
Abstract
Abstract
Background:
Postoperative leaks develop in a low percentage of patients undergoing laparoscopic sleeve gastrectomy (LSG), representing a rare yet devastating postoperative complication increasing morbidity and hospital stay. Leaks can become collections and may be very difficult to manage. Several therapeutic options with variable results, including surgical and nonsurgical methods have been described. Endoscopic abscess septotomy is an alternative method recently performed by a few centers reporting efficacy and safety outcomes. The purpose of this report is to present our successful experience with endoscopic abscess septotomy for the treatment of postsleeve gastrectomy leaks.
Methods:
Two female patients with post-LSG leaks and abscess formation diagnosed 4 weeks postprocedure, initially managed with diagnostic laparoscopy, peritoneal washout, and drain placement with poor improvement, were chosen for endoscopic abscess septotomy with concomitant lumen dilation and sleeve axis rectification.
Results:
Endoscopic abscess septotomy was successfully performed in both patients with no complications. Clinical and radiological resolutions were accomplished at 10 and 12 weeks, respectively, postseptotomy.
Conclusion:
This endoscopic approach is a feasible and effective method for the treatment of leaks and collections after LSG. Concomitant balloon dilation of the gastric sleeve improves gastric emptying and reduces intraluminal pressure, hence favoring tissue healing and leak resolution.
Introduction
L
Leaks represent a serious and potentially life-threatening complication of LSG. The management is a multidisciplinary approach aimed at controlling sepsis by defining the leak and managing potential collections either through a nonoperative approach such as a percutaneous or endoscopic drainage or through surgical intervention.
During the abscess septotomy, the septum separating the gastric lumen and the abscess cavity is incised and divided, completely exposing the surfaces of both spaces 6 ; the idea of making the abscess cavity bigger was initially conceived after the concept of myotomy for the treatment of Zenker's diverticulum, where the muscle is incised and a route from the diverticulum to the esophageal lumen is opened, thus suppressing the accumulation of contents in such a cavity. 7 Endoscopy plays a valuable role for this purpose. 8
The objective of this report is to present our experience managing 2 cases of postsleeve gastrectomy leaks with endoscopic abscess septotomy and concomitant lumen dilation and sleeve axis rectification.
Materials and Methods
Case 1
A 42-year-old female underwent a laparoscopic band removal with conversion to sleeve gastrectomy. Four weeks after the procedure, the patient presented with abdominal pain and signs of hemodynamic instability; a gastric leak was diagnosed and managed with diagnostic laparoscopy, peritoneal washout, and drain placement. Six weeks postsleeve gastrectomy, the patient status was unimproved, and evaluation with upper gastrointestinal imaging series and computed tomography (CT) scan of the abdomen demonstrated a distal stenosis of the sleeve, and contrast extravasation and stagnation at the gastroesophageal junction (GEJ) were consistent with an anastomotic leak and abscess formation. The patient was chosen for endoscopic abscess septotomy.
Case 2
A 43-year-old female who underwent LSG with hiatal hernia repair presented signs and symptoms of sepsis 4 weeks after the procedure; a gastric leak was diagnosed and initially managed with diagnostic laparoscopy, peritoneal washout, and drain placement. Subsequent diagnostic studies including an upper gastrointestinal imaging series revealed distal stenosis of the sleeve and a CT scan of the abdomen demonstrated gross extravasation and collection of contrast at the GEJ, subsequently treated with CT-guided percutaneous drainage and endoscopic stent placement. Eight weeks post-LSG, under sepsis control and nutritional optimization, and endoscopic leak management with stents, the patient's condition improved; however, diagnostic studies demonstrated incomplete resolution of the collection. At 11 weeks post-LSG, the patient was chosen for endoscopic abscess septotomy.
