
Abstract
Abstract
Introduction:
Dismembered pyeloplasty remains the gold standard for the treatment of pelviureteric junction obstruction (PUJO). Robotic approach to this procedure has proven its efficacy and is gaining popularity. The introduction of barbed sutures such as “V-Loc™” (Covidien) has provided an addition to the sutures available for pyeloplasty. This work provides our experience with the V-Loc suture for closure of pelvis in children for robotic pyeloplasty (RP).
Materials and Methods:
A review of 10 pediatric RP (da Vinci Robotic System) during which the V-Loc suture was used was performed. Comparison was made with 15 cases in which 5-0 Vicryl® suture was used as an alternative. Overall median age was 4 (range 9 months to 16 years), M:F = 14:9. All had confirmed PUJO on renal ultrasound and mercaptoacetyltriglycine (mertiatide) (MAG-3). RP was done in the standard Anderson–Hynes manner with the placement of a multilength JJ ureteral stent intraoperatively. Patients had removal of the JJ stent 6 weeks postoperatively followed by renal ultrasound 3–4 months later.
Results:
Twenty-five RPs have been performed between May 2013 and November 2015, of which 10 have had closure of the pelvis performed using the V-Loc suture and 15 with Vicryl. One patient (6.67%) in the Vicryl group underwent redo-pyeloplasty secondary to a stent-related complication. The entire V-Loc group made an eventful initial recovery; however, four (40%) developed worsening hydronephrosis and drainage on ultrasound and MAG-3 after stent removal, despite remaining completely asymptomatic. These four required either restenting and observation (n = 1) or redo-pyeloplasty (n = 3). Histology demonstrated a “plaque-like” inflammatory reaction at the pelvic suture line.
Conclusion:
Closure of the pelvis using V-Loc suture material during RP can lead to a significant hydronephrosis requiring further procedures, including redo-pyeloplasty. These children can be asymptomatic and so extra vigilance on postoperative follow-up is essential.
Introduction
D
Advances in surgical technology also encompass changes to suture material, including the introduction of the unidirectional barbed suture material, such as V-Loc™ (Covidien). During minimally invasive surgery, intracorporeal knot-tying is known to be one of the most time-consuming steps and skills to acquire and perform with many learning curve studies focusing on the time required to complete such tasks. 3
The knotless properties of V-Loc and similar products, through which there is an end loop built into the suture through which the rest of the suture is passed, negate the need for a traditional knot to be tied and thus reduced operative time. Results comparing nonbarbed versus barbed suture to obtain closure of the renal pelvis during RP have recently been published in the adult population. 4 Both suture types obtained 90.1% patients demonstrating no obstruction postoperatively. Success was reported in 100% in the nonbarbed group and in the barbed group this figure was 92%.
This study provides our experience with V-Loc renal pelvis closure in pediatric RP over an 18-month period.
Materials and Methods
A prospective, nonrandomized review of 25 RPs, performed by a single surgeon, was performed between May 2013 and November 2015. Mean age at the time of operation was 4.2 years (9 months to 16 years) with Vicryl® mean age being 5.0 (±3.7, range 11 months to 16 years) and V-Loc 3.5 (±3.0, range 9 months to 8 years). The male to female ratio was 1.6:1.0. All children had confirmed hydronephrosis on USS and obstruction on mercaptoacetyltriglycine (mertiatide) (MAG-3) isotope renogram before surgery.
Patients were positioned in a supine position with elevation under the affected loin to provide optimum working space and access to the renal pelvis. The procedure was achieved using a transabdominal approach in all, none was performed transmesenterically. A three-port technique was used with an additional accessory port if necessary for assistance with retraction and gain exposure particularly if there is difficulty keeping bowel out of the way or excess intra-abdominal fat. A standard dismembered pyeloplasty was performed using the da Vinci Robotic System. The pelviureteric anastomosis was performed in all cases using a 5′0 Vicryl. Closure of the pelvis was achieved using 5′0 Vicryl or V-Loc; these were not consecutive cases and reflect the surgeons change in practice from Vicryl to V-Loc.
Placement of a multilength JJ ureteral stent and urethral urinary catheter was performed intraoperatively. The urethral catheter was removed typically on the first day postoperatively followed by a plain X-ray to confirm stent position before discharge. JJ stents were removed at 6 weeks postoperatively followed by ultrasound 3–4 months later. Clinical follow-up was maintained up to 21–52 months postoperatively.
