
Abstract
Abstract
Background:
Video-Assisted Thoracic Surgery (VATS) is conventionally performed through multiple small incisions (C-VATS). Recent studies have reported encouraging results with the single-incision VATS (S-VATS) over the conventional technique. However, these studies were either small in size, unfocused, nonuniform, retrospective, lacking follow-up information, or focused on pain. We aim to validate previously reported results in a single large meta-analysis, including only the best evidence studies available.
Methods:
Systematic review of the PubMed archive was conducted to include only full English articles with Newcastle Ottawa Scale score ≥7. The primary outcome was the complications rate while secondary outcomes were operative time, resected lymph nodes (LNs), chest tube duration, estimated blood loss, length of postoperative stay (LOS), and postoperative pain on day 1 after surgery. Odds ratio and standard mean difference were used as effect estimates. Random model and leave-one-out analysis were used.
Results:
A total of 39 studies were included with 4635 patients (1686 S-VATS versus 2949 C-VATS). S-VATS has resulted in significantly less postoperative pain (P < .001), blood loss (P = .006), LOS (P < .001), and chest tube duration (P < .001). In lung cancer patients, the number of retrieved LNs was similar to that of C-VATS (P > .05). Subgroup comparison of the rate of complications between lung resections versus other intrathoracic procedures, lung cancer versus pneumothorax, and lung cancer versus other lung-only lesions did not show any significant differences between the groups.
Conclusion:
Performing S-VATS technique has shown superior postoperative outcomes over the C-VATS technique in the treatment of thoracic disorders. Substantial benefit was confirmed in terms of less postoperative pain, blood loss, drainage time, and postoperative hospital stay.
Introduction
V
Many individual studies have shown various benefits to utilizing this technique over the conventional multiportal technique. Most of these studies were small in size, unfocused, not uniform, retrospective, or missing important follow-up information. Earlier meta-analyses published about this topic were focused on minor thoracic surgeries or postoperative pain. Some included abstracts and scientific posters, articles published in other languages, or included small number of studies. 8
In this study, we aim to conduct a meta-analysis of published literature about single-incision VATS (S-VATS) to compare it with conventional multiportal VATS (C-VATS) and to validate previously reported results in a single large meta-analysis.
Materials and Methods
This systemic review and meta-analysis with its results follow the preferred reporting items for systemic reviews and meta-analysis (PRISMA) statement. 9
Data sources and literature search strategy
A literature review was conducted using PubMed by 2 independent investigators (A.A.A. and M.R.) through PubMed online data sources (up to March 2017), using the search terms “single” or “one” or “uni-portal” and “utility incision-thoracic surgery” or “VATS” or “video-assisted thoracic surgery” or “minimally invasive thoracic surgery.” In addition, upon identifying any related prior meta-analyses or systematic reviews, references were scanned for relevant articles and pertinent reviews (i.e., backward snowballing) to obtain further studies.
Study selection
Inclusion criteria for the clinical outcome studies were as follows: (1) unmatched or propensity score matched (PSM) studies; (2) comparing S-VATS with C-VATS in patients who had any thoracic surgery (i.e., lobectomy, bullectomy, segmentectomy, wedge resection, diaphragm plication, sympathectomy, thymectomy, and pectus excavatum surgery [Nuss procedure]) and included outcomes such as complication rate, operative time, resected lymph nodes (LNs), chest tube duration, estimated blood loss (EBL), length of postoperative stay (LOS), and postoperative pain in day 1 (POD 1); (3) published full text article; and (4) written in English.
Two investigators (A.A.A. and M.R.) independently reviewed the search results at the title and abstract level to determine whether the study met our inclusion criteria. Pertinent articles were then retrieved.
Outcomes
Primary outcome was the reported complications rate, whereas secondary outcomes were operative time, resected LN, chest tube duration, EBL, LOS, POD 1, and 30 days/in-hospital mortality.
Data extraction and statistical analysis
Microsoft Office Excel 2010 (Microsoft, Redmond, WA) was used for data extraction. Data extraction of all included studies was performed independently by 2 investigators (A.A.A. and M.R.). In case of disagreement, a third coauthor's opinion (M.K.) was sought and it was solved by combined agreement. Extracted variables for PSM studies were taken from among the unmatched population. Separate analysis for the matched studies was conducted. Variables included the following: study name and location, publication year, number of patients, study period and design, Newcastle Ottawa Scale (NOS), surgical procedure, age, gender, comorbidities, pathological presentation, operative details, and postoperative course. All types of reported complications were included under complication rates variable.