Endoscopic abscess septotomy procedure
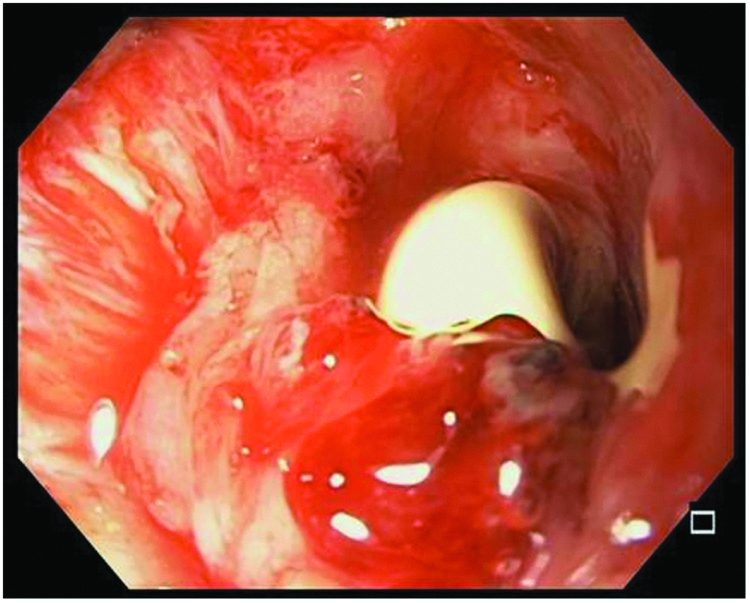
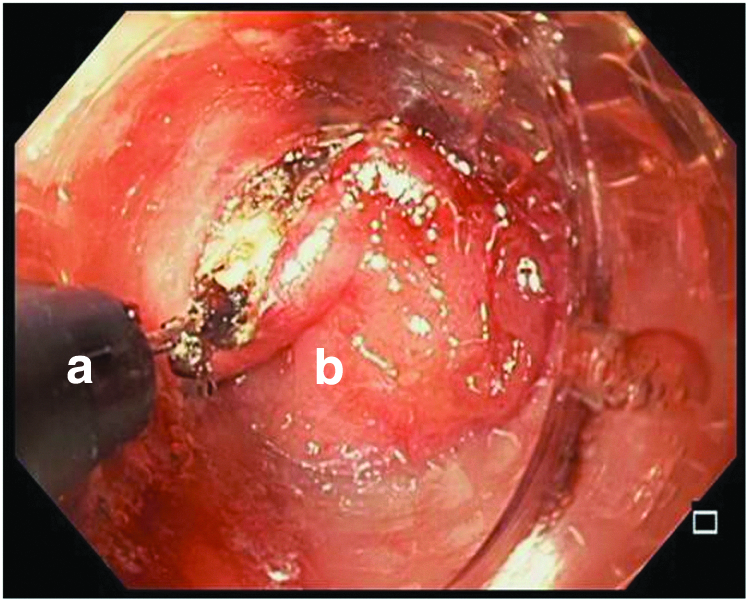
In the operating room, a gastroscope was delivered into the distal esophagus without difficulty. Air insufflation was maintained to examine the mucosal lining of esophagus, stomach, and duodenum. The first step consisted in delineating the anatomy of the sleeve gastrectomy, with special attention to the leak and its relationship with the GEJ. Similarly, a thorough examination of the sleeve was performed with particular attention to angulation, strictures, or spiraling of the sleeve. Both patients had a previous sleeve gastrectomy with fistulas evident right at the angle of His with a septum separating the abscess cavity and the lumen (Fig. 1). Carefully, the abscess cavity was entered and inspected; in both cases we were able to localize the percutaneous drains previously placed (Fig. 2).

Endoscopic view:
Endoscopic view of a percutaneous drain previously placed.
The abscess cavities were irrigated with saline, debris removed, and aspirated as needed, minimizing contamination. Next, using a triangular knife coupled with electrocautery, we proceeded to divide the septum between the abscess cavity and the lumen of the sleeve (Fig. 3). The septum division was completed when the wall of abscess cavity was entirely exposed to the lumen of the sleeve (Fig. 4). Under direct endoscopic visualization, the percutaneous drain was pulled sequentially about an inch but left in the cavity and resecured to the skin with 1-0 Nylon.
Endoscopic view of the triangular knife used for the septum division.
