
Abstract
Abstract
Purpose:
This study was designed to introduce a new surgical innovation, referred to as the “Longtan modification,” for cases with parastomal hernia (PSH) following intraperitoneal sigmoidostomy, and to assess the safety and feasibility of this procedure.
Methods:
Between January 2013 and June 2016, a total of 26 consecutive cases with PSH successfully underwent this procedure. The patient demographics, surgical outcomes, stoma-related complications, and the stoma function were collected and analyzed.
Results:
Mean diameter of the hernia ring was 7.6 cm, mean operation time was 94.2 minutes, and mean intraoperative blood loss was 18.0 mL. The mean period of postoperative hospitalization was 4.4 days while the mean hospitalization cost was only $3,750 USD. There were no severe complications such as postoperative hemorrhage, ischemic necrosis, peritoneal infection, or intestinal obstruction, although one case suffered from postoperative infection at the site of incision. None of the cases had a recurrence of PSH during the follow-up period. In addition, the stoma functioned efficiently and appropriately following the Longtan modification.
Conclusion
: Overall, the Longtan modification appears to be an effective and economical surgical innovation for cases with PSH following intraperitoneal sigmoidostomy.
Introduction
R
Intraperitoneal sigmoidostomy is the most common surgical method for single lumen sigmoidostomy, while parastomal hernia (PSH) is the most common long-term complication, with a reported incidence of 45%–60%.4–6 PSH may exert an adverse influence on the quality of life, including skin irritation, stoma appliance problems, stoma site discomfort, abdominal pain, and even intestinal obstruction.4,7 Although various techniques and materials have been studied and reported to prevent and repair PSH, the recurrence rate still remains high.4,8–10
Extraperitoneal sigmoidostomy has been used for rectal cancer cases undergoing abdominoperineal resection in the National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College since 2011. As a result, we have found that extraperitoneal sigmoidostomy can clearly reduce the incidence of PSH. From January 2013, we have developed a method of seaming the rectus abdominis fascia and extraperitoneal sigmoidostomy in situ as a therapy for PSH. We named this innovative surgical method the “Longtan modification” because of the beautiful Longtan Park close to our medical institution. In this article, we aim to introduce and analyze the outcomes of this new surgical innovation.
Patients and Methods
The study was approved by the Ethics Committee of the National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College. Moreover, the study conformed to the ethical standards of the World Medical Association Declaration of Helsinki.
The inclusion criteria were as follows: (1) bulgy mass around the stoma could be clearly identified by physical examination and became larger when standing or increasing abdominal pressure; and (2) the abdominal contents of the hernial sac were verified by computed tomography (CT) scan. The advantages and disadvantages of the Longtan modification was explained to patients in detail and the patients themselves chose to proceed and provided informed consent.
Between January 2013 and June 2016, a total of 26 consecutive cases with PSH successfully underwent the Longtan modification. All of these cases underwent abdominoperineal resection and intraperitoneal sigmoidostomy, and no signs of recurrence were evident on CT scan and colonoscopy examination. Preoperative mechanical bowel preparation was performed using polyethylene glycol electrolyte powder. Preventative antibiotics were administered by intravenous drip 30 minutes before the operation and continued for 24 hours postoperation.
