
Abstract
Abstract
Background:
The aim of this study was to evaluate demographic and clinical characteristics of the children undergoing laparoscopic varicocelectomy by using polymeric ligating clips and to evaluate postoperative outcomes and analyze semen according to the grade of varicocele after surgery.
Patients and Methods:
The case records of 120 pediatric patients who underwent laparoscopic varicocelectomy were retrospectively reviewed. The following parameters were examined: age, grade of varicocele, lateralization, diameter of spermatic veins, indications for surgery, duration and outcomes of surgery, complications, and recurrence rate. For patients older than 16 years of age, semen analyses were obtained before and after the surgery and were compared according to the clinical grade of varicocele.
Results:
The median age of the patients was 15 years. Of the total number of patients, left-sided varicocele was found in 119 patients and bilateral varicocele was found in 1 patient. Of the 120 varicoceles, 8 (6.7%) were grade I, 58 (48.3%) were grade II, and 54 (45%) were grade III. There were no major intraoperative complications. Hydrocele was found in 2 (1.6%) patients. There were no cases of recurrence recorded. Sperm concentration (P < .01), morphology (P < .01), and motility (P < .01; P = .02) improved 6 months after surgery in patients with varicocele grades of I and II, respectively. In grade III varicocele, only sperm concentration (P < .01) and morphology (P = .03) improved whereas motility (P = .150) did not change significantly.
Conclusion:
Laparoscopic varicocelectomy using polymeric ligating clips is a safe, feasible, and cost-effective technique, with a low rate of postoperative complications and recurrence and it significantly improves sperm parameters in adolescents.
Introduction
V
The aim of this study was to evaluate the demographic and clinical characteristics of the children undergoing laparoscopic varicocelectomy by using polymer ligating clips and to evaluate postoperative outcomes and effects on testicular volume improvement and semen parameters during a 5-year period.
Material and Methods
Patients
The case records of 120 children, treated laparoscopically for symptomatic varicocele from May 2012 to May 2017 at the Department of Pediatric Surgery, University Hospital of Split, Croatia, were retrospectively reviewed. Informed consent was obtained from the parents of all the patients, and the Ethics Committee of the University Hospital of Split approved the study. All patients with symptomatic varicocele younger than 18 years of age who were operated laparoscopically by using 5-mm polymer ligating clips were enrolled in the study. The exclusion criteria were patients older than 18 years of age, the patients operated with open approach, patients with recurrent varicocele who were previously operated by open approach, and patients with incomplete data or follow-up shorter than 3 months. The patient data are summarized in Table 1.
BMI, body mass index.
Preoperative evaluation
Varicocele was defined on ultrasound as dilation of the vessels of the pampiniform plexus greater than 2 mm. In physical examination, varicocele was graded according to Dubin and Ambler's classification. 10 In all of the patients, physical examination, levels of serum luteinizing hormone (LH)/follicle-stimulating hormone (FSH), ultrasound of the testicles, and urinary tract were performed and for the patients older than 16 years of age semen analysis was carried out before treatment. Indications for surgical intervention included the following: testicular volume discrepancy >20%, abnormal semen parameters, persistent pain or testicular discomfort due to varicocele, and elevated serum levels of LH/FSH.
Hypothesis and outcome measures
The primary endpoint of this study was to test the hypothesis that using polymer ligating clips is an efficient method of treatment for varicocele with great results and a low rate of recurrence and complications. The primary outcome measures were the treatment outcome, the frequency of intraoperative or postoperative complications, the rate of recurrence, and the sperm quality and count analysis in 6 months and 1 year postoperatively. The secondary outcome variables were indications for surgical treatment, duration of surgery, hospital stay, and the rate of reoperations. The intraoperative complications included access-related complications, such as organ lesions, thermal damage of intra-abdominal organs, and intraperitoneal bleeding. Postoperative complications included bleeding into the abdominal wall, wound infection, postoperative ileus, pain, and formation of hydrocele.
