
Abstract
Abstract
Introduction:
Laparoscopy-assisted gastrectomy (LAG) is a minimally invasive procedure for the treatment of gastric cancer. It is generally thought that a minimally invasive technique results in less visible blood loss during the surgery. Nevertheless, a meaningful perioperative hidden blood loss (HBL) is often ignored. In this study, we investigated the amount of HBL and the influential factors after LAG for gastric cancer.
Methods:
A retrospectively analyzed clinical data of 62 consecutive patients who underwent laparoscopy-assisted total or distal gastrectomy at our center from May 2016 to May 2017. The HBL was calculated according to Gross's and Nadler's formula. The data of patient gender, age, height, weight, body mass index, preoperative and postoperative hematocrit, postoperative drainage, albumin loss, diabetes mellitus, and hypertension were analyzed by multivariate linear regression analysis. The type of surgical reconstruction was analyzed by one-way analysis of variance. The difference between the preoperative blood pressure and postoperative blood pressure was measured by paired sample t-test and boxplot.
Results:
The HBL was 322.2 ± 195.9 mL (64.3% ± 14.1% in total blood loss [TBL]), the TBL was 475.6 ± 222.8 mL, and the hemoglobin (HB) loss was 15.0 ± 8.7 (11.5% ± 6.1% of HB level loss). Multivariate linear regression analysis revealed that gender, hypertension, and albumin loss between preoperation and postoperation are influential factors of HBL in patients after LAG for gastric cancer. Compared to male patients, female patients are positively associated with HBL.
Conclusion:
In our study, we found HBL is a significant segment of TBL and is much larger than what we considered previously in LAG for gastric cancer. Gender, hypertension, and albumin loss are significantly correlated with HBL. Therefore, paying attention to HBL is significant for promoting clinical treatment and ensuring patients' safety.
Introduction
T
The concept of HBL was put forward in 2000 by Sehat et al. 7 and has received increasing attention in recent years. Sehat et al. 8 found that HBL accounts for 49% of the amount of total blood loss (TBL) after total knee replacement. This phenomenon gives us ample reasons to bring HBL to the attention in clinical practice. However, only orthopedic surgeons have been concerned about HBL over the past years; as far as we know, there is still no published study that has examined the issue of HBL in LAG for gastric cancer.
In this study, we performed a retrospective review investigating the amount of HBL and analyzing the influential factors of HBL after LAG for gastric cancer.
Materials and Methods
Patients
A total of 62 patients (including 42 males and 20 females) with a complete history of disease and average age of 62 (42–85) years were recruited in this study. All the patients underwent laparoscopy-assisted total or distal gastrectomy at Wenzhou Medical University from May 2016 to May 2017. The data of patient gender, age, height, weight, body mass index (BMI), preoperative and postoperative hematocrit (HCT) and hemoglobin (HB), postoperative drainage, diabetes mellitus, hypertension, and type of reconstruction were recorded. All patients had no blood transfusion in this study. Patients who had history of hematological diseases were excluded from the study.
Management of blood loss, blood pressure and heart rate
Intraoperative blood loss (IBL) was assessed by measuring the amount of blood in the suction bottle, which does not include the rinse fluid, and by weighing the sponges used during the surgery. Postoperative blood loss (PBL) was calculated by measuring the amount of fluid in the drainage bottle after 48 hours. Blood routine examination, blood biochemical item, systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate before the surgery and on the third postoperative day were recorded, because the patient's hemodynamics tend to stablize during this time.
Calculation of HBL
The patient's blood volume (PBV) was calculated by Nadler's formula 9 : PBV (L) = k1 × height (m)3 + k2 × weight (kg) + k3, (k1 = 0.3669, k2 = 0.03219, and k3 = 0.6041 for male; k1 = 0.3561, k2 = 0.03308, and k3 = 0.1833 for female).
The TBL in the perioperative period was calculated by Cross's formula 10 : TBL (L) = PBV (L) × (Hctpre − Hctpost)/Hctave, where Hctpre is preoperative HCT, Hctpost is the HCT on the third postoperative day, and Hctave is the average of Hctpre and Hctpost.
