
Abstract
Abstract
Background:
Traumatic thoracoabdominal injuries can involve multiple organs and multiple cavities, which increases the complexity of surgical management. Traditionally, these injuries required laparotomy and thoracotomy. However, minimally invasive intervention may be reasonable for stable patients.
Materials and Methods:
We present a case of a thoracoabdominal gunshot wound resulting in multiorgan, multicavity injury to the lung, diaphragm, and liver. We performed hepatorrhaphy and diaphragm repair, and addressed a retained hemothorax through a transabdominal laparoscopic approach.
Results:
The patient tolerated the procedure well. He required no further procedures, and had no evidence of retained hemothorax or bile leak from the liver injury. After a short stay in the hospital, the patient recovered uneventfully.
Conclusions:
In hemodynamically stable patients, the transabdominal laparoscopic approach is a feasible and effective approach to penetrating thoracoabdominal trauma.
Introduction
P
Case Presentation
A 27-year-old male was evaluated in the emergency department after he sustained a high-velocity GSW to the right chest. Paramedics reported that the patient was alert, oriented, and able to ambulate independently at the scene. On arrival to the emergency department, vital signs showed mild tachycardia at 112 beats per minute, tachypnea at 40 respirations per minute, blood pressure 124/79 mmHg, and SpO2 96% on 15 L oxygen through mask. Physical examination revealed a GSW to the right anterior chest concurrent with diminished breath sounds over the right hemithorax. No exit wound was discovered on examination. A second wound to the right shoulder was noted, causing superficial avulsion without penetrating the chest. Arterial blood gas revealed acute respiratory acidosis with pH 7.29, pCO2 52 mmHg, and base deficit of 1.5 mmol/L. Focused assessment with sonography for trauma revealed hemopneumothorax without evidence of hemoperitoneum. A 32F tube thoracostomy was inserted on the right side with return of air and ∼400 mL blood. The patient improved rapidly with chest tube placement and maintained oxygen saturation >96% on subsequent evaluations.
With these interventions, the patient remained hemodynamically stable and underwent contrasted computed tomography (CT) scan of the chest, abdomen, and pelvis that confirmed a penetrating injury that appeared to course from the medial right chest superiorly through the pectoralis muscles laterally and inferiorly causing a right hemopneumothorax, fractures of the right fifth to ninth ribs, and a grade II liver laceration at segments 7 and 8. CT revealed retention of the missile in the right flank subcutaneous tissue. Owing to the mechanism of injury, there was concern for hollow viscus and diaphragm injury at the time of examination.
Because the missile entered the right chest and traveled through the liver (Fig. 1), there was a high index of suspicion for diaphragm injury, so the patient was taken emergently for diagnostic laparoscopy. A 10 mm supraumbilical port was placed in an open manner. Pneumoperitoneum was inflated to a pressure of 15 mmHg, in a standard manner. Examination of the abdomen revealed no additional injuries other than those seen on CT. Upon identification of the diaphragm injury, pneumoperitoneum was decreased to 10 mmHg and thoracostomy collection container suction was confirmed. Pneumoperitoneum was decreased to avoid development of a tension pneumothorax. Working ports for laparoscopy were placed in a configuration similar to a laparoscopic cholecystectomy with a 5 mm mid-clavicular port and a 5 mm anterior axillary port. To pass sutures, a 10 mm subxiphoid port was inserted (Fig. 2). Placing the ports in this manner enabled observation of the chest through the diaphragm injury. The laparoscope was advanced through the diaphragm laceration for further examination of the chest; this confirmed right lower lung contusion and adequate lung inflation without tension physiology or evidence of large air leak. The laparoscope was also used therapeutically to evacuate the hemothorax under direct observation. A powered suction irrigator was inserted through the subxiphoid port, and into the thorax in a transabdominal manner. This allowed for transabdominal laparoscopic evacuation of the retained hemothorax.