Review Manager Version 5.3 (The Cochrane Collaboration, the Nordic Cochrane Centre, Copenhagen, Denmark) was used to perform this pairwise meta-analysis. The data can be synthesized only when number of studies was ≥2. Measurement data reported as mean ± standard deviation were adopted; odds ratios (ORs) with standard error for the included studies were calculated and aggregated on the log scale. Individual and pooled ORs with 95% confidence intervals (CIs) were calculated by means of the DerSimonian–Laird (inverse variance) method. 10 Risk difference (RD) was used in case of absence of events in many studies in both arms. Hypothesis testing for statistical homogeneity was set at the two-tailed 0.10 level and was based on the Cochran Q test, with I2 values of 25%, 50%, and 75% representing mild, moderate, and severe heterogeneity, respectively, with random-effect model being used if I2 > 25%, otherwise fixed effect model was adopted. Publication bias was graphically assessed using the funnel plots. The subgroup analysis was performed based on type of procedure and pathology. Leave-one-out analysis was performed by Comprehensive Meta-Analysis software, version 2 (Biostat, Englewood, NJ). The quality of the included studies was assessed by the NOS. 11 Only high-quality studies, defined as those achieving seven or more stars, were included in this review.
Results
Eligible studies and characteristics of studies
For clinical outcomes, 698 studies were identified. After removal of duplicates, 420 studies were screened. Sixty-one full-text articles were assessed for eligibility. Among them 39 studies12–50 (31 unmatched and 8 PSM studies) (see Table 1) met the inclusion criteria. An outline of the PRISMA flowchart for clinical outcomes is shown in Figure 1.
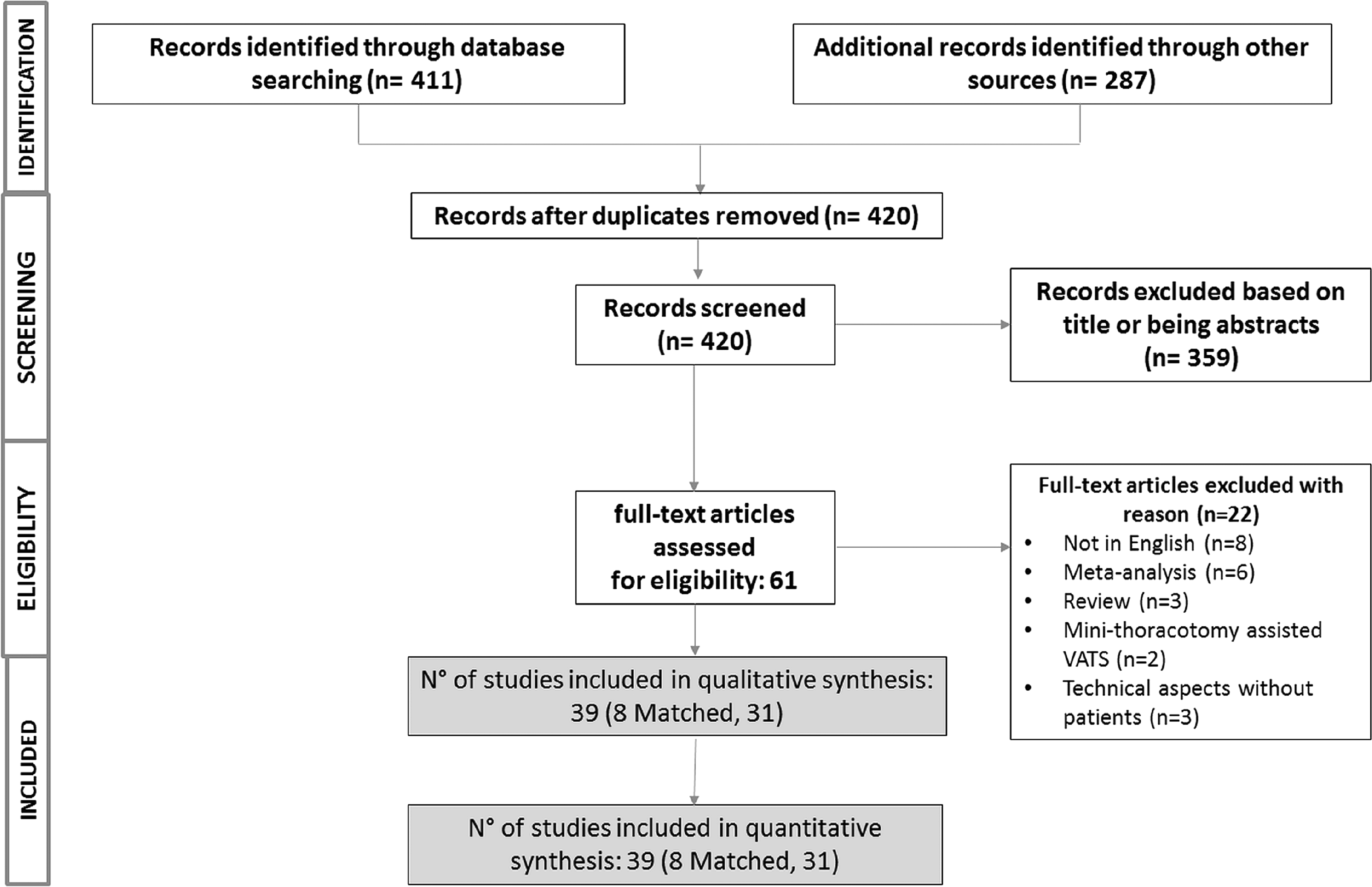
PRISMA flowchart for clinical outcomes. PRISMA, preferred reporting items for systemic reviews and meta-analysis.
NOS, Newcastle Ottawa scale; NR, not reported; PSM, propensity score matched.
Tables 1 and 2 show the characteristics and the overall quality (NOS score) of the included studies. Overall, 21 studies with an NOS score of 9/9, 13 studies with a score of 8/9, and only 5 studies with a score of 7/9 were included in this meta-analysis. Of the 4635 patients included, 1686 (36.38%) underwent S-VATS and 2949 (63.62%) underwent C-VATS.
C-VATS, conventional multiportal video-assisted thoracic surgery; HH, hyperhidrosis; LNs, lymph nodes; NR, not reported; NSCLC, nonsmall cell lung cancer; S-VATS, single-incision video-assisted thoracic surgery.
Table 3 shows the mean and standard deviation values for the continuous outcomes (operative time, resected LN, chest tube duration, EBL, LOS, and postoperative pain).
C-VATS, conventional multiportal video-assisted thoracic surgery; LN, lymph node; LOS, length of postoperative stay; POD 1, postoperative pain in day 1; S-VATS, single-incision video-assisted thoracic surgery; VAS, visual analogue scale.
Meta-analysis of postoperative outcomes
Primary outcome
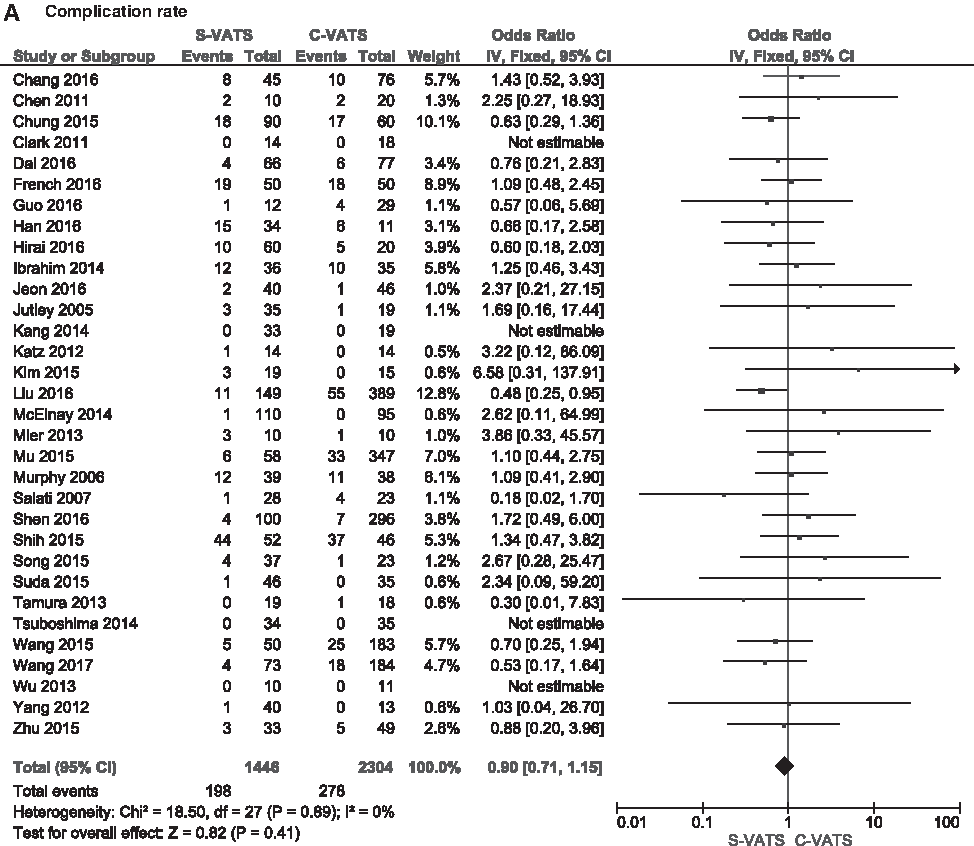