Finally, HBL can be calculated as follows: HBL = TBL − (IBL + PBL).
Statistical analysis
Multivariate linear regression analysis was used to evaluate the influential factors of HBL, including six quantitative variables (age, BMI, the changes of preoperative and postoperative SBP, DBP, heart rate, and albumin loss) and three qualitative variables (gender, hypertension, diabetes mellitus, and type of reconstruction). In the qualitative variables, male, hypertension, and diabetes mellitus were set as “1.” Female, nonhypertension, and non-diabetes mellitus were set as “0.” A positive coefficient indicates a positive influence on the dependent variable (HBL), whereas a negative coefficient indicates a negative influence. One-way analysis of variance (ANOVA) was performed to find out the relative correlation between HBL and the type of surgical reconstruction. The independent sample t test was used to evaluate the relationship between age and HBL, TBL, and postoperative hospital stay. The difference between the preoperative blood pressure and postoperative blood pressure was measured by paired sample t test and boxplot. SPSS 19.0 software was used for all statistical analyses. P value <.05 was considered significant.
Results
From May 2016 to May 2017, a total of 62 patients were treated by LAG for gastric cancer. All demographic data of patients are summarized in Table 1. The data for IBL, postoperative suction drainage, preoperative albumin, postoperative albumin, albumin level loss, HB loss, HB level loss, HCT level loss, TBL, HBL, and percentage of HBL in total are shown in Table 2. The TBL was 475.6 ± 222.8 mL, the HB loss was 15.0 ± 8.7 g/L (11.5% ± 6.1% of HB level loss), the albumin level loss was 19.5% ± 8.1%, and the HBL was 322.2 ± 195.9 mL (64.3% ± 14.1% in TBL), indicating a considerable amount of HBL.
Data are mean ± SD.
BMI, body mass index; SD, standard deviation.
Data are mean ± SD.
To examine the association between HBL and five influential factors as mentioned earlier, we performed multivariate linear regression analysis. As shown in Table 3, hypertension (P = .027) and albumin loss (P = .001) were positively correlated with HBL. Meanwhile, we found that compared to male patients, female patients were positively associated with HBL (P = .046). However, it appeared that age (P = .854), BMI (P = .307), diabetes mellitus (P = .4), the changes of preoperative and postoperative SBP (P = .137), DBP (P = .122), and heart rate (P = .414) were not significantly correlated with HBL.
P < .05.
DBP, diastolic blood pressure; SBP, systolic blood pressure.
As shown in Table 4, one-way ANOVA revealed no significant correlation with HBL among different types of surgical reconstruction of LAG for gastric cancer (P = .094). As shown in Table 5, independent sample t test revealed that patients older than 70 years had greater HBL (P = .274) than patients younger than 70 years, and had longer postoperative hospital stay (P = .013). Patients' blood pressure was significantly decreased after LAG, as shown in Table 6 and Figure 1.