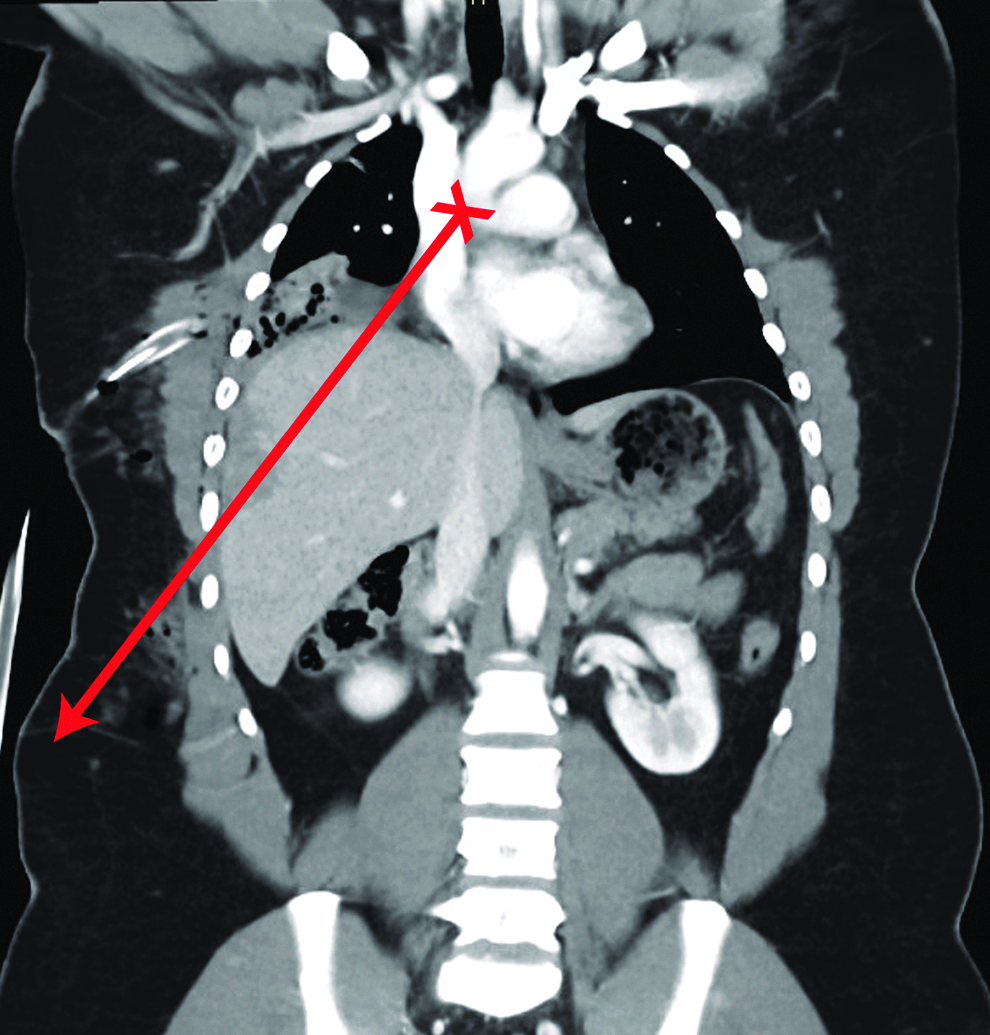
Missile trajectory shown on coronal computed tomography. “X” represents entrance wound, while the line represents the path of the missile.

Laparoscopic port placement.
Once the hemothorax was addressed, the laparoscope was retracted into the abdominal cavity for diaphragm repair. Sutures were placed at the lateral borders of the diaphragm laceration then pulled through opposite ports to proximate the edges of the injury, elevating it into view. Repair was completed with additional interrupted nonabsorbable sutures and tied using the laparoscopic knot pusher.
After diaphragm repair, a shallow grade II laceration was identified at segments 7 and 8 of the liver. Topical hemostatic agent was applied to the liver for hepatorrhaphy (Fig. 3). Before closure, hemoperitoneum was evacuated; colon and right lower quadrant were re-evaluated without identification of injury. Postoperatively, the patient had an uneventful course. No complications occurred and the patient was discharged after tube thoracostomy removal on hospital day 9.