Operative technique
General anesthesia with laryngeal mask was used in all patients. A Veress needle was introduced below the umbilicus and CO2 insufflated at a pressure of 8–12 mmHg depending on the patient's age and body weight. The first trocar was introduced through the same incision. After exploration of the abdominal cavity, two additional 5 mm trocars were introduced in the right and left midclavicular line, 1–2 cm below the horizontal line to the umbilicus, along the lateral border of each abdominal rectus muscle (Fig. 1). After identification of spermatic vessels and identification of vas deferens (Fig. 2A), the peritoneum was opened by using laparoscopic scissors in the lateral aspect from a point 1 cm superior to the internal inguinal ring along the testicular vessels to expose them (Fig. 2B). After mobilization of spermatic vessels, accompanying lymphatics were preserved from the spermatic veins (Fig. 2C). Non-absorbable polymeric ligating clips (Ligating Clips ML; Grena, Brentford, United Kingdom) were used for ligation of spermatic vessels (Fig. 2D). Spermatic vessels were resected by using laparoscopic scissors (Fig. 2E). When the procedure was completed, the intraperitoneal pressure was reduced to 5 mmHg to check the surgical site and to ensure absence of bleeding (Fig. 2F). The trocars were subsequently removed. Skin incisions were closed by simple skin sutures.

Trocar position. The first 5 mm trocar was placed supraumbilically. Two 5 mm trocars were introduced in the right and left midclavicular line, 1–2 cm below the horizontal line to the umbilicus, along the lateral border of each abdominal rectus muscle.
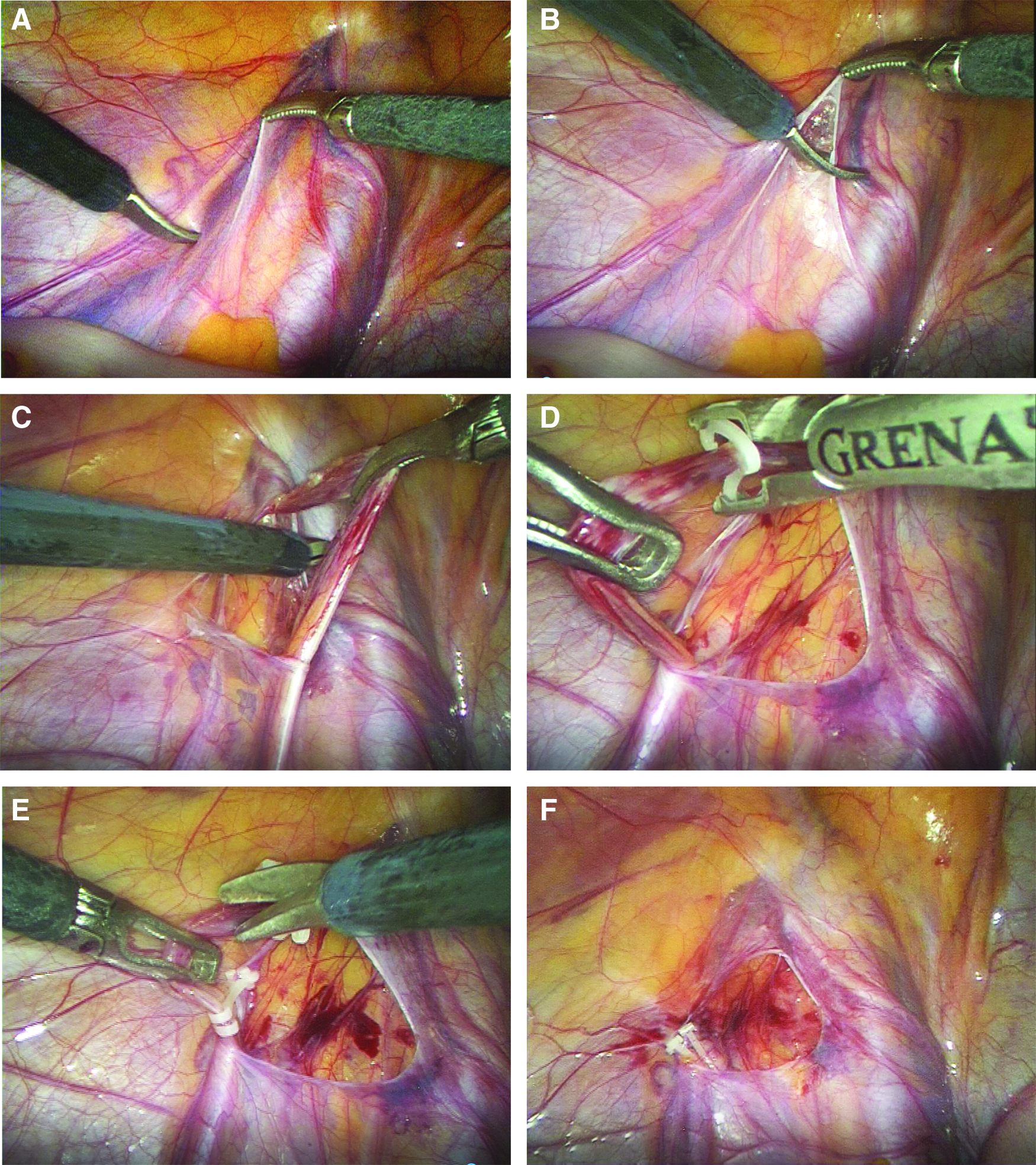
Laparoscopic varicocelectomy:
Follow-up
All patients were discharged from hospital the day after surgery. The patients were followed up at our outpatient clinics at the first and fourth week after surgery for detection of any complications. Skin sutures were removed during the first week visit. Follow-up program consisted of physical examination and ultrasound 6 months after surgery to assess testicular size, the presence of late complications, and persistence or recurrence of the varicocele. Semen analysis was performed 6 months and 1 year after surgery for patients older than 16 years of age.
