
Abstract
Abstract
Purpose:
The learning curve is an important method of assessment of progression in the use of a new technique or device and, in the field of robotic surgery, is most commonly described for individual procedures, often concentrating on console time and outcomes. We contemplated whether a learning curve of the similar nature and duration was exhibited in the procedure-independent variable of docking time.
Materials and Methods:
The time from first incision to end of robot docking was found for a single surgeon's first 55 robotic cases, which encompassed a range of pediatric urological procedures. Raw and cumulative summation (CUSUM) data were found and plotted, with learning- and maintenance-phase times compared statistically.
Results:
A classical learning curve of ∼30 cases was found with a statistically significant reduction in time between learning and maintenance phases.
Conclusions:
A learning curve of similar nature and duration to procedure-specific analyses was found for docking time. The variability of port placement and robot positioning for multiple procedures further increases the significance of this result.
Introduction
T
The rapidly expanding field of robotic surgery has resulted in a large amount of learning curve data for both skills exercises and operative techniques, but the hallmark of such articles relates to temporal benefits. There is limited information available on the number of procedures that should be performed for the learning curve to have been completed, whether this relates to outcome or parity of operative time between laparoscopic and robotic procedures. Crudely, this appears to lie between 15 and 50, but can be higher depending on the type of operation and previous experience of the surgeon.1–4
The literature is replete with examples of procedure-specific advances within robotics but less well represented by procedure-independent variables, which are equally important. These factors are often removed from analyses so as not to distort the primary outcome measure of console time, which is the time it takes to perform the procedure. 5
One such variable, the knife-to-skin (KTS) to docking time, represents the duration between the first incision and the end point of the docking procedure. This is not the same period defined as docking time in the adult literature, which describes the time after final port placement to sitting at the console to begin the procedure. Port placement and angulation, adequate insufflation, robot positioning, and docking are all key factors that make the difference between a straightforward operation and one complicated by poor view or clashing instruments and so contributed to the data in this study.
We present our prospective data for this variable for the first 55 robotic cases performed by a single surgeon at our institution to discover whether it also demonstrated a learning curve. In addition to raw timing data, cumulative summation (CUSUM) was analyzed. CUSUM, first described by Page in 1954, 6 is a well-established method to represent data from consecutive procedures, transforming the variability of raw data into a cumulative sum of differences between each value and the mean. 2 A perfect learning curve would follow a bell-shaped curve pattern, with the upward slope (learning phase) representing the time during which outcomes exceeded the mean (i.e., the procedure took longer) and the downward slope (maintenance phase) representing the time wherein the procedure took less time than the mean to achieve proficiency when the graph is continuously declining or maintained at 0.
Materials and Methods
Interval timings for each phase of the surgeon's first 55 consecutive robotic procedures were prospectively collected, including positioning of the patient, KTS, insertion of first port and all ports, time of docking, start and end of robotic procedure, robot undocking time, and closure. Procedures were carried out throughout by the same experienced laparoscopic surgeon (R.S.) on the Da Vinci Si three-armed robotic system, with senior trainee assistance and a team familiar with robotic surgery. The procedures included pyeloplasty (20), nephrectomy (20), Mitrofanoff (4), and other (9—heminephroureterectomy, varicocele ligation, and second-stage orchidopexy). Only the orchidopexy patients (2) had previous laparoscopic surgery for the first stage clipping of vessels. The first port placed under direct vision was the 12 mm umbilical camera port, secured with a 2/0 polydiaxonone suture purse string suture, and, after insufflation of the abdomen, two further 8 mm ports were placed under internal observation in the appropriate positions. The time taken between the first incision (KTS) and robot docking was calculated for each case and the mean was found. Raw data were plotted and the trend line is shown. CUSUM was calculated as described previously using the internal control of mean time and the observed-minus-expected (mean) method 2 and was plotted. Mean times pre- and postlearning curve peak were compared using student's t-test.
