
Abstract
Abstract
Purpose:
To determine the clinical efficacy of preoperative coil localization-guided video-assisted thoracoscopic surgery (VATS) for lung nodules.
Materials and Methods:
Between November 2015 and July 2017, 56 patients with lung nodules underwent coil localization-guided VATS procedure. The coil implantation was performed under the guidance of computed tomography (CT). The end tail of the coil remained above the visceral pleura. The target lung nodules were removed by VATS wedge resection. Data on the technical success of coil localization and wedge resection, procedure-related complications, and pathological results were collected and analyzed.
Results:
Sixty-seven lung nodules in 56 patients (1.2 nodules/case) were localized. The technical success rate of coil localization was 89.6% (60/67). Sixty-three nodules were localized with one coil and four nodules with two coils. The mean time taken to perform CT-guided coil implantation was 15.7 ± 5.3 (range: 8–40) minutes. Six patients (9.0%) experienced pneumothorax after coil implantation. The technical success rate of wedge resection was 97.0% (65/67). Two nodules were removed directly by video-assisted lobectomy. Nine patients with multiple target lung nodules underwent single-stage resection. The mean total operating time was 147.2 ± 79.1 (range: 50–360) minutes. The mean volume of blood loss was 113.2 ± 113.0 (range: 10–700) mL. Postoperative complications included prolonged air leak (n = 2) and pleural effusion (n = 5).
Conclusions:
Preoperative coil localization is a safe and effective method to facilitate a high successful rate of VATS wedge-resection for lung nodules.
Introduction
L
Although percutaneous needle biopsy has a high diagnostic accuracy for lung nodules,2–4 some small lung nodules (≤15 mm) may be missed because of technical difficulties. 5 Surgical resection is the gold standard for diagnosis of lung nodules.6–11 Video-assisted thoracoscopic surgery (VATS) wedge-resection of lung nodules is a minimally invasive procedure that allows prompt postoperative recovery. However, some small lung nodules and sub-solid nodules are sometimes undetectable during the VATS procedure because of their size and soft nature, and cannot be removed by wedge-resection. 6
At present, preoperative localization has been widely used to facilitate VATS wedge-resection for lung nodules.6–11 The common methods of preoperative localization include methylene blue, radio-label, hookwire, and coil localization.6–11 The aim of this study is to determine the clinical efficacy of coil localization-guided VATS for lung nodules.
Materials and Methods
The protocol for this single-center retrospective study was approved by the institutional review board at our hospital. Written informed consent was obtained from all patients who participated in the study.
Patients
Fifty-six patients with lung nodules underwent coil localization-guided VATS procedure at our institution between November 2015 and July 2017. Their baseline data are summarized in Table 1. The lung nodules were detected by chest CT scan (section thickness 1 mm). The size of the lung nodules was measured on the maximal transverse diameter. The inclusion criteria were a pathologic diagnosis of an indeterminate lesion, a lesion size ≤3 cm, and a lesion-pleura distance ≤3 cm. Typical benign lesions (e.g., calcification), typical metastatic lesions, and lesions measuring less than 4 mm were excluded.
Coils
All coils were 50 mm long, 0.038 inch diameter fiber-coated microcoils (Cook, Bjaeverskov, Denmark). Each coil was loaded in a cannula (Fig. 1).