Overall rate of complications after S-VATS (reported in 32 studies) was not significantly different from that of C-VATS (OR = 0.90, 95% CI = 0.71, 1.15; P = .41) (Fig. 2A, Table 4).
Forest plot of comparison of S-VATS versus C-VATS:
C-VATS, conventional multiportal video-assisted thoracic surgery; LN, lymph node; LOS, length of postoperative stay; ND, no differences; OR, odds ratio; POD 1, postoperative pain in day 1; SMD, standard mean difference; S-VATS, single-incision video-assisted thoracic surgery; VAS, visual analogue scale (0–10).
After inclusion of only lung studies, the overall cohort OR was 0.86 (CI = 0.66–1.12, P = .25), subgroup analysis on lung cancer versus other lung lesion revealed no difference in complications rate in each subgroup. In lung cancer subgroup, the OR was 0.80 (CI = 0.59–1.08, P = .15). In other lung lesions (benign/mixed) subgroup, the OR was 1.06 (CI = 0.62–1.79, P = .84). Another subgroup comparison revealed no difference in complications rate in lobectomies (OR = 0.73, CI = 0.47–1.16, P = .18) or in other/mixed lung resection subgroups (OR = 0.93, CI = 0.66–1.28, P = .25) (Supplementary Fig. S1; Supplementary Data are available online at www.liebertpub.com/lap).
Among PSM studies, no difference in the complications rate was found (Supplementary Fig. S2).
Secondary outcomes
(1) Operative time: Operative time reported in 31 studies was not significantly different between both groups (OR = 0.12, CI = 0.07, 0.32; P = .21) (Fig. 2B, Table 4).
(2) Number of resected LNs: No significant difference was found between both groups in 13 studies that reported this outcome (OR = −0.01, CI = −0.19, 0.16; P = .88) (Fig. 2C).