Results
Procedures performed are shown in Table 1 and completed successfully with no conversion to laparoscopy or open approach. Patients were aged between 1 and 15 years. Mean weight of the patients in this series was 24.07 kg (range 9–65.5 kg). Docking time showed wide variability for the first 30 cases but then became reproducibly consistent. The trend line shows a steady decline in time taken to dock as experience increased (Fig. 1). CUSUM data demonstrate a bell-shaped curve with maximum peak at case 29, before a smooth decline toward proficiency (Fig. 2). There was a steep learning curve to case 5, which flattened and undulated toward the peak and a steep decline toward proficiency interrupted by a flattening of the curve during cases 36–48. Mean KTS to dock time up to case 29 was 23 and 15 minutes from cases 30 to 55 (P < .0001). No intraoperative complications occurred in this series.
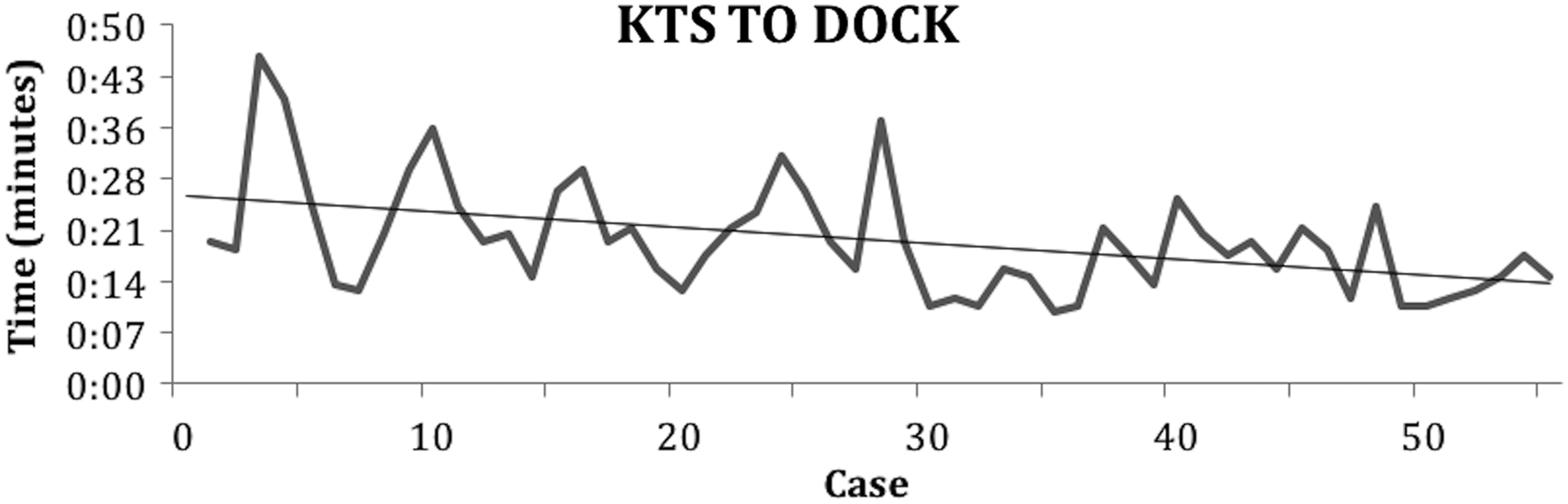
Raw data showing time taken from first incision to end of robot docking. KTS, knife-to-skin.