Outcomes measured included operative time, time to discharge, symptomatic relief (if appropriate as per preoperative status), radiological resolution of obstruction, and reoperation if needed. All details were recorded on a Microsoft Excel spreadsheet® and statistical analysis performed using Instat™ software version 3. Statistical comparison of operative time and length of hospital stay (LOS) used unpaired t-test with Welch correction.
Results
Of the 25 RPs performed (left 11 versus right 14), 10 cases had closure of the pelvis performed using the V-Loc suture and 15 with Vicryl. In the Vicryl group, the mean operative time was 191.3 ± 48.2 minutes (range = 116–287) and in the V-Loc group, mean operative time was 106.0 ± 12.2 minutes (range = 88–120). Statistically, there was an extremely significant difference in the mean operative time P < .0001.
It could be argued that the difference in operative time may be related to the surgeon's learning curve, however, Figure 1 demonstrates the operative time for all cases and suture types plotted against the month and year. It can be seen that a standard learning curve exists over 18 months. However, when comparing V-Loc and Vicryl cases performed around the same point of the curve in this study, the V-Loc cases are faster.

Learning curve for RP with suture subtypes included. The initial experience of RP was using 5-0 Vicryl®. As expected, the learning curve follows the generally accepted pattern with operative time reducing with number of cases. Nonetheless, once both Vicryl and V-Loc are utilized during the same period, it is clear that operative time appears to be lower in the V-Loc group. There was no significant difference in mean age between the two groups. RP, robotic pyeloplasty.
There was no significant difference in the LOS, with both suture groups being discharged in a median of 2 days: Vicryl group range 1–4 days and V-Loc range 1–3 days.
One patient (6.7%) in the Vicryl group underwent redo-pyeloplasty secondary to a stent-related complication. The proximal end of the stent had caught up inadvertently in the suture line causing a leak. The entire V-Loc group made an eventful initial recovery; however, four (40.0%) developed worsening hydronephrosis on ultrasound after stent removal, despite remaining clinically asymptomatic. Subsequent MAG-3 scanning of these four patients confirmed poor drainage in association with hydronephrosis. All four cases required redo-pyeloplasty. Histology demonstrated a “plaque-like” inflammatory reaction at the pelvic suture line (Figs. 2 and 3).
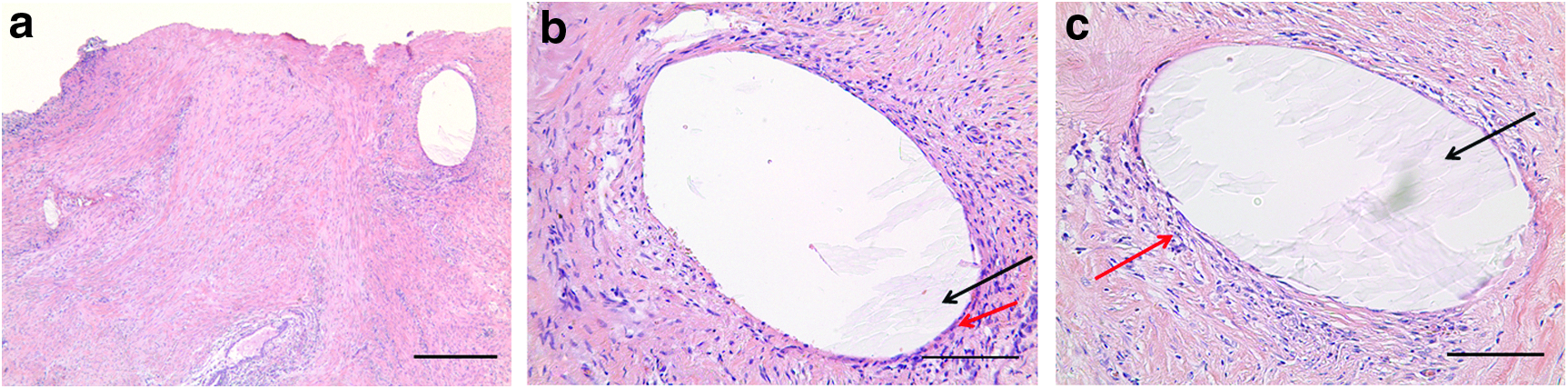
Histology taken from first V-Loc™ patient at the time of redo-pyeloplasty. The red arrow is used to highlight the fibroblastic, chronic “plaque like” inflammatory reaction at the renal pelvis suture margin as demonstrated by hematoxylin and eosin staining at both × 10
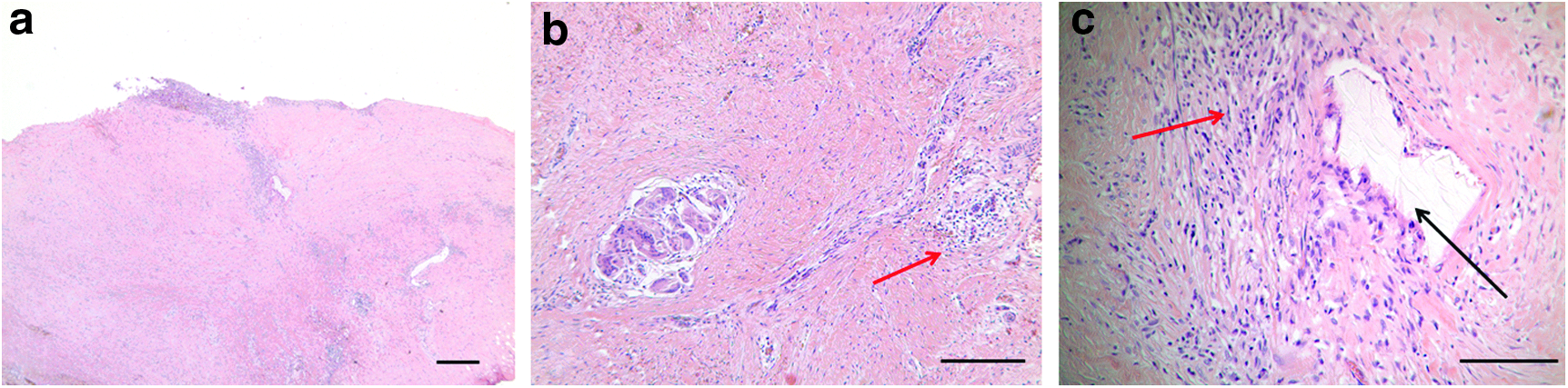
Histology taken from second V-Loc patient at the time of redo-pyeloplasty. The red arrow is used to highlight the fibroblastic, chronic “plaque like” inflammatory reaction at the renal pelvis suture margin as demonstrated by hematoxylin and eosin staining at both × 2