Statistical analysis
The data were analyzed by using the Microsoft Excel for Windows Version 11.0 (Microsoft Corporation) and SPSS 19.0 (IBM Corp, Armonk, NY) software programs. Distributions of quantitative data were described by means and standard deviations, or medians and ranges, whereas absolute rates and percentages were used to describe categorical data. The difference between pre- and post-operative seminal data was analyzed by using a paired Wilcoxon signed-rank test. All values of P < .05 were considered to indicate statistical significance.
Results
During the study period, a total of 120 patients with a median age of 15 years (range 13–18 years) underwent laparoscopic varicocelectomy. Median follow-up was 25 (range 3–61) months. Of the total number of patients, left-sided varicocele was found in 119 patients (99%) and bilateral varicocele was found in 1 patient (1%). Varicocele grades I, II, and III were detected in 8 (6.7%), 58 (48.3%), and 54 (45%) patients, respectively. Median diameters of veins in varicocele grades I, II, and III were 2.95, 3.20, and 4.0 mm, respectively. Hospital stay was 1 day for all of the patients. The medians of operation duration were 12 minutes (10–35 minutes) and 19 minutes for unilateral and bilateral cases, respectively. The patient data are summarized in Table 1. The indications for operative intervention were diverse. The most frequent recorded indication for treatment was testicular volume discrepancy >20%, followed by abnormal semen parameters and pain/testicular discomfort. All indications for surgery are presented in Table 2.
Out of a total of 120 patients, 94 had one indication, whereas 26 had two or more indications of surgery.
FSH, follicle-stimulating hormone; LH, luteinizing hormone.
There were no major intraoperative complications. Only 1 case of intraoperative injury of the spermatic vein was recorded. This was easily controlled, and no conversion or blood transfusion was required. A total number of 3 (2.5%) postoperative complications was recorded. In 1 patient (0.8%), hematoma in supraumbilical incision due to injury of epigastric blood vessel was found. Hydrocele was found in 2 (1.6%) patients, 6 months after surgery. Hematoma was treated with hemostatic suture and in both patients with hydrocele, Winckelmann's procedure was performed. There were no cases of recurrence recorded. Treatment outcomes are presented in Table 3.
Sperm concentration (P < .01), morphology (P < .01), and motility (P < .01; P = .02) improved 6 months after surgery in patients with varicocele grades of I and II, respectively. However, in grade III varicocele, only sperm concentration (P < .01) and morphology (P = .03) improved whereas motility (P = .150) did not change significantly (Table 4).
Wilcoxon signed-rank test.
IQR, interquartile range.
Discussion
There are many controversies about the treatment of varicocele in the pediatric population, because not all varicoceles cause infertility. Regarding this, it is important to define the true indications for varicocelectomy, to select only the patients who really need surgery.
Although it is not appropriate to ask for semen analysis in adolescents, there is consensus that semen analysis may be performed in adolescents older than the age of 16. 11 In addition, improved semen quality has been demonstrated after adolescent varicocele repair in many studies.11–13
Generally, in the pediatric population, varicocelectomy is indicated in the case of abnormal findings in spermiogram, when the testicular volume is decreased >20%, in case of elevated levels of serum LH/FSH and when associated with persistent pain/discomfort.7,8,11 In our study, in most of the patients, surgery was performed due to testicular volume decrease, followed by abnormal findings in spermiogram and persistent pain or discomfort.
