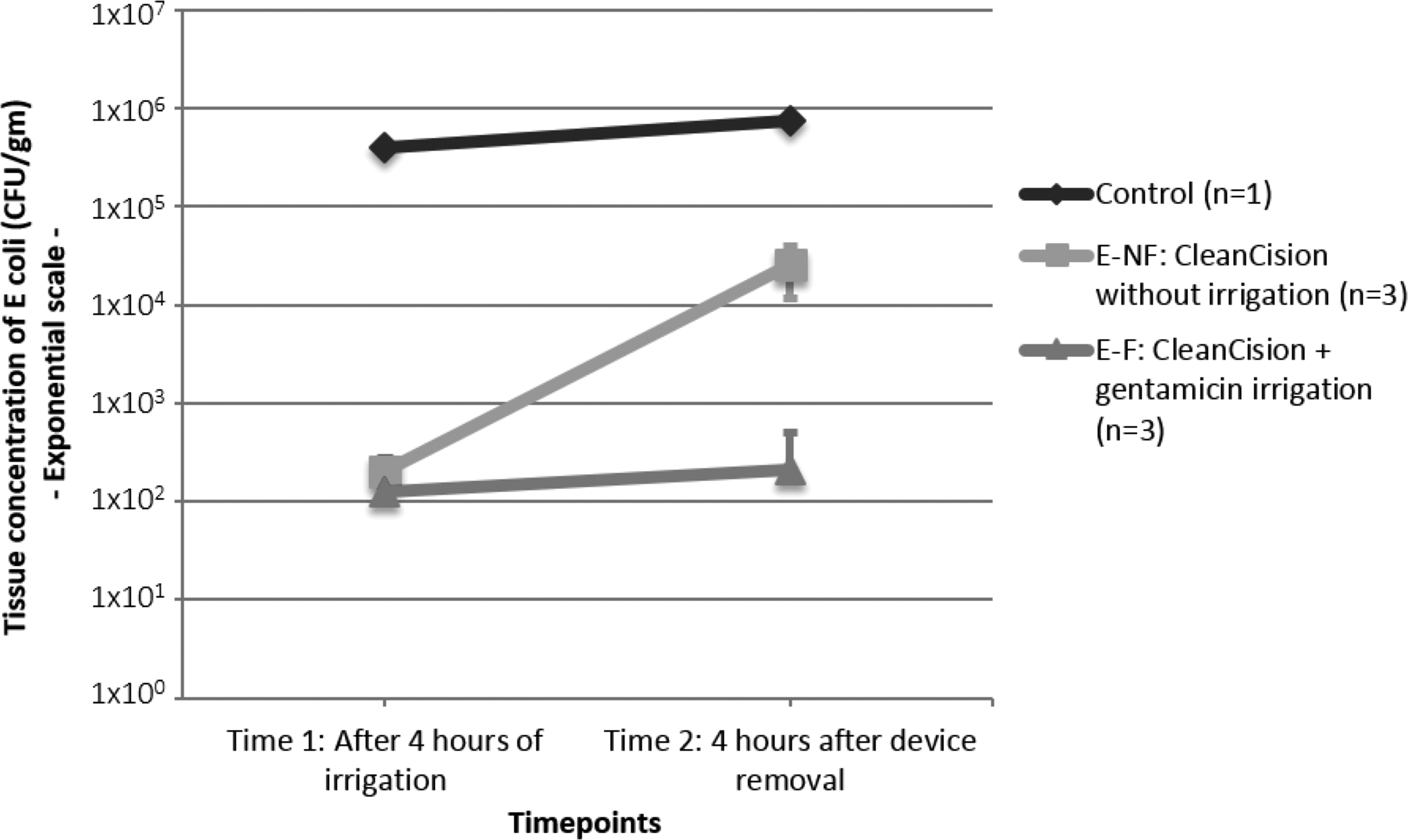
Quantitative bacterial tissue culture over time with and without use of CleanCision. CFU, colony-forming units.
Both H&E staining (Fig. 4) and TUNEL assays were performed on the tissue blocks from the time of fascial closure as well as the reopening of the wound. There was no significant evidence of local tissue necrosis or apoptosis on the wound edges in any of the study groups, and there were no significant differences in the pattern of staining or fluorescence among the control, E-NF, and E-F groups.

Representative H&E sections of tissue blocks taken at the time of fascial closure from pigs in the
Serum gentamicin concentrations over time after irrigation through CleanCision
We set a clinically relevant lower threshold for serum gentamicin concentration at 1 mg/L, based on literature and clinical pharmacy guidelines. In the group receiving topical antibiotic, systemic gentamicin absorption remained nearly undetectable and began to decrease over time. The mean serum gentamicin concentrations were 0.24 ± 0.11 mg/L after 4 hours of irrigation (Time 1) and 0.10 ± 0.05 mg/L 4 hours after device removal (Time 2) (Fig. 5).

