
Abstract
Abstract
Introduction:
The timing of surgical intervention in the management of spontaneous pneumothorax remains controversial. The aim of this multicenter review was to compare management strategies and outcomes in children with spontaneous pneumothorax.
Methods:
We retrospectively reviewed patients 10–19 years old in the Pediatric Health Information System admitted for spontaneous pneumothorax from 2010 to 2014. Three treatment groups were identified based on initial hospital management—no intervention, initial chest tube placement, and operation; and outcomes were compared.
Results:
A total of 1040 patients were included. The majority were male (82.1%) and White (71.1%). The mean age at first encounter was 15.7 ± 1.7 years. Initial treatment included no intervention in 336 (32.3%), chest tube in 497 (47.8%), and video-assisted thoracoscopic surgery (VATS) in 207 (19.9%). Ultimately, 417 (40.1%) patients underwent VATS during the initial admission and 559 (53.8%) during the initial admission or a subsequent encounter. Aggregate length of stay (LOS) was highest for those treated initially with chest tube alone (P < .001). For patients managed initially with chest tube, the probability of requiring surgery increased with each day of hospitalization. Initial operation was associated with a decreased risk of readmission (OR 0.67, 95% CI 0.50–0.90). Estimated adjusted hospital costs, aggregated across all encounters, were highest for chest tube alone (P < .001).
Conclusion:
Early VATS is associated with decreased hospital LOS, charges, and readmissions. For those managed initially with chest tube alone, the likelihood of requiring operation increases with each day hospitalized, and early conversion to operative management should be considered in patients with persistent pneumothorax or air leak.
Introduction
S
There are no evidence-based pediatric-specific guidelines for the management of spontaneous pneumothorax and it remains unclear whether adult guidelines are applicable to children. 2 The effectiveness of surgery in preventing recurrence and the timing of intervention also remain controversial. There are three general approaches to the initial management of a patient with spontaneous pneumothorax—no intervention, drainage through needle aspiration or chest tube placement, or immediate operation, most commonly in the form of video-assisted thoracoscopic surgery (VATS). Single-institution retrospective reviews have shown that nonoperative management is associated with a recurrence rate as high as 57%3–6 and that shorter length of stay (LOS) is achieved when surgery is performed initially rather than after failure of nonoperative management.4,7 In contrast, there are costs and potential complications associated with VATS and a nontrivial recurrence rate even after surgery, so many clinicians prefer a conservative management approach for initial episodes. The majority of patients currently undergo initial nonoperative management with chest tube placement alone. 7
Given the limitations of single-institution reviews, this study aims to compare outcomes and resource utilization among patients with spontaneous pneumothorax who underwent nonoperative management, chest tube placement, or operation within the initial 24 hours of admission using a large national database. A secondary aim is to determine the likelihood of operation before discharge for each consecutive day of hospitalization for nonoperative therapy. We hypothesized that recurrence, readmission, and resource utilization would be lowest in those who had early operation and that the likelihood of surgery before discharge for patients managed initially with chest tube alone increases with each day they remain hospitalized.
Methods
Data for this study were obtained from the Pediatric Health Information System (PHIS), an administrative database that contains inpatient, emergency department, ambulatory surgery, and observation encounter-level data from over 45 not-for-profit, tertiary care pediatric hospitals in the United States. These hospitals are affiliated with the Children's Hospital Association (Overland Park, KS). Data quality and reliability are assured through a joint effort between the Children's Hospital Association and participating hospitals. Portions of the data submission and data quality processes for the PHIS database are managed by Truven Health Analytics (Ann Arbor, MI). For the purposes of external benchmarking, participating hospitals provide discharge/encounter data, including demographics, diagnoses, and procedures. Nearly all of these hospitals also submit resource utilization data (e.g., pharmaceuticals, imaging, and laboratory) into PHIS. Data are deidentified at the time of data submission, and data are subjected to a number of reliability and validity checks before being included in the database. For this study, data from 45 hospitals were included. Institutional Review Board exemption was obtained for this study from the Ann & Robert H. Lurie Children's Hospital of Chicago.