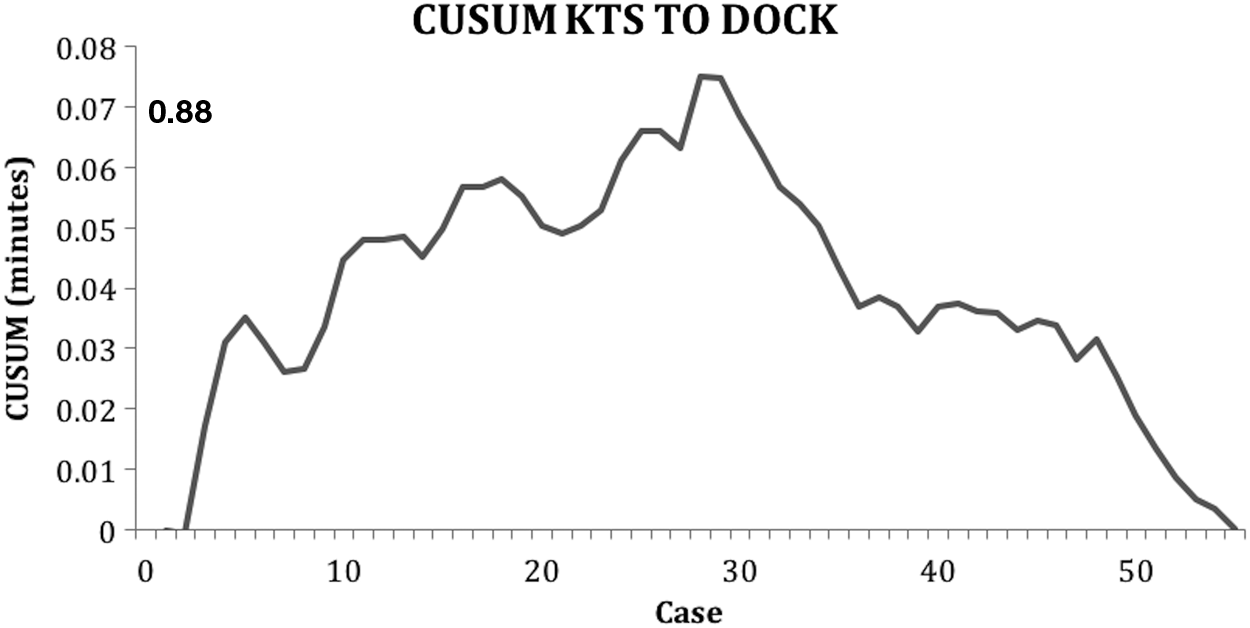
CUSUM data showing learning curve of docking time. CUSUM, cumulative summation.
Discussion
These results show that the technical components of robotic surgery that are common to all procedures also demonstrate a learning curve that is comparable in number to that of procedure-defined curves at ∼30 cases. Our data show a progressive improvement in duration from KTS to robot docking, but the CUSUM chart is helpful in confirming what appears to be a reduction in variability of duration shown in the latter stages of Figure 1.
Some authors have described a temporal learning curve in as few as two procedures, 7 and so it is of little surprise that an extremely rapid curve of 5 cases should exist with an experienced laparoscopic surgeon, before it flattens as the more complex difficulties associated with a change in practice can be fully corrected.
The interruption of what is a steep decline toward proficiency is interesting. A new procedure was introduced during this time but performed only twice, and these operations fell within a period of frequent robot usage. It may be explained by the surgeon attempting to further refine the technique as his confidence grew, thus increasing the time taken, but then quickly re-entered a rapid decline toward proficiency.
Another factor that makes this result impressive is that procedure-based learning curves inherently describe the same steps, including preparing the robot in the same scope-anatomy-console arrangement, but this work describes multiple different procedures with variable laterality and robot arrangement. One could postulate that the CUSUM curve would be closer to the perfect bell shape had this study been performed for a given procedure, but the experience between such cases would further bias the learning curve toward a more favorable result.
It is also important to note that the docking time does not reflect entirely on the surgeon, but in fact relates to the learning curve of a team, as successful positioning and operation of the device are in large part to the highly trained theater staff whose experience grows with each case along with the surgeon.
Conclusion
We believe that the skills required for robot surgery should begin with the basics, and meticulous planning of correct port placement and the placement of the robot for docking are key components that affect the success of any procedure. The need for special training to meet defined standards and requirements is essential for safe robotic practice. 8 This learning curve, which mirrors that observed for the procedures themselves, is a good benchmark of competence when using these new devices.
Footnotes
Acknowledgments
The authors sincerely thank for the professionalism and support given by the robotic theater team: Tony Loftus, Matt Millott, Maureen Westgarth, and Howard Korer.
Disclosure Statement
No competing financial interests exist.