Surgical procedure
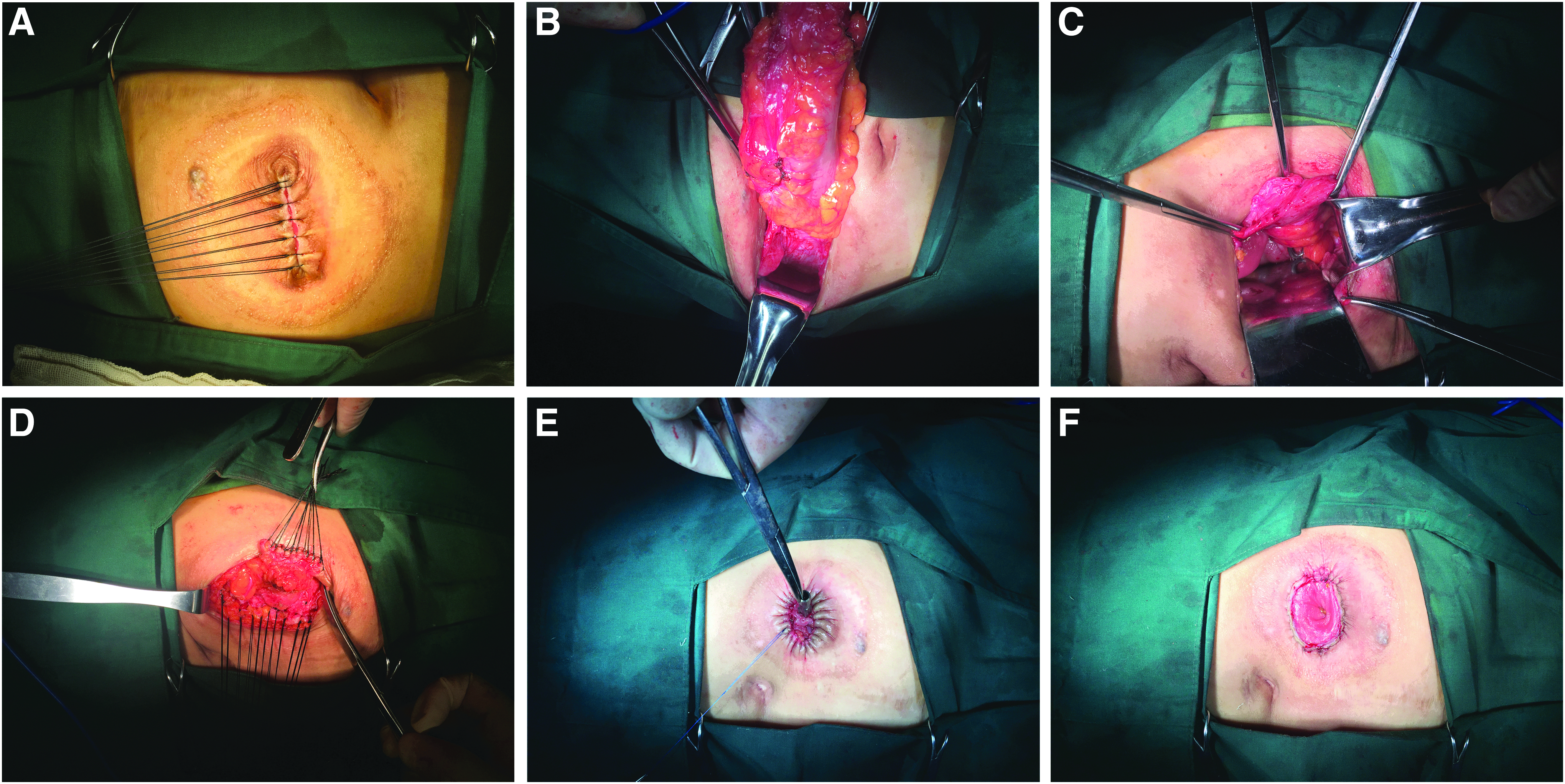
The patient was placed in a horizontal position. After satisfactory general anesthesia had been induced, we sutured the stoma discontinuously so that we could reduce outflow of the intestinal contents (Fig. 1A). Skin and subcutaneous tissues around the stoma were sharply dissected until the hernial sac was clearly exposed. The entire hernial contents were then placed into the abdominal cavity. The sigmoid colon and its mesentery were dissected sequentially until they were entirely dissected (Fig. 1B). The aponeurosis of the obliquus externus abdominis was cut crossly ∼5 cm outside of the hernial sac, and parts of the obliquus externus abdominis, obliquus internus abdominis, and transversus abdominis were cut layer by layer. Next, we created a tunnel, 5–10 cm in length, along the extraperitoneal spaces. At the end of the tunnel, we created a hole at the side of the peritoneum, which was 3–4 cm in diameter. Then, the closed broken end of the sigmoid colon was dragged out of the abdominal wall via the tunnel (Fig. 1C). The defective peritoneum and rectus abdominis anterior sheath were then sutured (Fig. 1D), and the closed broken end was reopened (Fig. 1E) and finally anastomosed with skin using the stapling technique (Fig. 1F).