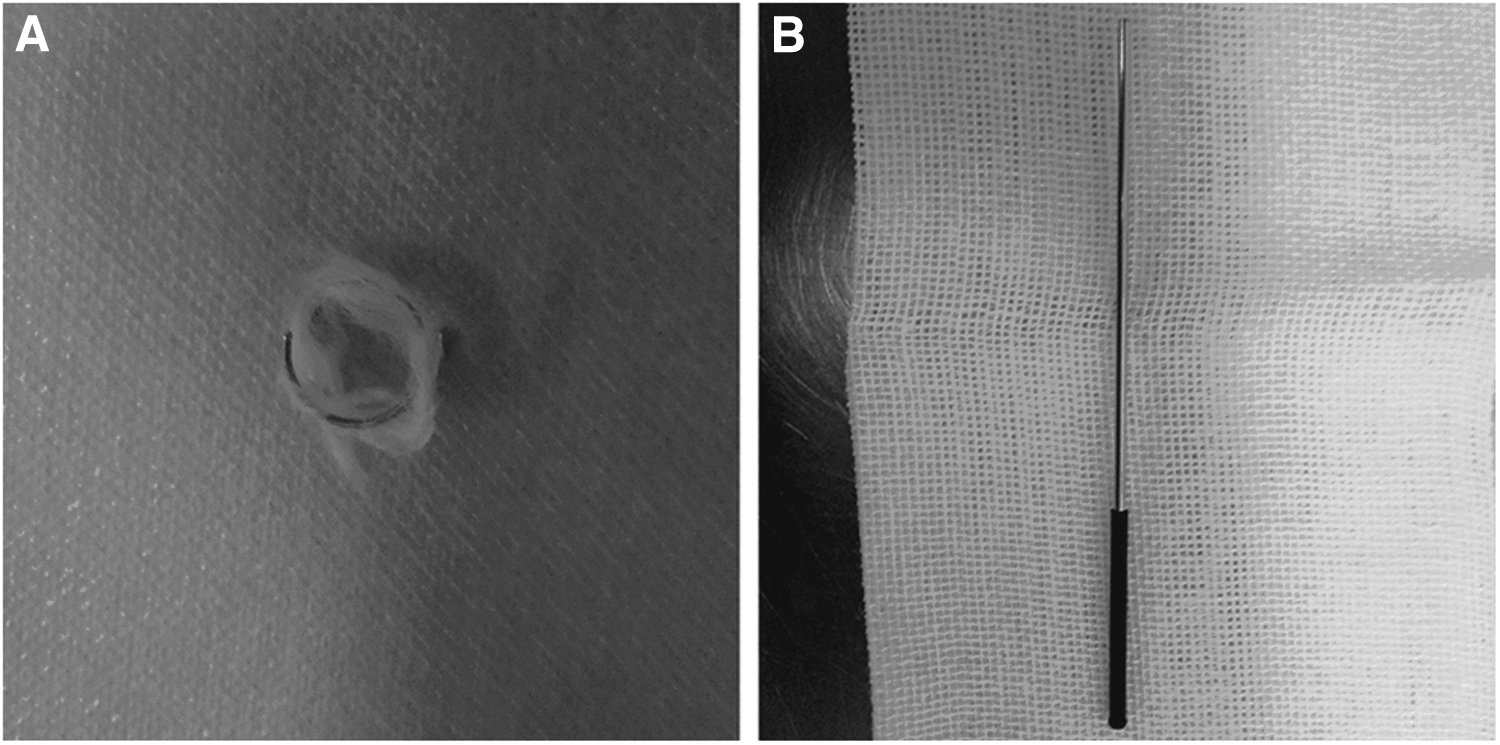
The photographs of coil
CT-guided coil implantation
All procedures were performed under the guidance of a 16-detector CT device (Philips, Cleveland, OH). The imaging parameters of the scanner were 120 kV, 150 mAs, and 2 mm section thickness.
The patients were placed in a prone, supine, or lateral decubitus position according to the location of the lesion. A thoracic CT scan was performed first to identify the needle pathway, which was selected to avoid bone, visible vessels, bullae, and fissures. The puncture site was chosen by the CT gantry laser lights and landmarks using a homemade radiopaque grid on the patient's skin. Local anesthesia was induced using 5 mL of 2% lidocaine. An 18 G coaxial needle (Precisa, Roma, Italy) was punctured into the lung and the tip of the needle was placed within 1 cm near the lesion. The core of the needle was removed and a coil was pushed into the needle sheath from the loading cannula by using the needle core. The coil was partially inserted in to the lung tissue, after which the needle sheath was removed smoothly and the end tail of the coil remained above the visceral pleura based on the distance from the lesion to the pleura (Fig. 2). Finally, chest CT was repeated to confirm the location of the coil and to check for complications.

A 64-year-old man with lung nodule underwent CT-guided coil localization.
VATS procedure
All patients underwent nonintubated uniportal VATS using a combination of target controlled sedation, intercostal nerve block, and intrathoracic vagal block within 24 hours of coil localization. All patients were placed in the lateral decubitus position, and a 3–5 mm incision was made through the fifth intercostad space along the anterior axillary line. A 10 mm video telescope (Stoze, Tuttlingen, Germany) was used to detect the pleural cavity. When the end tail of the coil was detected (Fig. 3), a wedge-shaped piece of lung tissue was removed using a stapler device (Covidien, Mansfield, MA). If the end tail of the coil could not be detected, we attempted to locate the coil by palpation. If palpation was successful, a wedge resection was undertaken, and if not, a lobectomy was performed.

The coil was detected during the VATS procedure. VATS, video-assisted thoracoscopic surgery.