In this study all patients aged 10–19 years old with a diagnosis of spontaneous pneumothorax from January 1, 2010 to December 31, 2014 were included. The International Classification of Diseases, Ninth Revision (ICD-9) codes used to identify spontaneous pneumothorax were 512.0, 512.81, 512.83, and 512.89. Procedures/operations were captured using ICD-9 procedure codes: 34.04, 32.20, 32.21, 32.29, 32.3, 32.39, 34.51, 34.59, 34.52, 34.29, 34.28, 34.6, and 34.21. Chest tube placement based on ICD-9 procedure code (34.04) was found to be incomplete and was therefore captured using either the ICD-9 code or Clinical Transaction of Care (CTC) code for chest tube or Pleur-evac. Hospitals were excluded from analysis if PHIS captured supply charges for Pleur-evac or chest tube placement in <10% of cases. Chest computed tomography scan (CT scan) utilization was identified using ICD-9 procedure code (87.41) or imaging CTC codes (4330–4339, 4399 with technique = 51).
Demographic data were extracted, including age, sex, race, and ethnicity. Comorbidities were also identified. The primary outcome measure was surgery either during the initial admission or a subsequent encounter. Secondary outcome measures included CT utilization, LOS, readmissions (including both emergency department and inpatient visits), reoperations, and total hospital estimated costs. Patients were analyzed according to the initial management strategy during hospital day 0 or 1 into three groups—no intervention, chest tube alone, or operation (VATS). Descriptive analysis of demographic data was performed and reported as means, medians, and frequencies. Univariate analysis was performed using chi-square test or analysis of variance. Multivariate analysis was performed to test the association of readmissions with initial operation using a logistic regression controlling for comorbidities and chest CT scan utilization. For patients who underwent initial chest tube placement, the cumulative chance of requiring operation was calculated for each day that patients remained hospitalized. IBM SPSS Statistics for Windows, version 24, was used for analysis, and a P value <.05 was considered statistically significant.
Results
Patient characteristics
A total of 1040 patients from 36 pediatric hospitals had an inpatient admission for spontaneous pneumothorax meeting inclusion criteria during the study period, 2010–2014. The majority of patients were male (82.1%), White (71.1%), and non-Hispanic (84.8%). The mean age at first encounter was 15.7 ± 1.7 years (median 16). Most patients (68.2%) were admitted through the emergency department on their first encounter. Comorbidities included asthma in 129 (12.4%) and cystic fibrosis in 29 (2.8%).
Initial treatment (on hospital day 0 or 1) included no intervention in 336 (32.3%), chest tube in 497 (47.8%), and operation in 207 (19.9%). Ultimately, 417 (40.1%) had surgery during the initial admission and 559 (53.8%) either during the initial admission or a subsequent encounter.
CT scan utilization
During their first encounter, 334 (32.1%) patients had a CT scan. There was no difference in CT scan utilization between the three initial treatment groups. However, among patients who had a CT, 185 (55.4%) underwent an operation during the initial encounter compared to 232 (32.9%) who did not have a CT (P ≤ .001). The readmission rate was no higher for patients who did not have a CT during their initial admission (23.7%) compared to those who did undergo CT (26.2%) (P = .40).
Length of stay
Initial hospital LOS was longer with either intervention (chest tube or operation) compared to no-intervention (P < .001). When analyzing aggregate LOS over all encounters for pneumothorax, the LOS was similar in those treated initially with operation or no-intervention, but higher for those treated initially with chest tube alone (P < .001) (Table 1).
VATS, video-assisted thoracoscopic surgery.
Likelihood of surgery by hospital day
Among the 497 patients managed with chest tube alone in the first 24 hours, 157 (31.6%) underwent operation at some point before discharge. These operations were performed on hospital day 2 in 29 (18.5%), day 3 in 33 (21.0%), day 4 in 21 (13.4%), day 5 in 22 (14.0%), and day 6–30 in 52 (33.1%). For patients managed initially with chest tube alone, the probability of requiring surgery was 36% if they remained hospitalized on day 3, 46% on day 4, 55% on day 5, and 62% on day 6 (Fig. 1).