Follow-Up
The first day after surgery represented the beginning of the follow-up period. Patients were asked to visit the colostomy outpatient department every 3 months after leaving the hospital, and the deadline of follow-up period was February 28, 2017. No patient was lost during follow-up. In March 2017, we completed our assessment of stoma function by either telephone or by letter. The questions and standards used in this assessment were set by international colostomy practitioners within our team, and are shown in Table 1.
Results
We successfully completed the Longtan modification in all 26 cases, including 12 (46.2%) males and 14 (53.8%) females. Mean patient age was 58.2 years (range: 46–68 years), mean body mass index was 23.8 kg/m2 (range: 21.5–27.2 kg/m2), mean interval from accepting radical surgery to PSH formation was 21.6 months (range: 17–27 months), and mean diameter of hernia ring was 7.6 cm (range: 5.2–9.5 cm). Please refer to Table 2 for a complete breakdown of these data.
BMI, body mass index.
Mean operation time was 94.2 minutes (range: 76–118 minutes), and mean intraoperative blood loss was 18.0 mL (range: 10–30 mL). For all 26 cases, the mean length of time until first flatus was 1.6 days (range: 1.2–2.1 days). Mean postoperative hospitalization time was 4.4 days (range: 3–6 days), and mean hospitalization cost was only $3,750 USD (range: $3,300–4,200 USD). No severe complications such as postoperative hemorrhage, ischemic necrosis, peritoneal infection, or intestinal obstruction occurred, except in one case who suffered from postoperative infection of the site of incision; this patient had fully recovered from this infection 3 weeks later following regular dressing changes. None of the patients died after undergoing the Longtan modification. The mean length of the follow-up period was 26.5 months (ranged: 8–48 months) and there was no PSH recurrence in any of the cases during the follow-up period (Table 3). Representative images of preoperative and postoperative stoma are shown in Figure 2.

In addition, stoma function was also assessed and the results are shown in Table 4. Cases tended to experience a stimulatory signal before defecating; in 19 cases, this signal lasted for more than 1 minute. In 24 cases, the frequency of defecation was < 6. The number of cases experiencing good regularity of defecation and self-controlled ability of defecation was 11 and 14, respectively.
Q, question.
Discussion
Despite the advances in surgical devices and improvements in surgical performance, it is still difficult to avoid sigmoidostomy for patients with ultralow rectal cancer. 3 While abdominoperineal resection is considered to be the standard treatment for these cases, PSH still remains the most common long-term complication, can exert an adverse influence on the quality of life, and can increase the psychological burden of the patients involved.4,7
Conservative treatments, such as wearing an elastic bellyband, and treating diseases causing cough or dysuria, are recommended for cases with a small hernial sac and no symptoms of discomfort.11,12 Surgery, however, should be considered for cases with a huge hernial sac, stoma appliance problems, stoma site discomfort, abdominal pain, and intestinal obstruction. It has been reported that reoperative intervention is required in more than 45% of cases with PSH following abdominoperineal resection.13–15
There is no consensus regarding a standard surgical method. Traditional surgical methods mainly include repairing coloboma in situ using mesh and by reconstructive colostomy; these techniques can achieve satisfactory effects to some extent.7,9,10 In addition, some research studies have moved away from a surgical focus and toward prevention. Brandsma et al. 16 conducted a randomized controlled trial (RCT) to investigate the incidence of PSH after end-colostomy formation using a polypropylene mesh, and compared this technique against conventional colostomy formation. Results showed that 3 of 67 patients (4.5%) in the mesh group and 16 of 66 patients (24.2%) in the nonmesh group developed PSH (P = .0011). A meta-analysis, including seven RCTs with low bias risk, was conducted by López-Cano et al. 5 and showed a significant reduction of the incidence of PSH using a mesh (ratio rate [RR]: 0.43; 95% confidence interval [95% CI]: 0.26–0.71; P = .0009). However, the high rate of recurrence, the complicated nature of procedure, the high incidence of incision infection, and foreign body sensation, all represent major deficiencies of traditional surgical methods. DeAsis et al. 10 reported that 81 recurrences, with a recurrence rate of 17.4% (95% CI: 9.5–26.9), following laparoscopic intraperitoneal mesh repair. Warwick et al. 17 further reported that only repair of PSH using a crosslinked porcine dermal collagen biological mesh reinforcement showed poor long-term outcomes with unacceptably high recurrence rates (26/29, 89.6%), and should not, therefore, be performed.