When the wedge resection was complete, the lung tissue specimen was cut open to confirm that it contained the lesion. On confirmation, the lesion was sent for prompt pathologic examination. No further surgery was planned if the lesion was found to be benign, precancerous, carcinoma in situ, or a metastasis; if minimally invasive carcinoma was found additional lobectomy and systematic lymph node dissection were performed.
Definition
Coil localization was considered to be technically successful if the end tail of the coil was visible during the VATS procedure. Wedge resection was considered to be technically successful if the target lesion was identified in the wedge-shaped lung tissue. A malignant or precancerous lung nodule was considered to be a positive pathologic result and a benign lesion was considered to be a negative pathologic result.
Statistical analyses
All statistical analyses were performed using SPSS 16.0 software (SPSS, Chicago, IL). Categorical variables are compared by the chi-square test or Fisher's exact test. A p value <.05 was considered statistically significant.
Results
Coil localization
Sixty-seven lung nodules were localized in 56 patients (1.2 nodules/case; Table 2). Technical success rate of coil localization was 89.6% (60/67). Technical failure occurred in seven nodules. Six of the seven coils in the unsuccessful cases were not detected during VATS and one coil was found between the visceral and parietal pleura during the procedure.
Forty-seven patients underwent coil localization for one nodule, 7 for two nodules, and 2 for three nodules. Sixty-three nodules were localized with one coil and four nodules were localized with two coils. For the nodules requiring two coils, it was suspected on repeat chest CT that the first coil had been completely inserted into the lung tissue. The mean time taken to perform CT-guided coil implantation was 15.7 ± 5.3 (range: 8–40) minutes. Six patients (9.0%) experienced pneumothorax after coil implantation, but this did not influence the subsequent VATS procedure.
Surgical procedure
Wedge resection was technically successful in 65 nodules (97.0%). Although coil localization was unsuccessful in seven nodules, five were successfully removed by wedge resection because the coil was palpated during the VATS procedure. The remaining two nodules (one adenocarcinoma and one chronic inflammatory lesion) were removed directly by video-assisted lobectomy. Nine patients underwent single-stage resection of multiple lung nodules.
After the 65 wedge resection procedures, 33 nodules were diagnosed as malignant, 23 as benign, and 9 as precancerous. There was no significant difference in positive pathological result rates between nodules with different sizes (Table 3).
Among the 65 nodules, 21 cases were performed with subsequent lobectomy due to invasive adenocarcinoma and 1 case was performed with subsequent segmentectomy due to minimally invasive adenocarcinoma. Two patients with invasive adenocarcinoma and 1 with squamous carcinoma were not treated by lobectomy. Among the 3 cases, 2 patients declined lobectomy and 1 patient had previously undergone lobectomy for lung cancer.
The mean total operating time (including time spent waiting for an immediate pathology report) for the 56 patients was 147.2 ± 79.1 (range: 50–360) minutes. The mean volume of blood lost was 113.2 ± 113.0 (range: 10–700) mL. The postoperative complications were prolonged air leak (n = 2) and pleural effusion (n = 5).
One of the 56 patients underwent wedge resection during thoracotomy because this patient simultaneously had the mediastinal tumor and underwent single-stage resection of mediastinal tumor and lung nodule. Five patients simultaneously had lung cancer that was in a different lobe from that of the target lung nodule and underwent single-stage video-assisted resection of both lesions. One patient simultaneously had esophageal cancer and underwent single-stage resection of both lesions.
Ground-glass opacity nodules
Twenty-five ground-glass opacity (GGO) nodules in 21 patients were localized and resected. The mean diameter of these nodules was 11.1 ± 5.7 (range: 4–25) mm. The technical success rates of coil localization and wedge resection were 92.0% (23/25) and 92.0% (23/25), respectively. The mean time taken to perform CT-guided coil implantation and surgery were 15.0 ± 6.0 (range: 8–40) minutes and 147.8 ± 96.9 (range: 60–360) minutes, respectively.
Thirteen of the 25 GGO nodules were diagnosed as malignant lesions (8 as invasive adenocarcinoma and 5 as adenocarcinoma in situ), 6 as precancerous lesions, and 6 as benign lesions.
Discussion
This study determined the clinical efficacy of coil implantation-guided VATS for the treatment of lung nodules. Technical success rates of coil localization and wedge resection were 89.6% and 97.0%, respectively. The successful rate of wedge resection is comparable with that in previous studies of coil and other localization methods for lung nodules.8–11 These results may indicate that (1) CT-guided coil implantation is very effective for localization of lung nodules; (2) coil localization can facilitate a high successful rate of VATS wedge-resection for lung nodules.