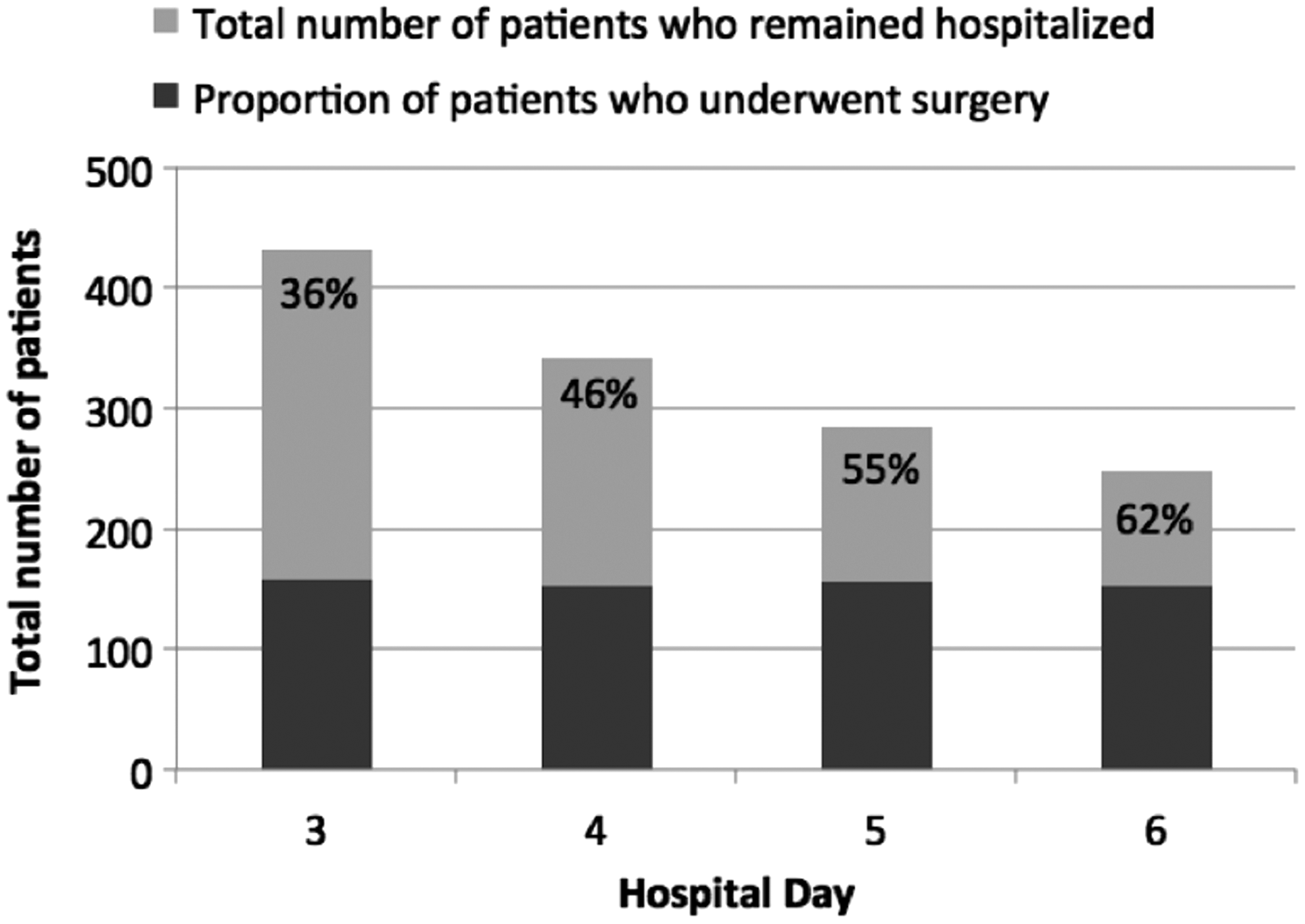
Probability of undergoing operative intervention for patients managed initially with chest tube who remain hospitalized on each respective day.
Readmissions
Patients who were treated with initial operation within 24 hours had a trend toward lower readmission rate than those treated nonoperatively or with chest tube alone but this was not statistically significant on univariate analysis (P = .08) (Table 1). However, among those who received an operation during the first admission (regardless of timing), the readmission rate was 87/417 (20.9%) compared to 177/623 (28.4%) among those who did not (P = .007). In a multivariable logistic regression, controlling for patient risk factors (asthma and cystic fibrosis), as well as for CT scan utilization, operation during the first encounter was associated with a decreased risk of readmission (OR 0.67, 95% CI 0.50–0.90).
