
Abstract
Abstract
Introduction:
Patients with moderate (grade II) acute cholecystitis patients, as defined by the 2013 Tokyo Guidelines, were retrospectively compared with respect to emergency cholecystectomy (EC) and delayed cholecystectomy (DC) after percutaneous transhepatic gallbladder drainage (PTGBD) to determine the better treatment strategy.
Methods:
Forty-nine of 103 patients with PTGBD and 47 of 54 patients with EC were assessed for eligibility from January 2013 to January 2017. Patients with the following conditions were included: (i) moderate (grade II) acute cholecystitis diagnosed by the 2013 Tokyo Guidelines; (ii) no common bile duct stones; (iii) no atrophic cholecystitis; (iv) no decompensated liver cirrhosis and massive ascites; (v) no diffuse peritonitis; (vi) surgeons are professors or associate professors; and (vii) PTGBD is not the only procedure for the patient defined by clinicians. The preoperative characteristics and postoperative outcomes were analyzed. PTGBD was performed by experienced interventional radiologists and cholecystectomy was performed by professors or associate professors.
Results:
Patients in the EC and PTGBD + DC groups had similar demographic, clinical, preoperative laboratory, and imaging characteristics. Both PTGBD and EC resolved the cholecystitis quickly. Compared to the PTGBD + DC group, EC patients had more intraoperative bleeding (101 ± 125 mL versus 33 ± 37 mL, P = .003), longer duration of postoperative abdominal drainage (9.0 ± 12.9 days versus 3.4 ± 2.1 days, P = .041), more patients converted to open cholecystectomy (OC; 19.1% versus 4.1%, P = .021), more OC patients (14.9% versus 0%, P = .005), more patients with gangrenous cholecystitis (40.4% versus 8.2%, P < .001), more cholecystitis patients with perforation (12.8% versus 0%, P = .012), a higher incidence of respiratory failure (14.8% versus 2.0%, P = .029), more admissions to the intensive care unit (ICU) (21.3% versus 2.0%, P = .003), and longer postoperative hospital stays (8.2 ± 3.2 days versus 11.6 ± 4.6 days, P < .001) in the PTGBD + DC group. In addition, there were statistically more OC patients (63.2% versus 14.3%, P = .001) in the nonbiliary surgeon group than the biliary surgeon group.
Conclusion(s):
In patients with moderate (grade II) acute cholecystitis, PTGBD and EC were highly efficient in resolving cholecystitis. DC patients after PTGBD had better outcomes with a lower rate of OC, less intraoperative bleeding, shorter duration of postoperative abdominal drainage, shorter hospital stays after cholecystectomy, a lower incidence of respiratory failure, fewer admissions to the ICU than EC, and reversed the pathologic process affecting the gallbladder. The total postoperative hospital stay was longer in the PTGBD + DC group.
Introduction
C
PTGBD can relieve inflammation and peri-cholecystic adhesions, and lead to complications related to the procedure. Controversy has arisen based on a detailed comparison between emergency cholecystectomy (EC) and delayed cholecystectomy (DC) after PTGBD in patients with moderate acute cholecystitis. The present research retrospectively compared the efficacy of EC with DC after PTGBD under strict inclusion criteria.
Patients and Methods
Inclusion criteria
(1) Moderate (grade II) acute cholecystitis with severe inflammation diagnosed according to the 2013 Tokyo Guidelines, 1 associated with any one of the following conditions:
(i) elevated white blood cell count (>18,000/mm);
(ii) palpable tender mass in the right upper abdominal quadrant;
(iii) duration of complaints >72 hours;
(iv) marked local inflammation (gangrenous cholecystitis, peri-cholecystic abscess, hepatic abscess, biliary peritonitis, and emphysematous cholecystitis); and
(v) diagnostic standard of gangrenous cholecystitis (irregular thickening of the gallbladder wall or imaging of the ruptured gallbladder wall or the presence of peri-cholecystic fluid, excluding pancreatitis, duodenitis, and perforated peptic ulcer.1,3
(2) Others:
(i) no common bile duct stones;
(ii) no atrophic cholecystitis;
(iii) no decompensated liver cirrhosis and massive ascites;
(iv) no diffuse peritonitis;
(v) surgeons are professors or associate professors; and
(vi) PTGBD is not the only procedure for the patient defined by clinicians (there is a contraindication for surgery or anesthesia; cholecystectomy cannot improve the patient survival time and quality of life).