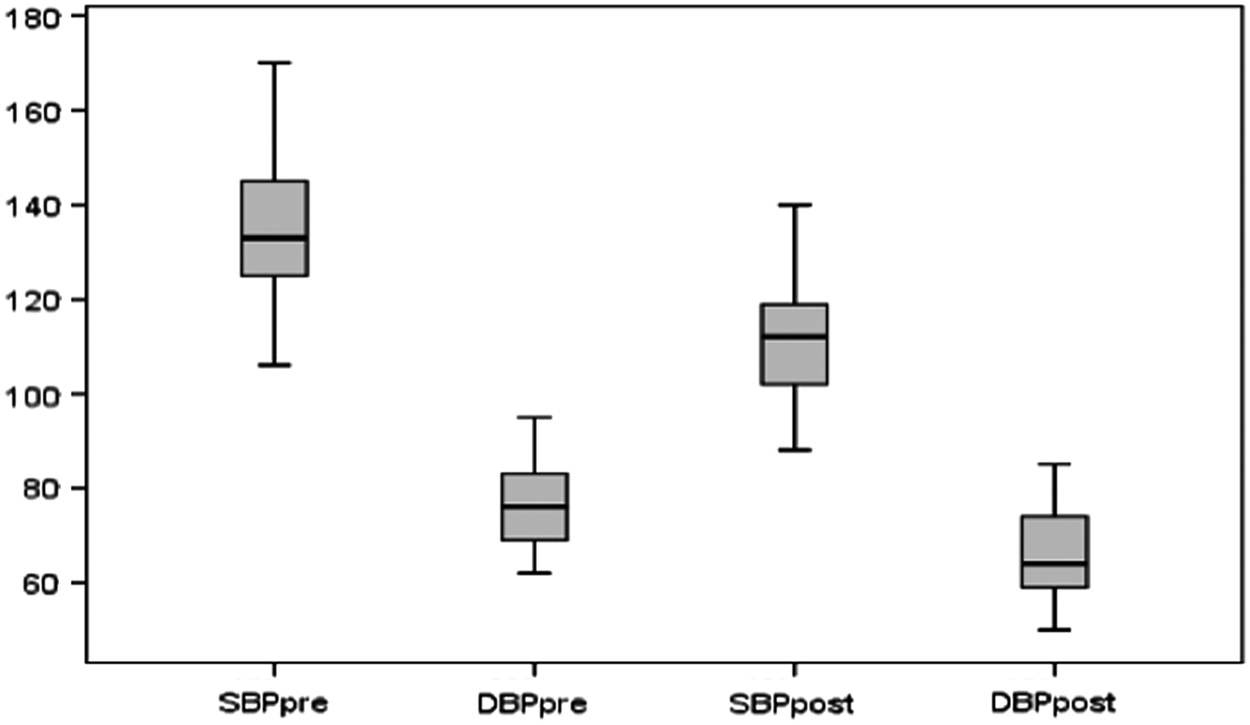
The boxplot of the SBP and DBP for preoperative and postoperative period. DBP, diastolic blood pressure; SBP, systolic blood pressure.
Data are mean ± SD.
Data are mean ± SD
P < 0.05.
Data are mean ± SD.
P < .01
Discussion
Over the past years, LAG has spread globally and is within reach for many general hospitals. Owing to its small surgical incisions and less visible blood loss, HBL is usually ignored in LAG, especially when the clinical symptoms of anemia are not obvious. In this study, we performed a retrospective investigation on 62 consecutively enrolled LAG patients to estimate the amount of HBL and the influential factors.
Sehat et al. reported that HBL accounts for 49% of the amount of TBL after total knee replacement. 7 Similarly, in this study, we found the amount of HBL was 322.2 ± 195.9 mL, with a percentage of 64.3% ± 14.1% in TBL during the perioperative period, indicating a considerable amount. In addition, when we study the association factor, our results showed that gender and hypertension are correlated with the HBL after LAG for gastric cancer. Obviously, the collected relative data will affect the result of HBL. Postoperative HCT is one of the most significant reference indexes to calculate the HBL. Based on consecutively 7 days of preoperative and postoperative blood routine examination, we found that the lowest HCT value occurs on the third day after operation in most patients. Therefore, we used the HCT value on the third postoperative day to calculate the HBL. Presently, the exact mechanisms of HBL are not fully determined. Pattison et al. examined that blood loss was mainly caused by a hemolytic or redistributive process. 11 Erskine et al. reported that blood loss was mainly caused by a large amount of blood into the tissue gap in the perioperative period. 12 It is generally considered that older patients with anemia have a higher risk of death than normal hemochromatosis patients in the perioperative period.13,14
Miao et al. reported that the amount of HBL is associated with age following total hip arthroplasty. 15 However, our results showed that age is not correlated with the HBL after LAG for gastric cancer. Nevertheless, in our study, we found that patients older than 70 years had greater HBL than patients younger than 70 years, and had longer postoperative hospital stay (P < .05). After analyzing the reasons, we consider that HBL has the following effects on elderly patients: (1) excessive HBL will activate the sympathetic-adrenal medullary system, which will aggravate the heart load, inducing the original or underlying heart disease, which directly or indirectly affects the recovery of patients. (2) HBL can lead to malnutrition in the body; the body's skin and muscle will suffer the insufficiency of blood supply and oxygen supply, which will affect the wound healing and increase the risk of infection. (3) Excessive HBL will lead to the disorder of electrolyte and milieu interior that might threaten the patient's life. In summary, we consider that paying more attention to HBL for elderly patients is meaningful.