Reoperation rate
Among those treated initially with operation, the reoperation rate was 9 (4.3%) during the initial encounter and 28 (13.5%) across all readmission encounters. Laterality could not be determined in the PHIS database, so a fraction of these reoperations were likely on the contralateral side.
Hospital costs
Estimated adjusted hospital costs, aggregated across the initial and readmission encounters, were $16,523 for no intervention, $24,178 for chest tube alone, and $20,374 for operation (P < .001) (Table 1).
Discussion
This study has shown that most patients with spontaneous pneumothorax undergo chest tube placement as initial management in the first 24 hours, but the majority will ultimately require surgical intervention. The readmission rate was lowest in those who had an operation during the first admission, and total hospital LOS across all admissions was longest in those who had chest tube placement alone. This study also showed that the likelihood of surgery increases with each day of hospitalization for those managed with chest tube alone.
The majority of patients in this analysis, as in prior studies, underwent initial nonoperative management. In a single institution review by Qureshi et al., nonoperative treatment was attempted in 37 of 51 pneumothoraces, 20 of which recurred requiring VATS. 4 In a similar review by Lopez et al., 98 of 108 pneumothoraces were initially managed conservatively, with a recurrence rate of 40%. 7 Initial nonoperative management was performed in 80% of patients in our population, including 336 who received no intervention and 497 who underwent chest tube placement.
CT scan utilization in the current study was highly variable, reflecting the controversy over the value that it adds for clinical decision-making. There was no difference in CT utilization among patients treated initially with no intervention, chest tube, or VATS. However, patients who underwent CT were more likely to undergo surgery before discharge. Fewer than one-third of patients underwent CT, which is lower than rates reported in studies of adults with PSP.2,8 The rationale for avoiding CT in children cannot be determined, but may include a desire to avoid ionizing radiation in children or a belief that CT findings do not affect clinical decision-making. Clinicians favoring CT in the initial workup argue that it can identify blebs in the contralateral lung, which can guide patient/parent counseling regarding recurrence, and also that it rules out secondary pathological conditions, which may have caused the pneumothorax. 2 In one review, 40% of those with contralateral disease on CT developed a pneumothorax in the subsequent 6 months. 2 However, it is still not clear whether this mandates intervention if the patient is asymptomatic on that side. Furthermore, since histology confirms blebs in nearly all patients who undergo operative intervention, 2 there seems to be limited utility in demonstrating blebs preoperatively. In another review by Laituri et al., almost 80% of patients with negative scans were found to have blebs intraoperatively suggesting that the sensitivity of CT for detecting blebs is low. 8 Some investigators have suggested that the presence of blebs on CT is predictive of ipsilateral recurrence, whereas in other studies this has not held true.9,10
The correlation between initial management and hospital LOS is also poorly understood. While most patients remain hospitalized for several days following operative management, this is counterbalanced by the hospital days associated with persistent air leak in patients managed with chest tube alone. In a review of the literature by Chambers and Scarci, VATS was associated with decreased LOS compared to chest tube drainage alone. 3 Similarly, Lopez et al. found that initial nonoperative management was associated with increased LOS compared to primary surgery. 7 Qureshi et al. found that total treatment LOS was shorter for primary VATS compared to VATS done only after recurrence. 4 Our study showed that total hospital LOS across all encounters for spontaneous pneumothorax was highest in those who had chest tube alone as initial management. Persistent air leakage after chest tube placement likely contributes to the increased LOS. The definition of a persistent air leak ranges in the literature from 3 to 5 days7,11,12 and there are no evidence-based guidelines on the duration of air leak after which operative intervention is required. O'Lone et al. suggested that surgical intervention is likely to be required for a leak persisting for longer than 5 days, 11 while Granke et al. suggest earlier intervention at 3 days. 12 However, persistent air leakage signaling failure of nonoperative management has been identified as a factor associated with proceeding to surgery.7,13,14 A decision for early operation in patients with persistent air leak after chest tube placement may reduce the period of preoperative hospitalization and total cost. This study has also demonstrated the likelihood of surgical intervention increases with each day that patients with a chest tube remain hospitalized, further underscoring the rationale for earlier definitive surgical intervention.