Discussion
Barbed sutures such as V-Loc provide an alternative method to obtain a watertight closure of the renal pelvis. A small series of three patients had been described in the literature 5 with positive preliminary results. However, the data reported here are larger and raise concerns regarding severe, localized inflammatory reaction along the suture line and eventual stenosis in 40.0% of cases, only identified during routine USS at 4.5–6 months postoperatively.
Kaushik in 2012 assessed the physical properties (tensile strength and peak sliding force) of robotically “manipulated” sutures, including V-Loc. The mean difference in breaking forces for manipulated versus nonmanipulated V-Loc sutures was 1.30 N (P = .046) and a lower peak sliding force compared with the nonmanipulated group (0.76 N versus 0.88 N, P = .199). Electron microscopy demonstrated that this loss in performance was related to structural damage to the suture and barbs but not thought to be clinically significant. However, the microfractures within the material may make it more likely to create an abnormal surface for the body to react to.
Communication between our group and the manufacturers suggests that the 4-0 V-Loc suture is equivalent to a 3-0 standard monofilament suture, when the full dimension, including the barb, is taken into account. Given the increased relative suture size creating larger holes permitting microscopic urine leakage around the anastomosis, increased inflammation to surrounding tissues is likely to occur. Despite the absence of clinical symptoms, this potentially small amount of urine leakage is pathologically significant as it creates inflammation around the suture line. Personal communication with some colleagues in the adult urology practice revealed that similar episodes were encountered in their practice although this is unverified and not published in literature.
V-Loc sutures have been used for hepaticojejunostomies in pediatric hepatobiliary surgery, with stenosis and obstruction at the anastomotic site being reported. 6 Data of V-Loc use in adult laparoscopic ventral rectopexies demonstrated the incidence of small bowel obstruction to be significantly higher. 7 Of note, the risk of bowel obstruction from the V-Loc in the aforementioned work was not reduced by burying or cutting the suture flush, technical advice given to reduce obstruction.
Our experience of using a barbed, knotless suture for closure of the renal pelvis in RP is the largest in the literature. Despite being clinically asymptomatic, 40% children developed an evolving problem. All four redo-pyeloplasties, which had V-Loc utilized in the initial operation, have had a successful second procedure using Vicryl. The authors no longer utilize V-Loc for any aspect of RP in any pediatric case, irrespective of age. V-Loc suture material can lead to redo-pyeloplasty and despite offering the advantage of shorter operative times, may offer just a “barbed shortcut.”
Footnotes
Disclosure Statement
No competing financial interests exist.