There are several surgical procedures for a surgical varicocele repair: retroperitoneal (Palomo), inguinal (Ivanissevich), and subinguinal approaches. Of these, a retroperitoneal procedure can also be performed laparoscopically, and inguinal and subinguinal approaches are usually performed by using a surgical microscope or lupes.11,14–17 In adult infertile men with varicocele, microsurgical inguinal or subinguinal varicocelectomy is reported to have the highest success rate with lowest morbidity, although the duration of surgery may be longer than that with conventional approaches. In adolescents, a recent survey of pediatric urologists found that the most common surgical approach to adolescent varicocelectomy was the laparoscopic approach.15,16 Laparoscopic varicocelectomy is equally effective as open varicocelectomy. 17 Currently, laparoscopic varicocelectomy gained traction, as pediatric urologists have become increasingly facile with laparoscopic techniques. Wang et al. performed retrospective analyses of 1326 laparoscopic varicocelectomy cases performed by 16 participants, and they demonstrated that the learning curve for laparoscopic varicocelectomy was 15 cases. 14 Laparoscopy has been shown to have the same intraoperative safety, shorter hospital stay, and less postoperative complications.11,17,18
Intraoperative complications in laparoscopic varicocelectomy are rare.3,4,17,19 These are usually general complications of the laparoscopic approach. Serious intraoperative complications were not observed in our study. Only in 1 patient, bleeding due to injury of the spermatic vein was recorded, but it was easily controlled without further complications. The most postoperative complications are hydrocele formation and recurrence. Testicular atrophy is rarely found.4,17–19 In this study, no case of testicular atrophy was recorded.
The laparoscopic approach provides better magnification, which is more helpful to preserve the testicular artery and lymphatic vessels. There are two main approaches for laparoscopic varicocelectomy. One is mass ligation of spermatic vessels, and the other is just ligation of the veins and sparing lymphatics and testicular artery. Hydrocele formation is related to failure to preserve the lymphatic vessels associated with the spermatic cord. The risk of hydrocele formation after mass ligation of spermatic vessels ranges from 3% to 25%.3,19,20 As for a laparoscopic approach, it seems that lymph sparing may not increase the recurrence rate, although it would decrease the postoperative hydrocele rate. 3
Misseri observed very good outcomes after lymphatic sparing varicocelectomy. 21 They reported a significantly higher rate of hydrocele formation after mass ligation. Kocvara reported 17.9% hydrocele formations with conventional laparoscopic varicocelectomy and 1.9% after lymphatic vessel preservation. 22 In our study, mass ligation was performed. Only 2 cases (1.6%) of hydrocele formation during a median of 25 months follow-up after surgery were encountered. It is similar with the results of Tarun et al., who reported hydrocele formation in 2 patients (4.88%) when mass ligation was done. 23
Recollateralization or failure to ligate all branches of internal spermatic veins may be a cause of varicocele recurrence. The risk of recurrence after laparoscopic varicocelectomy ranges from 0% to 11%. 1 McManus et al. reported 0% of recurrence rate at their center while doing laparoscopic mass ligation, whereas Keys et al. had a recurrence rate of 8.3%.24,25 Some studies showed that recurrence rates and complication rate of laparoscopic varicocelectomy are similar to those reported with open surgery.1,26 On the other hand, there are many reports of lower rate of recurrence with the laparoscopic approach.27,28 Recurrence increases progressively with the increase of varicocele grade.3,27 Ligation of the artery does not impair testicular growth, and, thus, it is more useful and safer to interrupt the artery to avoid recurrence due to periarterial venous network. Many studies demonstrated that laparoscopic varicocelectomy with internal spermatic artery ligation has lower recurrence rate than without internal spermatic artery ligation.23,29,30 In the study of Tarun et al., there were no recurrences when mass ligation was performed. Recurrence was found only in patients when artery-preserving ligation was done. 23 Our findings are similar to previous reports. We performed mass ligation in our study and found no recurrences.