A multitude of factors have been reported to correlate with recurrence risk, including initial management approach, patient factors, and operative technique. Our findings correlate with prior reports demonstrating a reduced recurrence risk in children who undergo VATS compared to nonoperative management. Lopez et al. found a recurrence rate of 40% after nonoperative management compared to 15% after surgery. 7 Similarly Noh et al. demonstrated lower recurrence rates after surgery compared with observation or chest tube placement and interestingly found that recurrence was higher in younger age groups, particularly those less than 16 years old. 15 Other studies have also found that younger age is associated with higher recurrence rates.16,17 The correlation between operative technique and recurrence rates remains very controversial. Different surgeons utilize various approaches, including combinations of wedge resection, pleurectomy, pleural abrasion, chemical pleurodesis, and staple line covering. In a systematic review of 51 studies by Sudduth et al., wedge resection and chemical pleurodesis, with or without pleural abrasion, were associated with the lowest recurrence rate, 18 while Joharifard et al. found lower recurrence rates with pleurectomy compared to pleural abrasion. 19
Differences in LOS, recurrence, and operative utilization in the different management groups all contribute to variation in costs and charges. Our study examined aggregate estimated costs across all encounters for spontaneous pneumothorax and found significantly higher costs associated with initial management by chest tube alone. This was attributed to longer hospital stay and eventual need for surgery in those who were initially managed nonoperatively. In a cost-benefit analysis of primary versus delayed VATS for spontaneous pneumothorax, Qureshi et al. found that the charges associated with primary versus delayed VATS were not significantly different, but that if the charges for surgery on the 46% of patients who did not recur were considered, performing primary VATS on all patients would increase the total charges by $4010 per patient. 4 Cook et al. also concluded that it was most cost-effective to perform surgery only after the first recurrence of spontaneous pneumothorax and not on the initial admission. 6 However, both these studies, like ours, used charge data, which does not always accurately reflect actual hospital costs. Lopez et al., using direct measures of cost, found that initial nonoperative management had lower median direct costs than initial surgery, but that there was no difference in cost between primary and delayed surgery. 7 Given that LOS influences cost in the earlier resource-intensive periods of hospitalization, 20 we believe that earlier surgical intervention on the first admission for those who are more likely to fail nonoperative management may serve to lower overall expenditure.
We acknowledge the limitations of this study. Inherent to the retrospective examination of an administrative database is the lack of clinical data on such factors as provider decision-making and the clinical status of the patient, which may have influenced the decision to intervene surgically. We were unable to determine which patients may have had a persistent air leak or residual pneumothorax on imaging, factors that influence clinical decision-making. Similarly, the database does not provide historical information on whether this was the first episode of pneumothorax in the patients included. Furthermore, this study only captured data from children's hospitals which participate in PHIS. Adolescents with PSP are frequently treated at adult institutions, where management patterns may be very different. As such, the generalizability of our findings is restricted. Likewise, an unknown proportion of these patients may grow out of pediatric care and transition to adult institutions so that they are lost to pediatric follow-up, which may affect the accurate assessment of recurrence rates.
Despite these limitations, we believe that this study highlights the management and associated outcomes of spontaneous pneumothorax on a national level, providing evidence favoring earlier identification and surgical intervention for those patients who are likely to fail nonoperative management. Determining the factors that allow providers to identify these patients within the first few days of admission would facilitate earlier intervention and should be a focus of future prospective studies.
Conclusion
Many children with small pneumothoraces do well with no intervention. For those requiring any intervention, the majority ultimately requires VATS. Early VATS decreases hospital LOS, charges, and readmissions. For those managed initially with chest tube alone, the likelihood of requiring operation increases with each day hospitalized and early conversion to operative management should be considered.
Footnotes
Acknowledgments
The authors express sincere gratitude to the members of the Pediatric Health Research Outcomes Group for Surgery at Ann & Robert H Lurie Children's Hospital of Chicago for assistance in data analysis. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' Contributions
T.A.O. and T.B.L. conceptualized the project, performed data analysis, and supervised the preparation of the article. K.W. was the primary author of the article. G.H. performed data analysis and drafting of the article. R.J.H., T.B.L., and T.A.O. provided final editing of the article.
Disclosure Statement
No competing financial interests exist.