The study was conducted at Shengjing Hospital Affiliated to China Medical University (Liaoning, China). From January 2013 to January 2017, we reviewed the medical records of 103 patients who underwent PTGBD, and selected 49 patients with moderate acute cholecystitis who underwent DC after PTGBD under the inclusion criteria (Fig. 1). The interval of time from PTGBD to DC was 1–1096 days, with an average of 92 days. During the same period, we reviewed the medical records of 54 patients diagnosed with moderate acute cholecystitis who underwent EC and selected 47 patients who were eligible based on the inclusion criteria (Fig. 2). The EC and PTGBD + DC groups were compared based on the following: demographic data; preoperative clinical characteristics; preoperative laboratory results; and imaging findings.
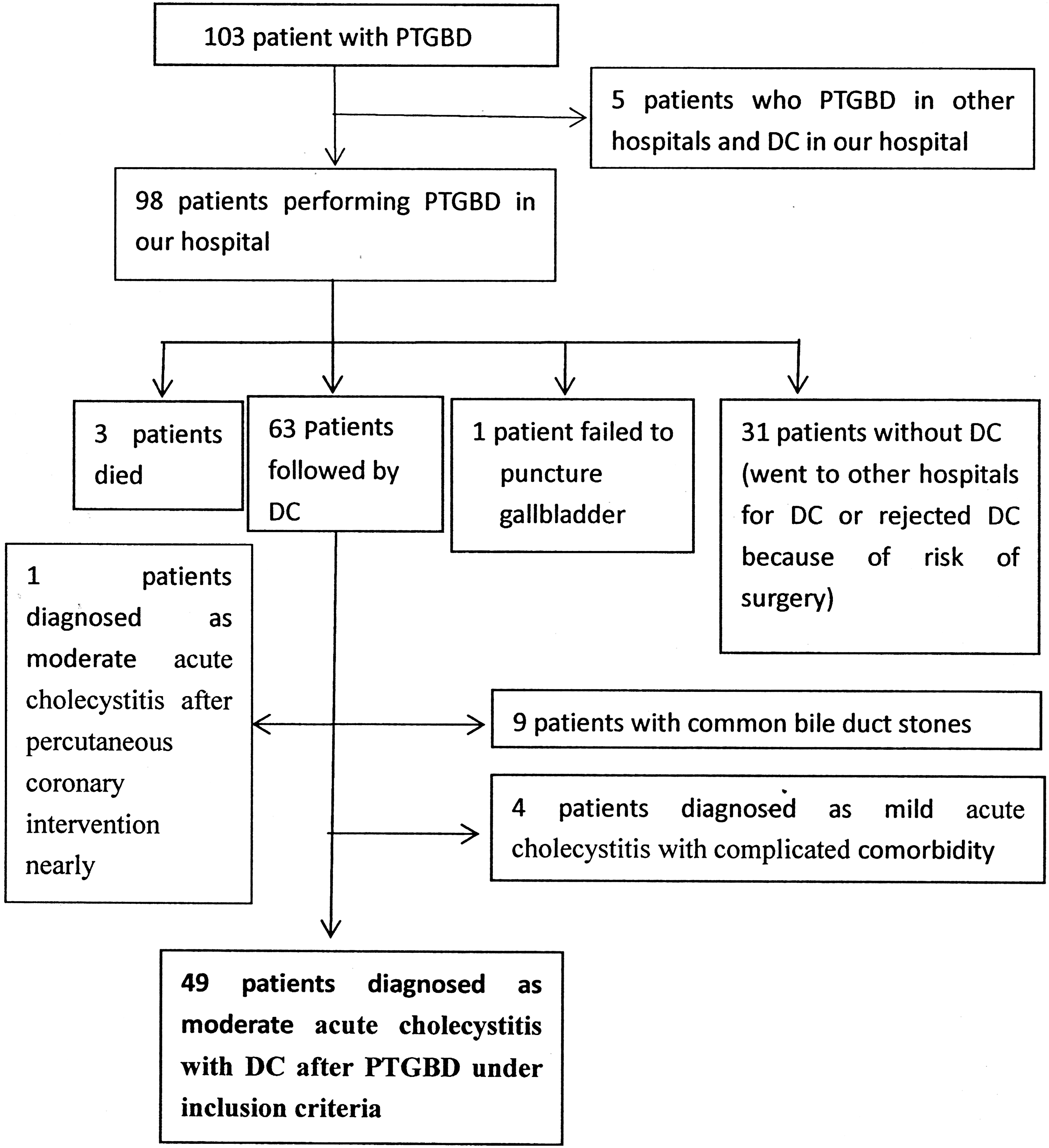
Patients in PTGBD + DC. We searched 103 patients who underwent PTGBD, and selected 49 patients performing DC after PTGBD in moderate acute cholecystitis under inclusion criteria. DC, delayed cholecystectomy; PTGBD, percutaneous transhepatic gallbladder drainage.
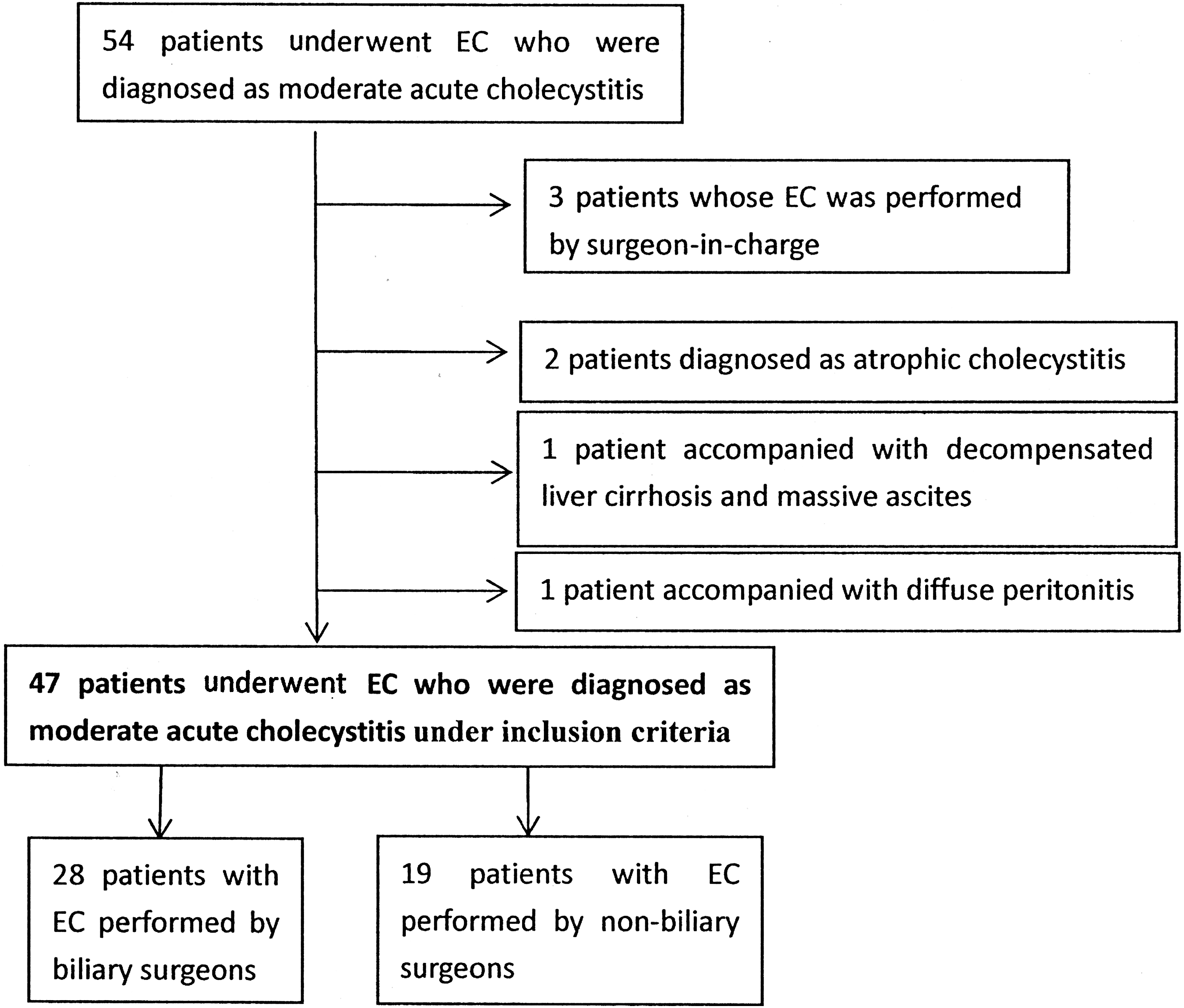