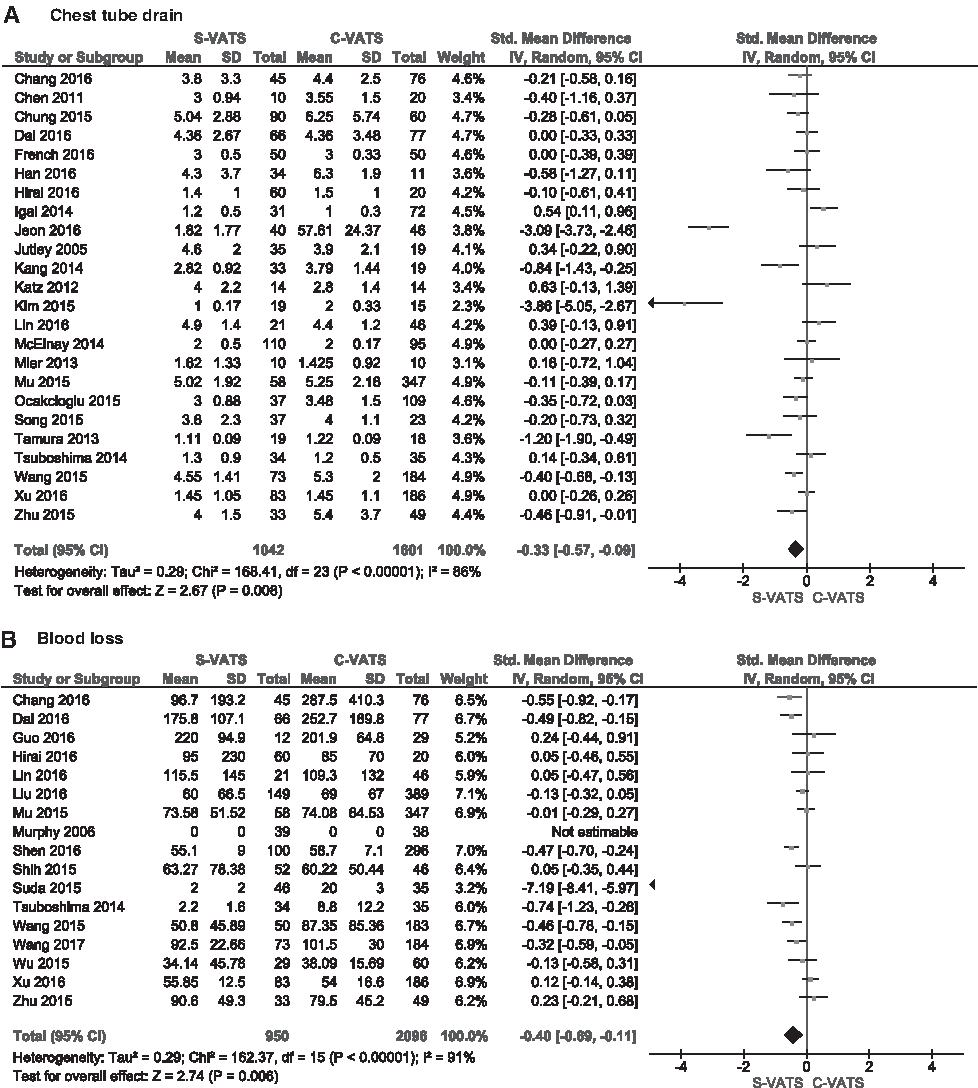
(3) Chest tube duration: This outcome was significantly shorter in the S-VATS group in 24 studies (OR = −0.33, CI = −0.57, −0.09; P = .008) (Fig. 3A).
(4) Blood loss: In 17 studies, the volume of lost blood during the operation was significantly lower in the S-VATS group (OR = −0.40, CI = −0.69, 0.11; P = .006) (Fig. 3B).
(5) Postoperative LOS: Postoperative LOS in 33 studies was significantly lower in S-VATS group (OR = −0.33, CI = −0.52, −0.36; P ≤ .00001) (Fig. 3C).
(6) Postoperative pain: On day 1, visual analogue scale (VAS) pain score was reported in 17 studies. S-VATS showed significantly lower rates of postoperative pain than C-VATS (OR = −0.95, CI = −1.37, −0.53; P ≤ .00001) (Fig. 3D).
Forest plot of comparison of S-VATS versus C-VATS:
Mortality (30 days/in-hospital)
There was no statistical difference in mortality rates between both groups (RD = −0.00, CI = −0.01, 0.00; P = .83) (Supplementary Fig. S3).
Funnel plots comparing the S-VATS versus C-VATS regarding different outcomes (chest tube drain, blood loss, length of stay and postoperative pain) are shown in Supplementary Figure S4.
Leave-one-out analysis of complications rate in all studies is shown in Supplementary Figure S5.
Discussion
In this study, we tested the hypothesis that S-VATS has better or at least similar postoperative results in comparison with C-VATS. This meta-analysis included 39 high-quality studies, being the largest meta-analysis about this topic up to date. To maximally curtail the potential for bias, we aimed at tight inclusion criteria in the form of only best evidence full studies published in English in PubMed archive. The NOS was calculated for each study and all of them were given at least a score of 7.