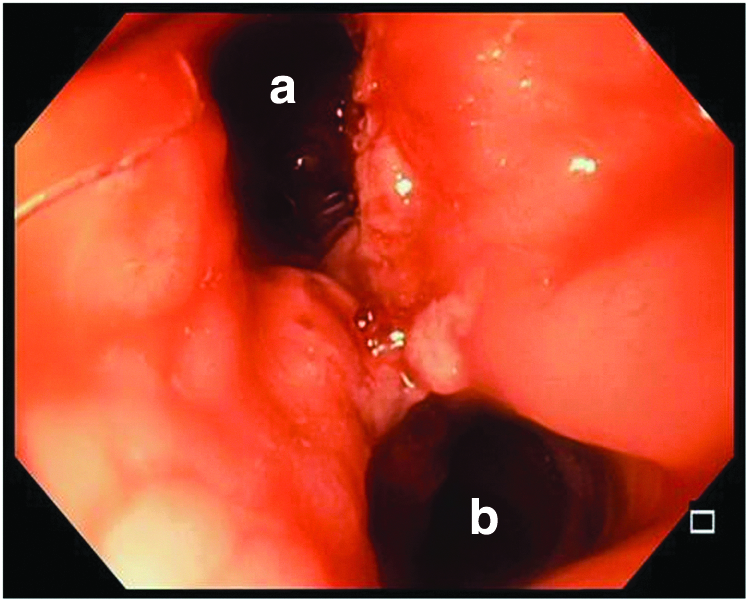
Endoscopic view of the septotomy completed with the abscess cavity fully exposed to the gastric lumen.
Next, dilation of the sleeve was attempted to improve distal drainage. Metal markings were placed on the skin corresponding to the pylorus, incisura, and proximal sleeve. The endoscope was advanced to the duodenum and a guide wire was passed, then the endoscope was retrieved. Using fluoroscopy assistance, we decided to use a 30-mm pneumatic balloon dilator with a length of 8 cm that was passed and parked at the previously marked spots. The sleeve was dilated two times by gradually inflating the balloon with 15 psi. With this dilation the stricture was resolved; using a larger dilator or higher pressure could increase the risk of injury to the sleeve. Finally, the balloon and wire were retrieved, and endoscopy after completion was performed that revealed no iatrogenic injuries or perforation. The endoscope was then carefully removed without complication.
Results
The patients described underwent endoscopic abscess septotomy at our center at weeks 1 and 7 postdiagnosis of the gastric leak, respectively. The procedure was performed successfully with no complications. On postoperative day 1, an upper gastrointestinal imaging series was performed that confirmed no further leakage. Two endoscopic re-evaluations were performed on each patient at weeks 3 and 5 postseptotomy that showed progressive healing of the injured tissue allowing the percutaneous drains removal. Both patients achieved clinical and radiological resolution of the leak at weeks 10 and 12 postprocedure, respectively.
Discussion
Postoperative leaks after LSG represent a very serious complication of bariatric surgery. The International Sleeve Gastrectomy Expert Panel Consensus Statement classified leaks based on the time of presentation as acute (within 7 days), early (within 1–6 weeks), late (occurring after 6 weeks), and chronic leaks (after 12 weeks). 9 A multifactorial causality has been described, winding up to two major pathogenic mechanisms: mechanical leaks, mostly related to the long staple-line intrinsic of LSG, which appear early in the postoperative period, and ischemic leaks, occurring later in the postoperative period, usually at the GEJ, and are caused by the reduced vascularization of the angle of His compared with other gastric regions. 10 Furthermore, patients with concomitant distal stenosis of the sleeve, where the impaired gastric emptying is raising the intraluminal pressure that surpasses the staple-line resistance, are prone to developing disruption of the tissue and leakage. 11
Diagnosis is based on the patient's postoperative symptoms and signs plus image studies such as upper gastrointestinal imaging series, usually on postoperative days 1–3, or a CT scan with oral and intravenous contrast, which allows the identification of the postoperative anatomy and the presence of complications (contrast extravasation, free intra-abdominal gas or liquid, and collections) 11 ; intraoperative tests using methylene blue or the “air-leak” test are somehow useful when positive, but they do not predict the potential development of leaks in the future. 9
The keystone management of post-LSG leaks and collections is aimed at reducing the leak, resolving the fistula, and draining the abscess cavity. Unfortunately, no clear or standardized protocol has been established for this purpose. Several studies report the variable efficacy of endoscopic stent placement for the healing of fistulas and leaks,12–15 positioning this technique as the most popular treatment 16 ; however, complications associated with it, such as migration of the stent in about 58%–62% of the times, 14 mucosal tears, and bleeding have also been reported. 17
Management algorithms depending on the size of the fistula, 17 time of presentation of the leak, distal stomach stricture association, the patient's nutritional status, and the presence of peritonitis 18 have been developed by a few centers to assist this yet nonstandardized treatment.