Analysis of CT imaging features is the noninvasive method most commonly used for diagnosis of lung nodules.12–14 The diagnostic accuracy for malignancy ranges from 85% to 94.5%.12,13 With the development of positron emission tomography (PET)/CT, the diagnostic accuracy of lung nodules has improved further. 15 However, PET/CT has a low diagnostic sensitivity for GGO nodules. 16
Surgical resection is a management that combines diagnosis and treatment. With the development of VATS, thoracotomy is seldom used for removal of lung nodules. A combination of preoperative localization and VATS makes the procedure more efficient in terms of wedge resection, diagnostic accuracy, reduction of blood loss, and a lower conversion rate to thoracotomy. 8 A randomized controlled trial that compared preoperative localization with no localization in lung nodules showed that the localization groups had a higher rate of successful VATS wedge resection (93.1% versus 48.1%, P < .01), decreased operative time (37 minutes versus 100 minutes, P < .01), and reduced stapler firings (3.7 versus 5.9, P < .01). Even if the wedge resection was not successfully performed after preoperative localization, the lesion could be easily found in the pulmonary lobe or segment based on the localized mark. 8
At present, several preoperative localization methods have been developed.6–9 The coil implantation method is more complex than use of methylene blue, radio-label, or hookwire implantation because the end tail of the coil should remain above the visceral pleura. However, methylene blue may diffuse rapidly. 6 Radio-label localization requires intraoperative fluoroscopic guidance that can lead to radiation damage. 9 Hookwire is usually limited by a high incidence of wire dislodgement that can cause pneumothorax, lung parenchymal hemorrhage, pleurogenic pain, and air embolization. 6
Gill et al. 10 developed an image-guided VATS strategy for lung nodules in which a C-arm CT scan is used to guide percutaneous marking with two T-bars followed by VATS resection of the lesion. These authors reported technical success rates for T-bar localization and wedge resection of 87.0% and 100.0%, respectively. However, C-arm CT requires real-time monitoring and exposes patients to more radiation.
At present, coil localization has been widely used for wedge resection of lung nodules.6–8 Previous studies have described two methods of coil localization: (1) the leaving-coil-end tail implantation method; (2) the entire coil implantation.6–8 The wedge resection can be performed directly using the leaving-coil-end tail implantation method. If the entire coil implantation method is used, the wedge resection can be performed based on intraoperative palpation of the coil.6–8 In this study, the coil localization was considered technically successful if the end tail of the coil was visible during the VATS procedure. Coil localization was technically unsuccessful in 7 cases, but wedge resection could be performed successfully in 5 of these cases because the coil was palpated during the VATS procedure. However, intraoperative palpation increased the complexity of the surgery.
The main value of coil localization for VATS lies in the ability to identify GGO nodules. 7 These nodules usually cannot be palpated during the VATS procedure because of their soft nature. In our study, there were 25 GGO nodules. The technical success rates for coil localization and wedge resection were 92.0% and 92.0%, respectively. These rates are comparable with those in the previous study of coil localization for GGO nodules. 7
The incidence rate of pneumothorax after coil implantation was 9% in this study. This rate is comparable with that in the previous studies of coil localization of lung nodules,6–8 but lower than the previously reported rates of 29.3%–37.9% for hookwire localization of lung nodules.11,17
Nine patients in our study had multiple target lung nodules and 7 had the known tumor and synchronous lung nodule. All of these patients underwent single-stage surgery, which was made easier by coil localization of the nodule.
The positive pathologic result rate of 64.2% (43/67) in this study is lower than the previously reported rates (76.2%–97.0%) for resection of lung nodules. Further, there was no significant difference in the positive pathological result rate according to nodule size in this study. These findings may be attributed to the limited sample size.
This study has some limitations. First, this is a retrospective review and therefore the selection bias inherently associated with such studies does exist. Second, the limited sample size and single-center research make it difficult to make definitive conclusions regarding this technique. Third, there was no control group in this study. Therefore, we have no means of comparing this approach to other preoperative localization techniques for lung nodules. Further prospective, controlled trials should be performed.
In conclusion, although further clinical trials are needed, our study indicates that preoperative CT-guided coil localization is a safe and effective method to facilitate a high successful rate of VATS wedge-resection for lung nodules. Use of this localization method can effectively avoid the anatomic resection for the diagnosis of lung nodules.
Footnotes
Disclosure Statement
No competing financial interests exist.