POD 1 was reported in 17 studies. S-VATs showed significantly lower rates of postoperative pain than C-VATS, which is concordant to prior meta-analysis. 51 This could be attributed to the nature of S-VATS procedures with minimal pleura and thoracic wall trauma. Moreover, in S-VATS procedures, the manipulation of intrathoracic structures is similar to that of open surgery. C-VATS, in contrast, frequently demands excessive manipulation of intrathoracic structures, another factor that may aggravate operative trauma and postoperative pain.4,7
The rate of complications after S-VATS was not significantly different from that of C-VATS. These results conform to the findings in prior studies.8,51 However, Harris et al. found that complications were significantly lower in the S-VATS group for lung cancer patients undergoing lobectomy. 52 In our study, subgroup comparison of the complications rate in lung cancer and other/mixed lung lesion studies did not show any significant differences between the comparative arms in both subgroups. Similarly, no difference was identified in the complications rate among the matched studies. These findings run in parallel to a prior study. 51
The absence of a significant difference in the number of retrieved LNs suggests that this technique does not compromise the oncological outcomes of the procedure, as long as the proper technique is applied.
Operative time, reported in 31 studies, was not significantly different as well. This finding was also affirmed by prior published studies.6,51,53,54 However, we believe that these results could be further improved with time due to the learning curve effect and the differences in expertise among surgeons from the different institutions across the globe. In the literature, the new advancements in biotechnology have enabled S-VATS to technically mimic the situation of open surgery, 54 which could, theoretically, be translated into shorter operative time. This view could also be supported by previous literature that addressed the learning curve in S-VATS. 55 We believe that more studies comparing operative times could be able to better answer this question.
Chest tube duration was significantly shorter in the S-VATS group in 24 studies. Despite that Yang et al. 8 and Qin et al. 56 did not find a significant difference in the total duration of chest tube drainage, Akter et al., 51 Xu et al., 54 and Harris et al. 52 reported results similar to ours. We believe that the reason for this finding is not clear. Additional factors should be considered including the total number of chest tubes used during the procedure and surgery location (thoracic versus mediastinal). In a previous trial, 57 postoperative drainage using a single chest tube was found to be as effective as using two chest tubes after C-VATS procedures but resulted in a significant reduction of drainage time. Since the total number of chest tubes used in both groups was frequently not reported, we believe that this could be a confounding factor for these results. New prospective trials will probably be needed to verify whether this benefit can be attributed to the number of chest tubes or to the VATS approach.
Blood loss in 17 studies was significantly lower in the S-VATS group. This was similar to the results reported by Harris et al. in eight studies 52 That could be attributed to better handling of tissues in S-VATS than in C-VATS with less portal entry-site bleeding.
Postoperative LOS in 33 studies was significantly lower in S-VATS. Compared with Akter et al. results, 51 who did not find a significant difference regarding this variable, our results were similar to earlier results.6,51,53,54
These findings are probably largely due to shorter drainage times and subjective less postoperative pain associated with S-VATS. However, these studies did not report whether the fast tracking protocol was used, a factor that should be taken into consideration before attributing these results to S-VATS.58,59
Conducting statistical analysis on this large number of patients was not able to find any differences between both groups regarding mortality or morbidity rates during the perioperative period. S-VATS has resulted in less postoperative pain, blood loss, LOS, and chest tube duration. In lung cancer patients, the number of retrieved LNs was similar to that of C-VATS.
The findings reported in this study are limited to the available data from the included studies. Many of these studies are retrospective in nature, and hence are missing essential information needed for further validation of the benefits of S-VATS over C-VATS, such as the total number of chest tubes used and whether those patients were enrolled in a fast tracking protocol or not. Another limitation to this study is that long-term pain outcomes could not be assessed due to variability in measurement systems or the timing of assessment. We tried to use the most homogeneous data, and POD 1 measured using VAS score was the most frequently reported finding. New trails addressing long-term pain outcomes would be valuable. However, since early postoperative pain is one of the major complications after thoracic surgery, we believe that the S-VATS technique can be advocated as a better surgical option. When feasible, this technique will help minimize trauma to patients and save valuable hospital time and resources.
Conclusion
Uniportal VATS technique, when appropriately indicated and performed, has shown superior postoperative outcomes to the C-VATS in the treatment of both minor and major lung disorders.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.