Patients in EC. We searched 54 patients found to have moderate acute cholecystitis who underwent EC and selected 47 patients under inclusion criteria. EC, emergency cholecystectomy.
Percutaneous transhepatic gallbladder drainage
The PTGBD procedure was performed under local anesthesia (5 mL of 5% lidocaine) using ultrasound-guided drainage by experienced interventional radiologists. A puncture needle was advanced transhepatically into the upper one-third of the gallbladder. The aspirated material was sent for bacterial culture. Guidewire placement within the gallbladder was confirmed with fluoroscopy. After placing a guidewire and dilating the track, an 8-Fr pigtail catheter was inserted to form a loop in the gallbladder, which was connected to an external drainage bag. The bag was sutured and fixed to the skin, thus providing continuous external drainage.
Cholecystectomy
Operations were performed by professors or associate professors. One patient in the EC group underwent an open cholecystectomy (OC) because previous upper abdominal open surgery indicated increased anesthetic risk (American Society of Anesthesiologists [ASA] III or IV), and marked local inflammation. For six patients in the EC group a decision was made by the surgeons for these patients to immediately undergo OC to shorten the operative time and avoid operative complications. Experienced anesthetists determined there was an increased anesthetic risk, as well as marked local inflammation as established by ultrasound or computer tomography (CT), including a significantly enlarged gallbladder, pericholecystic or peri-hepatic fluid, and thickening of pericholecystic gastric or colonic wall. Other patients underwent laparoscopic cholecystectomy (LC) using a three- or four-port technique, and the decision to convert to OC was based on the operative findings, including difficulty of dissection, poor control of intraoperative hemorrhage, and severe adhesions involving Calot's triangle or the liver bed.
Statistical analysis of the data
Data were entered into a computer and analyzed using IBM SPSS software (version 19.0; Armonk, NY). Comparisons between groups for categorical variables were assessed using the chi-square test and Fisher's exact test. The Student's t-test was used to compare two groups for quantitative variables. The significance of the results was set at the 5% level.