Extraperitoneal sigmoidostomy, as a way to reduce the incidence of PSH, was first put forward by Goligher in 1958. 18 Over the last few decades, several clinical studies have verified the effectiveness of this technique in reducing PSH. For example, Kroese et al. 19 reported that extraperitoneal sigmoidostomy led to significantly lower PSH rates: 22 of 347 (6.3%) for extraperitoneal versus 125 of 701 (17.8%) for transperitoneal (RR: 0.36; 95% CI: 0.21–0.62, P < .001). Zhang et al. 20 reported that no PSH cases were observed during the follow-up period of 42 cases undergoing laparoscopic abdominoperineal resection with circular stapler-assisted extraperitoneal sigmoidostomy. A meta-analysis of stoma-related complications conducted by Wang et al. 21 also showed that an extraperitoneal group had a lower incidence of PSH when compared with a group of patients receiving intraperitoneal sigmoidostomy (1/206 versus 24/163; odds ratio: 0.10; 95% CI: 0.03–0.29; P < .0001).
In our present study, a total of 26 consecutive cases successfully completed the Longtan modification. Our results showed that this procedure is time saving, causes minimal bleeding, and leads to quick recovery and a short period of hospitalization. No severe complications occurred except in one case who suffered from postoperative infection of the incision site. None of our cases suffered a recurrence of PSH during the follow-up period. Thus, we proved the Longtan modification to be both safe and feasible. In addition, stoma function was effective following the Longtan modification. Cases undergoing extraperitoneal sigmoidostomy tended to show a stimulatory signal before defecation, which tended to last for more than 1 minute in most cases, thus meaning that patients had sufficient time to prepare. Experiencing regular defecation and having the self-controlled ability of defecation are likely to be of significant convenience for quality of life. Furthermore, this procedure saves money compared with traditional surgical methods, because an expensive mesh, valued at $750-1,200 USD in China, might not be required. Consequently, the economic burden associated with these patients can be significantly reduced.
Although our small sample size may represent a limitation of this study, all of our cases were independently selected for this innovative procedure and subjects agreed to a long period of follow-up. In future, we hope that the safety and feasibility of this procedure can be further verified in a larger sample size and with a longer follow-up period.
Conclusions
The Longtan modification appears to be an effective and economical surgical innovation for cases with PSH following intraperitoneal sigmoidostomy. This procedure is therefore worthy of further dissemination, although further studies are required for verification.
Ethical Standard
This study was approved by the Ethics Committee of National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100021, China.
Footnotes
Acknowledgment
This work was supported by The Central Level & Public Welfare Basal Research Fund of Chinese Academy of Medical Sciences (Grant No. 2016ZX310020).
Authors' Contributions
Study conception and design: P.W., H.S., Z.Z., H.Z. Acquisition, analysis, and interpretation of data: J.L., Z.W. Drafting of the manuscript: P.W., H.S. Critical revision of the manuscript: P.W., H.S., J.L., Z.W., Z.Z., H.Z. Final approval for submission: P.W., H.S., J.L., Z.W., Z.Z., H.Z. Agreement to be accountable for all aspects of the work: P.W., H.S., J.L., Z.W., Z.Z., H.Z.
Disclosure Statement
No competing financial interests exist.