Laparoscopic varicocelectomy is a simple and quick procedure. An average duration of varicocelectomy in literature is about 15–25 minutes.3,27 Operative times of open or laparoscopic varicocelectomy can be reduced to ∼15 minutes in the hands of experienced surgeons. 27 The means of operation duration in the study of Karami et al. were 25.7 and 37.1 minutes for unilateral and bilateral cases, respectively. Barry et al. reported an operative time for laparoscopic varicocelectomy of 14.7 minutes in unilateral cases and 21.6 minutes in bilateral cases. 27 In our study, the median of operative time was 12 minutes for unilateral cases and 19 minutes for bilateral cases.
Many studies demonstrated that laparoscopic varicocelectomy can be performed as an outpatient procedure.7,8,24 In this study, all of the patients left our department 24 hours after laparoscopic varicocelectomy.
There are many different approaches reported for ligation of spermatic veins (clips, intracorporeal suture, monopolar/bipolar diathermy, harmonic scalpel). In our series, polymer ligating clips were used to ligate spermatic veins. Polymer ligating clips are made of an advanced polymer to ensure a high level of biocompatibility together with structural and dimensional stability over time, which is necessary for long-lasting patient safety. It can ligate up to 10 mm tissue through a 5 mm trocar or up to 16 mm tissue through a 10 mm trocar in laparoscopic procedures. 31
Some authors reported the usage of harmonic scalpel or LigaSure for sealing of the spermatic vessels. 3 Still, the cost of instruments and unnecessary thermal energy spread with possible lateral thermal damage to surrounding tissues are main disadvantages.32–34
Chen et al. reported excellent results in 47 varicocelectomies using harmonic scalpel (Ultracision). They found only one hydrocele (2.1%), and no other complications have been reported. 35 Patients from a study of Karami et al. treated with bipolar coagulation had significantly higher hydrocele formation (4.3%) and recurrence rates (2.4%), probably due to thermal damage of lymphatic vessels, than the patients from our study treated with polymer ligating clips. 3 Méndez-Gallart et al. used LigaSure for spermatic vessels sealing and reported a high rate of hydrocele formation (14.3%) among their patients. 26 The highest rate of recurrences (10.5%) and hydrocele formations (23.6%) was reported by Polok et al., who used monopolar coagulation for spermatic vessels dissection. They also reported a significantly lower amount of complications when titanium clips were used. 36
Akin et al. evaluated the effects of different intracorporeal ligation techniques with titanium clips, plasma trisector, and surgical silk on laparoscopic varicocelectomy. They found a longer operation time in the group of patients operated with surgical silk. Hydrocele formation (2.8%) and recurrence rate (2.9%) in their study were similar between compared groups. 37 Barry et al. used polydoxanone clips (PDS) in their study and reported rates of 5% of recurrence and 5% of hydrocele formation. 27 In our study, polymer ligating clips were found to be safe, time saving, cost effective, and very easy to use, with lowest recurrence (0%) or hydrocele formation (1.6%) rates. Results of treatment from literature, among different laparoscopic varicocelectomy techniques, are summarized in Table 5.
/, no available data.
PDS, polydoxanone clips.
Most studies reported improved semen parameters after varicocelectomy. A meta-analysis showed improvement in postoperative semen parameters in 71% of the patients who underwent varicocelectomy.3,11 In our study, overall improvement in postoperative semen parameters was found in 81% of the patients. Semen analysis 6 months after surgery showed a significant improvement in sperm concentration, motility, and morphology in varicocele grades I and II. For varicocele grade III, concentration and morphology improved but sperm motility did not show significant changes. Similar findings were reported in the study of Karami et al., with a difference in grade III; they found improvement only in sperm concentration after follow-up of 1 year. 3
Al-Kandari reported no significant improvement in sperm morphology. 15 Our study was performed in adolescents, so this may be the reason of better results in sperm morphology.
Significant improvement of difference in testicular volume was found in 76% of the patients, and 92% of the patients who reported pain or discomfort before the surgery were pain free at 1-year follow-up.
Conclusion
Laparoscopic varicocelectomy using polymeric ligating clips is a safe, feasible, and cost-effective technique, with a low rate of postoperative complications and recurrence. The use of polymeric clips has an advantage of short operative time and low costs, and it significantly improves sperm parameters in adolescents. Laparoscopic varicocelectomy should preferably be done with en-bloc mass ligation, that is, both artery and vein should be ligated.
Footnotes
Disclosure Statement
No competing financial interests exist.