In addition, for the management of early leaks, some authors have reported the successful use of the Over-the-Scope Clip system.4,19,20 For chronic leaks, different methods including continuous pneumatic dilation with endoscopic septotomy, 21 or a definitive reconstruction with surgical conversion of the gastric sleeve to a Roux-en-Y gastric bypass or a total gastrectomy11,17 has also been reported.
It has been already established and confirmed the importance of endoscopy in the management of postoperative bariatric surgery complications. 22 Furthermore, we would like to point out the role of endoscopic septotomy as a feasible approach, providing good outcomes in terms of leak resolution.23–25 Lima 24 shared his experience by applying this technique to 10 cases of early post-LSG leaks, achieving leak resolution, reduction in the duration of hospital stay, and reduced need for reintervention. Likewise, Mahadev et al. 25 performed this procedure for the treatment of late and chronic leaks in conjunction with balloon dilation to address sleeve strictures (if present), reporting a 100% resolution by clinical and radiographic confirmation. Campos et al. 26 detailed the technical aspects of the procedure, which is similar to the operation performed at our center.
In addition, we would like to point out the parameters for an adequate septotomy and immediate postprocedure management. First, the septum must be incised from the fistulous orifice all the way down to the base of the abscess cavity. The incision is completed when the base of the abscess cavity is fully visualized through the sleeve lumen. A triangular knife works better than a needle knife when an extreme fibrotic septum is encountered. Next, saline irrigation of the abscess cavity with removal of debris, nonvital tissue, and residual staples must be sequentially performed to improve visualization of the cavity. Finally, resolving the sleeve stenosis with balloon dilation provides a better evacuation route of gastric contents (leaked contents and debris). The dilation also improves the healing process by reducing intraluminal pressure.
Regarding the postprocedural management, an upper gastrointestinal imaging series is necessary on postoperative day 1 to confirm no further expansion of the leak. Enteral feeding should be progressively introduced if imaging is negative. Endoscopic follow-up on weeks 3 and 5 postprocedure is recommended to evaluating the healing process and drain removal.
Regarding the cases we presented, the endoscopic abscess septotomy successfully allowed the internal drainage of the collection with redirection of the secretions back to the stomach sleeve, promoting healing and resolution of the fistula. Moreover, we theorize that the concomitant use of the balloon dilator during this endoscopic procedure relieves the distal stenosis of the sleeve and reduces the intraluminal pressure, therefore, providing a better gastric environment for the closure of the leak.
Conclusion
Endoscopic abscess septotomy represents a safe and less invasive alternative for the treatment of postoperative leaks. This novel treatment favors the internal drainage of the collection, redirecting the leak flow toward the gastric lumen providing tissue healing and decreasing the expansion of the collection, hence reducing the need for additional surgical intervention. This is a feasible and effective method to treat these severe post-LSG complications, and further multicenter, prospective studies are necessary to achieve standardization of this technique.
Ethical Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the report.
Footnotes
Disclosure Statement
C.B.O. and A.D.G. have no competing financial interests. D.P. is a consultant for Medtronic/Covidien, Teleflex, Gore, Allergan, and Intuitive; in addition, he holds a grant from Teleflex.