Serum gentamicin levels over time after topical delivery through CleanCision.
Discussion
SSI remains a common, morbid, and costly problem, and probably the single highest subset comes from incisional SSIs in clean-contaminated abdominal operations such as colorectal resections. The best and most rigorous estimates of SSI following colorectal surgery range from 10% to 30%, and most would agree that the “real” rate is probably in the 10%–15% range.12–15 SSI has been shown to increase hospital resources and increase inpatient costs by up to $17,000–$20,000.2,14 There have been many efforts along multiple fronts to try to stem this tenacious problem, from design of new drugs or devices, increasing the applicability of minimally invasive surgery, and improving adherence to perioperative care pathways. The diversity of approaches perhaps reflects the fact that the development of SSI is thought to be a multifactorial process with numerous risk factors that include the infecting microbe, the patient/host, and the environment. 16
Despite all of these efforts, SSI has persisted. Our simple hypothesis is that this failure is largely because the amount of pathogenic bacterial load left on the incisional wound remains too high for the host's immune system to keep in check during the wound healing process. Thus, a more effective anticontamination method working at the local incision level should eliminate much of the bacteria, which by definition are the primary causative factor for SSI. We believe that our hypothesis is supported by the literature on barrier wound protection and topical antibiotic irrigation. The studies that do not reflect a benefit from these measures appear to have challenges with heterogeneity in study design, lack of technical standardization, and possibly poor compliance. 17 Despite these negative reports, the methods of wound isolation and antibiotic irrigation have been found to have merit as anti-SSI strategies on meta-analysis.4–8 The CleanCision device was designed to be the first device to integrate both strategies in a standardized manner and in an easy-to-use intraoperative device.
In this preclinical surgical contamination study in an acute in vivo pig model, the CleanCision was shown to provide effective and sustained protection to the incisional wound against bacterial contamination due to both barrier control and intraoperative irrigation with antibiotic solution. Use of the CleanCision led to a dramatic decrease in bacterial growth on the protected wound, in comparison to the exposed sheath component of the device. The CleanCision effectively reduces bacterial wound contamination when measured at the end of surgery, with or without irrigation delivered through the device. Prevention of bacterial contamination was further augmented with the delivery of an antibiotic-containing solution through the device's wound irrigation function. Microbiological results suggest that the use of the CleanCision in association with delivery of a clinically appropriate, common surgical antibiotic solution (gentamicin) through its irrigation mechanism leads to a significant, sustained reduction in bacterial colonization when measured up to 4 hours after the end of the surgical procedure.
In addition, these results demonstrated safety of the CleanCision device with and without antibiotic as measured by parameters at the local tissue as well as systemic absorption levels. CleanCision's wound retractor functions were shown to be safe based on histological and immunohistochemical examination of the incision edges. Topical delivery for 4 hours of a clinically appropriate dose of gentamicin solution did not lead to a clinically significant level of systemic antibiotic absorption; therefore, a higher local dose of antibiotic may be administered with a markedly decreased risk of systemic toxicity.
There were a number of limitations to this study. First, this is an in vivo animal study, which by nature provides surrogate data for the clinical setting and may not be reproducible in human subjects. Further investigation in either or both preclinical and clinical trials would be necessary to more definitively make conclusions on the CleanCision's effects on contamination and SSI prevention. Second, the procedure was highly controlled with a single specific antibiotic targeting a susceptible organism, which may not perfectly reflect clinical scenarios. This limitation was inherent because the study was designed to prove the concept of the device's mechanism, and future studies would evaluate its effects on multiple organisms and using different approved surgical irrigation solutions. Third, the type of preincision systemic antibiotic administered may not have adequately covered the organisms in abdominal surgery. Further studies are necessary to determine the degree of effect of the CleanCision in the presence of appropriate systemic antibiotics, and indeed whether its use could eliminate the need of systemic antibiotics entirely in selected cases.
In conclusion, this proof of concept study in swine with a single antibiotic in a simulated high-risk abdominal surgical procedure supports the dual design of barrier protection and wound irrigation with antibiotics. This work warrants further exploration and yields promise for the safety and efficacy of this device in humans for the prevention of SSIs.
Footnotes
Acknowledgments
The authors acknowledge Lisa Claude, MS, for her assistance in preparing study data and materials for manuscript submission; and Laura Healy, DVM, PhD, for her assistance in histology and IHC. NSF SBIR Phase I grant ID 1345470; Fogarty Institute for Innovation.
Disclosure Statement
Insoo Suh: cofounder, stock interest in Prescient Surgical, Inc.; Sarah Long: none; Jonathan Coe: cofounder, employee, stock interest in Prescient Surgical, Inc.; Jeremy Koehler: cofounder, employee, stock interest in Prescient Surgical, Inc.; Donald Fry: scientific advisory board member for Prescient Surgical, Inc., stock interest in Prescient Surgical, Inc.; Mark Welton: cofounder, stock interest in Prescient Surgical, Inc.