Results
Patients in the EC and PTGBD + DC groups had similar demographic, clinical, preoperative laboratory tests, and imaging characteristics (Table 1). There was no statistical difference between the two groups with respect to the following: age, including patients >80 years of age; gender; temperature; white blood cell (WBC) count; neutrophil (NE)%, alanine aminotransferase, aspartate aminotransferase (AST), direct bilirubin, and indirect bilirubin level; prothrombin time; international normalized ratio; duration from onset of symptoms to surgical treatment; systemic inflammatory response syndrome; use of analgesics; cardiovascular disease; diabetes mellitus; cerebrovascular disease; respiratory disease; renal insufficiency; previous upper abdominal open surgery; Murphy's sign; and ASA class. Preintervention imaging findings, including thickness of the gallbladder wall; calculus incarcerated in the neck of the gallbladder; and local inflammation, such as peri-cholecystic exudation and peri-cholecystic or -hepatic fluid; thickening of the peri-cholecystic gastric or colonic wall; gallbladder bilateral sign; peri-cholecystic or hepatic abscess; and localized peritonitis.
Thickness of gallbladder wall was defined by ultrasound; local inflammation was defined by ultrasound or computed tomography.
Qualitative data were expressed using number and percent and were compared using the chi-square test or Fisher test. Quantitative data were expressed in mean ± standard deviation and was compared using the Student t test.
ALT, alanine aminotransferase; ASA, American Society of Anesthesiologists; AST, aspartate aminotransferase; DC, delayed cholecystectomy; EC, emergency cholecystectomy; INR, international normalized ratio; NE, neutrophil; PTGBD, percutaneous transhepatic gallbladder drainage; SIRS, systemic inflammatory response syndrome; WBC, white blood cell.
Forty-eight of 49 patients in the PTGBD + DC group improved after PTGBD, while one patient had continuous abdominal pain and jaundice and underwent LC. There were 28 patients in the PTGBD + LC group with the following bacterial culture results: (i) no bacterial growth (15 [53.6%]); (ii) Escherichia coli (3 [10.7%]); (iii) Klebsiella pneumoniae (3 [10.7%]); (iv) Staphylococcus aureus (2 [7.1%]); (v) Enterococcus faecalis (2 [7.1%]); (vi) Enterococcus faecium (1 [3.6%]); (vii) Citrobacter fungi (1 [3.6%]); and (viii) Enterobacter cloacae (1 [3.6%]). The top three bile traits of the PTGBD + DC group were as follows: (i) dark green bile (22 [44.9%]); (ii) white, yellow, or brown pus (13 [26.5%]); and (iii) yellow turbid bile (6 [12.2%]).
Efficacy of EC versus PTGBD
There were no statistical differences in temperature, WBC count, NE%, and AST, direct bilirubin, and indirect bilirubin levels 72 hours after EC or PTGBD in the two groups (Table 2).
Comparison of operative and postoperative data in the two groups
There were no significant differences in operative time, postoperative time to pass gas via the anus, postoperative use of analgesics, subtotal cholecystectomy, and total cost. A comparison of EC and DC revealed statistically more intraoperative bleeding (101 ± 125 versus 33 ± 37 mL, P = .003), postoperative abdominal drainage time (9.0 ± 12.9 versus 3.4 ± 2.1 days, P = .041), LC conversion to OC (19.1% versus 4.1%, P = .021), OC (14.9% versus 0%, P = .005), gangrenous cholecystitis (40.4% versus 8.2%, P < .001), and cholecystitis with perforation (12.8% versus 0%, P = .012) in the EC group, and a longer total postoperative hospital stay (8.2 ± 3.2 versus 11.6 ± 4.6 days, P < .001) in the PTGBD + DC group (Table 3).
Total postoperative hospital stay was defined as hospital stay after PTGBD and hospital stay after cholecystectomy.
LC, laparoscopic cholecystectomy; OC, open cholecystectomy; total cost, cost of PTGBD, and cost of cholecystectomy.