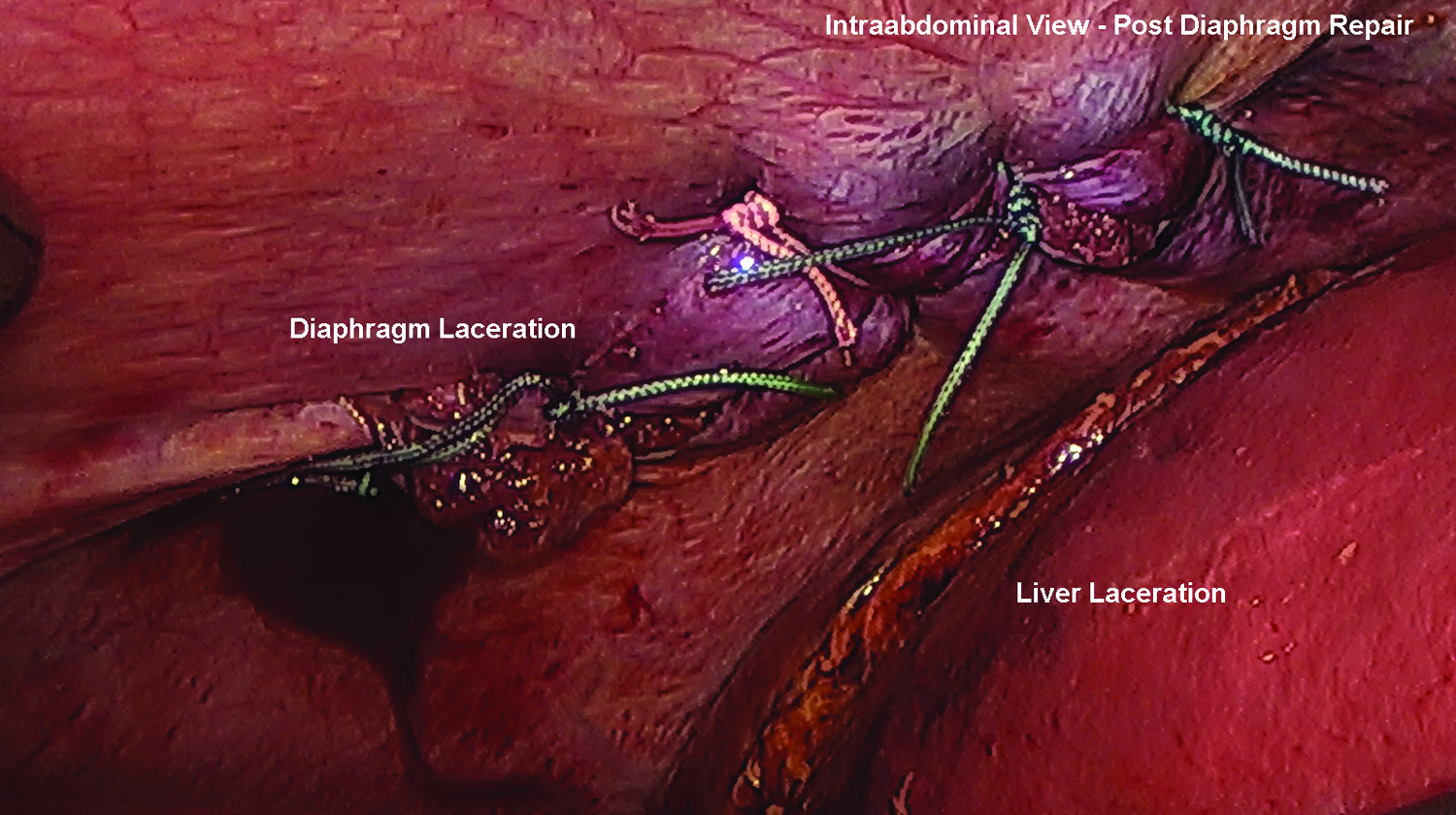
Laparoscopic view of repaired diaphragm and liver injury.
Discussion
In this case, we discuss a previously healthy 27-year-old male who suffered a high-velocity thoracoabdominal GSW. During triage, injuries to the lung and liver were identified. Potential injuries to the diaphragm and hollow viscus merited further evaluation. The patient remained hemodynamically stable throughout, and successful therapeutic intervention was achieved laparoscopically without complication.