Prasad et al. demonstrated that the increase in BMI did not cause more HBL in total knee arthroplasty. 16 Similarly, in our study, there is no evidence that the amount of HBL is associated with BMI. This result from our study supports the conclusion in the study by some scholars that obesity does not cause higher IBL and obesity is not a risk factor for postoperative morbidity after LAG.17–20
Hypoproteinemia is associated negatively with dehiscence of the wound, wound infection, postoperative infectious complications, prolonged hospitalization, and mortality.21–25 Such associations have been partly attributed to the catabolic effects of surgical interventions and mediators of protein-caloric malnutrition on postoperative morbidity and mortality, particularly among patients with surgical tumor with gastrointestinal malignancy.22,26–28 In our study, we found that the amount of albumin loss significantly correlated with HBL (P < .01). Due to the invasion of gastric cancer, the average serum albumin in patients was only 39.2 ± 3.2 g/L (normal range: 40–55 g/L), and the albumin decreased further to 31.5 ± 3.2 g/L after LAG. Therefore, we consider that reducing HBL has a positive effect on the prognosis of patients.
Despite the reforming in surgical technique and the obvious development of chemotherapeutic drugs, the prognosis of gastric cancer remains poor, some due to frequent recurrence. Peritoneal carcinomatosis is one of the most common patterns of recurrence after gastrectomy, especially in cases of gastric cancer with serosal invasion.29,30 Some studies reported that the amount of IBL in LAG was a significant correlation with the development of peritoneal recurrence.2,31 Although the LAG is generally considered to be less visible IBL, in our study we found that the amount of HBL is much larger than visible IBL; therefore, paying more attention to HBL may be helpful in reducing postoperative peritoneal carcinomatosis. Owing to the reform in minimally invasive surgery and the timely follow-up of patients with vital signs, all patients in this study had no blood transfusion and therefore the correlation between blood transfusion and HBL cannot be assessed.
The changes of blood pressure, heart rate, and albumin loss before and after surgery demonstrated well that the actual amount of blood loss in the LAG was far greater than visible blood loss. However, heart rate and blood pressure in our study were not significantly correlated with HBL; we concluded the reasons are as follows: (1) sample volume is too small and (2) individual differences. The patient's age, cardiopulmonary function, inflammatory response, basic disease, gender, and mood have influences on the measurement of the heart rate and blood pressure.
This study also suffers from several limitations. First, our results should be verified by prospective studies with a large number of patients because the number of patients included in this study was small. Second, HBL's exact mechanism is not fully determined. Finally, other potential influential factors, such as histologic differentiation, lymphatic invasion, vessel invasion, and tumor size, which were not included in this study, need to be further determined.
Conclusion
Currently, surgeons are increasingly pursuing minimally invasive surgeries while ignoring the perioperative blood loss, especially when the patient's vital signs are relatively stable. In our study, we found that HBL is a significant segment of TBL and is much larger than what we considered previously in LAG for gastric cancer. Gender, hypertension, and albumin loss are significantly correlated with HBL in patients after LAG for gastric cancer. Additionally, patients over 70 years old should be given special attention. HBL should be monitored after surgery due to the potential adverse effects of anemia. In conclusion, paying more attention to HBL is significant for promoting clinical treatment and ensuring patients' safety.
Footnotes
Disclosure Statement
No competing financial interests exist.