Comparison of complications between the two groups
There were no significant differences in total complications, bile leakage after cholecystectomy, residual stones after cholecystectomy, pneumonia, septicemia, cardiovascular complications, worsening renal insufficiency, neurologic complications, transient fevers, surgical wound infections, ileus, urinary tract infections, and death in the two groups. A comparison of the EC and PTGBD + DC groups revealed a statistically higher incidence of respiratory failure (14.8% versus 2.0%, P = .029) and admission to the intensive care unit (ICU) (21.3% versus 2.0%, P = .003; Table 4).
Complications associated with drainage tube of PTGBD (12): Bile leakage: 1; Hepatapostema: 1; Common bile duct stone: 2; Recurrence of cholecystitis: 1; Blocked drainage tube: 3; Slipping off drainage tube: 2; Bleeding: 1; Pierced gallbladder: 1.
ICU, intensive care unit.
There were 12 patients with complications associated with the PTGBD tube. There was bile leakage in one patient, who had jaundice and fever after drainage. The gallbladder drainage fluid was 5–20 mL per day and peritonitis was defined by CT, and then LC was performed. One patient, whose tube had been placed for 5 months had hepatapostema, with some drainage after discharge from the hospital, and intermittent upper abdominal pain and fever. Hepatapostema was diagnosed after re-admission. LC was performed with incision and drainage of the hepatapostema. Two patients had common bile duct stones. The tube was retained for 3 months in one patient, who had intermittent upper abdominal pain, and the tube was retained for 12 months in the other, asymptomatic patient. Two patients who were diagnosed with common bile duct stones by cholangiography, underwent endoscopic retrograde cholangiopancreatography. One patient in whom the drainage was <10 mL, had recurrent cholecystitis 2 months after hospital discharge, and improved after conservative treatment. Three patients had blocked drainage tubes. The tubes were cleared by flushing with saline. Two patients had displacement of the drainage tubes; one occurred 3 months and the other occurred 4 months after PTGBD. In one patient in whom the drainage tube was retained for 3 years, the tube pierced the gallbladder (Table 4).
Comparison between nonbiliary and biliary surgeons in the EC group
There were no significant differences in operative time, intraoperative bleeding, duration of postoperative abdominal drainage, and subtotal cholecystectomies in the two groups. Comparing nonbiliary and biliary surgeons in the EC group revealed statistically more total OC in nonbiliary surgeons (63.2% versus 14.%, P = .001; Table 5).
Total OC is defined as open cholecystectomy and laparoscopic cholecystectomy conversion to open cholecystectomy.
Discussion
PTGBD was first proposed by Radder in 1980 for the treatment of gallbladder empyema, which solved the problem of gallbladder bile drainage by elimination of the obstructive symptoms, but problems associated with drainage and secondary admission increased. EC can quickly remove the primary lesion, while the perioperative injury occurs more frequently, especially in moderate cholecystitis. Because of the lack of prospective randomized controlled trials, the efficacy of PTGBD is controversial. On the basis of the 2013 Tokyo Guidelines, the present study strictly controlled the inclusion criteria and retrospectively compared EC with PTGBD, followed by elective cholecystectomy.
With the development and maturity of PTGBD technology, there were 98 patients who underwent PTGBD in our hospital. Gallbladder puncture failed in one patient because of the lack of clarity of the gallbladder on ultrasound; the rate of success was nearly 99%. In the 49 patients with PTGBD in our group, 23 had postoperative complications after PTGBD; 12 cases were associated with the drainage tube, and the incidence of complications associated with drainage tube was 25.5%, similar to the 26.3% reported by Pang et al., 4 and higher than the 6.24%–8.57% reported by Winbladh et al. 5 The possible reasons for this finding are as follows: (i) the occurrence of drainage-related complications for patients in this study were collected from PTGBD to re-admission for cholecystectomy, while a number of previous studies collected statistics involving complications only after PTGBD, which led to an underestimation of complications; (ii) some of the patients in our study retained the drainage tube longer (up to 3 years, with an average of 92 days), which led to an increase in the incidence of complications. In the remaining 11 cases, complications were associated with an underlying disease. Although there was no significant difference in the total complications between the EC and the PTGBD + DC group, PTGBD would lead to additional complications for the patients. The incidence of respiratory failure and admission to the ICU were statistically higher in the EC group, which verified that PTGBD reduces the incidence of severe complications after cholecystectomy in patients with moderate acute cholecystitis, especially patients with complicated underlying diseases. If symptoms and laboratory indicators of patients do not obviously increase or even worsen 3 days after PTGBD, the prognosis is poor.