Standard exclusion criteria for laparoscopy in trauma include abnormal hemodynamics, multiple organ involvement, and traumatic brain injuries. Although the patient remained hemodynamically stable without brain injury, he had obvious multiple organ injury that would classically preclude laparoscopic management. Because individual components of the multiorgan injury were repairable laparoscopically and the patient remained hemodynamically normal, the surgical team proceeded with diagnostic laparoscopy.
There exist multiple well-documented benefits to laparoscopy, including shorter lengths of stay, less pain, and fewer wound complications. 1 In trauma scenarios, the benefits of laparoscopy become superfluous if the patient is not stable enough to undergo pneumoperitoneum or other components of laparoscopic management. However, hemodynamically normal patients may benefit from many aspects of minimally invasive surgery.
One relative contraindication to laparoscopic management of traumatic injuries is the presence of multiorgan, multicavity trauma. Although many injuries may be laparoscopically repaired in isolation, repair of concurrent injuries is typically performed in the classic open manner. We present a successful case of a penetrating injury involving multiple organs in multiple cavities that was repaired using standard laparoscopic instruments. As minimally invasive surgery becomes more intertwined with acute care surgery, perhaps it is time to reassess whether multiorgan injury should remain a contraindication to laparoscopy.
As much as 20% of penetrating thoracoabdominal injuries include a diaphragm injury. 5 In this case, diaphragm injury was assumed based on the trajectory of the missile from the chest to the liver, despite its imperceptibility on CT scan. The merits of repairing a diaphragm laceration laparoscopically are well known. 5 Appropriately placed laparoscopic ports are critical for observation when the liver obscures the diaphragm laceration. In our case, observation of the right hemidiaphragm was best achieved with ports configured similarly to that of a laparoscopic cholecystectomy with epigastric, midclavicular, and anterior axillary ports placed along the costal margin. An enlarged 10 mm epigastric port was utilized to allow passage of suture for laceration repair (Fig. 2). In addition to the utility of the ports, this configuration has an added benefit of familiarity for the surgical team.
Using the laparoscope to evaluate the chest cavity is a novel exploratory technique that was used in this case. There is inherent risk of creating a tension pneumothorax during the inflation of the pneumoperitoneum for laparoscopy in patients with a diaphragm laceration due to the equilibration of high pressure (15 mmHg) from the peritoneum to the thorax. In this case, the patient was evaluated for pneumothorax by advancing the laparoscope from the abdomen into the thoracic cavity through the diaphragm laceration. By driving the laparoscope through the diaphragm injury and into the thorax, the surgical team directly observed the lung to confirm adequate lung inflation without tension physiology. Although unconventional, this diagnostic maneuver has low risk, high utility, and can be performed rapidly, which makes it a promising addition to the procedure regimen. Advancing the laparoscope into the thoracic cavity has the aforementioned diagnostic use, but it also has innovative therapeutic use. As is expected in a thoracic GSW, the patient had a substantial hemothorax, which was emergently treated with a chest tube. Up to 20% of GSW victims have residual hemothorax after chest tube placement, which increases the risk of subsequent empyema. 6 Both retained hemothorax and empyema require additional therapeutic procedures such as thoracotomy or thoracoscopy with drainage. In this case, the laparoscope and suction device were advanced transabdominally into the right thoracic cavity to evacuate the retained hemothorax. This technique allows the benefits of hemothorax evacuation under direct observation without the added complexity of additional ports, and without repositioning the patient in lateral decubitus position to perform thoracoscopy.
Historically, research has not shown an advantage to using laparoscopy over laparotomy in patients with multiorgan trauma. 7 However, we suspect that as acute care surgeons become more facile laparoscopically, hemodynamically normal patients may benefit from laparoscopic management of traumatic injury. Further study is warranted, and a randomized trial would be beneficial to determine the merits of laparoscopic management for multiorgan injury after thoracoabdominal trauma.
Footnotes
Disclosure Statement
No competing financial interests exist.