There was no statistically significant difference in the efficacy between the EC and PTGBD groups, which confirmed that PTGBD effectively relieved obstruction and eliminated inflammation. One patient died of respiratory failure and postoperative cardiopulmonary dysfunction after EC. Three of 98 patients died after PTGBD. One patient admitted with coronary heart disease who had undergone percutaneous coronary intervention, died of ventricular fibrillation, septic shock, and multiple organ failure after PTGBD. One patient was diagnosed with acute ischemic intestinal obstruction and had secondary acalculous cholecystitis. PTGBD did not improve the critically ill status and the patient died of septic shock. The remaining patient had abdominal pain, chills, and fever 1 month after PTGBD, and was diagnosed with a liver abscess and septic shock. His advanced age and complicated underlying comorbidities contributed to his death. We concluded that the death after PTGBD was more closely related to the patient's comorbidities; however, he may have also died after EC. At the same time, attention should be paid to the death related to liver abscesses, while others have reported the mortality associated with PTGBD drainage was due to intestinal perforation and bile leakage. 5 No patients died after PTGBD followed by DC.
The postoperative drainage time, the length of hospital stay after cholecystectomy, the conversion to open surgery, and OC were statistically higher in the EC group, which is consistent with previous reports.5,6 It has been reported7,8 that PTGBD for acute cholecystitis increases the rate of open surgery, biliary complications, and the incidence of infection in DC. The difference may be because the candidates in this study had moderate acute cholecystitis only, which is associated with increased operative difficulty, while previous studies are less clear on the severity of cholecystitis, which could include patients with mild acute cholecystitis in the groups to reduce the difficulty of EC. Additionally, the reason for the difference could be that some patients are brought to our hospital from local hospitals, thus missing the optimal operative window of 72 hours. This in turn caused significant peri-cholecystic adhesions and a dense gallbladder triangle in EC. One case needed intraoperative cholangiography to verify the anatomic structure, and some cases were found with adhesive masses among the gallbladder, omentum, and intestinal wall, which caused difficulty during surgery. Surgeons made the decision of conversion to OC from LC when difficult separation of adhesions or uncontrollable bleeding was encountered. DC in patients after PTGBD had less local inflammation and the surgery was easier to perform.
Recently, it has been reported 9 that under the guidance of the 2013 Tokyo Guidelines, there was no statistical difference between the EC group with PTGBD followed by the DC group with respect to hospitalization time, operative time, rate of laparoscopic surgery, and postoperative complications for moderate acute cholecystitis. The authors also acknowledge that there were some incomplete records regarding diagnosis, treatment, and selection bias. In addition, the statistics pertinent to the preoperative, comorbidities and local inflammation were not detailed. At the same time, it was 9 concluded that the PTGBD + DC group had longer total postoperative hospital stays than the EC group (the total postoperative hospital stay was defined as the PTGBD postoperative hospital stay + DC postoperative hospital stay), which is consistent with the results of the present research.
Lo et al. 10 compared emergency LC with PTGBD + delayed LC in patients with acute cholecystitis and perforation and found that although the operative procedure of the former was more difficult, there was no statistical difference in the operative time, intraoperative bleeding, intra- and postoperative complications, and emergency LC significantly reduced the average length of hospital stay. Nevertheless, Lo et al. 10 still recommended patients >70 years of age with a duration of symptoms >4 days should have PTGBD followed by DC.
A prospective randomized controlled trial by El-Gendi et al. 11 demonstrated that PTGBD followed by cholecystectomy was more effective than EC for patients with moderate acute cholecystitis when the duration of symptoms was >72 hours in the 2013 Tokyo Guidelines. There was a statistical decrease in conversion to open surgery, operative complications, and hospital stay after cholecystectomy in the PTGBD + DC group, which was partly consistent with our study. El-Gendi et al. 11 excluded patients with ASA grade IV and severe local inflammation of the gallbladder, such as gangrenous cholecystitis, gallbladder abscess, biliary peritonitis, liver abscess, and emphysematous cholecystitis, which could lead to more blood loss, more postoperative abdominal drainage time, more patients with OC, a higher rate of respiratory failure, and the rate of admission to the ICU in our EC group.
In addition, we compared surgery performed by nonbiliary and biliary surgeons in the EC group, and concluded that the rate of total open surgery (OC and conversion to OC) is statistically higher among nonbiliary surgeons, while the operative time, surgical blood loss, postoperative abdominal drainage time, and subtotal cholecystectomy were not statistically different, indicating that with technical improvement of the surgeon, LC could be more widespread.
The average interval between PTGBD and cholecystectomy in 49 patients was 92 days in the current study. The average interval between PTGBD and cholecystectomy in 49 patients was 92 days in the current study, when performing a cholecystectomy following PTGBD is controversial. Han et al. 12 pointed out that for moderate acute cholecystitis, an interval <72 hours has a higher incidence of complications, longer operative time, and shorter hospital stay. Jung and Park 13 reported that for mild or moderate acute cholecystitis, the longer the tube was retained, the more tube-related complications occurred after PTGBD. Therefore, it was recommended that LC should be performed <10 days after PTGBD. Inoue et al. 14 reported that the cholecystectomy was more difficult <216 hours after PTGBD. Kim et al. 6 concluded that an interval of 2–7 weeks from PTGBD to LC reduces the conversion rate and the incidence of complications for moderate acute cholecystitis. It is our belief that the related research should take full account of the local inflammation of the gallbladder because many surgeons would perform PTGBD for patients with mild acute cholecystitis due to complicated comorbidities and to avoid the risk of surgery. The timing of DC corresponding to different local inflammation should be different. In addition, we found that separation of the gallbladder triangle is more difficult when it was drained for 2–3 months in moderate acute cholecystitis with calculus incarcerated in the neck or cystic duct of the gallbladder because the stone would compress the gallbladder triangle for a long time, causing dense fibrous adhesions and increasing the difficulty of surgery. The interval between LC after PTGBD warrants further study.
There were 19 cases of gangrenous cholecystitis and 6 cases of cholecystitis with perforation in the EC group, which was significantly more than the PTGBD + DC group. There were four cases of gangrenous cholecystitis and no perforation (the drainage time of the four cases with gangrenous cholecystitis were 3, 6, 8, and 40 days, with an average of 14 days) in the PTGBD + DC group. In addition, comparing the demographic data, preoperative clinical characteristics, preoperative laboratory testing, and imaging characteristics revealed no statistical differences. We concluded that gangrenous cholecystitis can progress to chronic cholecystitis, similar to cholecystitis with perforation after full drainage of the PTGBD, which helped to confirm the optimal timing of cholecystectomy after PTGBD.
Conclusion
In conclusion, PTGBD followed by DC for moderate acute cholecystitis is completely feasible and effective, especially for patients with comorbidities performed by nonbiliary surgeons which can effectively reduce the incidence of postoperative severe complications, operative difficulty, and reverse the pathologic process of the gallbladder. At the same time, complications related to gallbladder drainage should not be ignored, especially in patients retaining the tube for a long time. We should also explore the appropriate timing of DC after PTGBD with attention to the differing severity of local inflammation to determine the optimal individual treatment.
Footnotes
Disclosure Statement
No competing financial interests exist.