
Abstract
Abstract
Background:
Prior studies report safety and effectiveness of laparoscopic colectomy in older patients. The study aimed to examine the impact of laparoscopic colectomy on 30-day readmissions, discharge destination, hospital length of stay, and cost in younger (19–65 years) and older adults (>65 years).
Materials and Methods:
We used the nationwide readmission database from 2013 to study adults undergoing elective colectomy. The outcomes were 30-day readmissions, discharge destination for the index hospitalization (routine, skilled nursing facility [SNF]/intermediate care facility [ICF], home healthcare), length of stay, and cost. Multivariable analyses were conducted to determine the association of laparoscopic colectomy on outcome; logistic regression for 30-day readmission, multinomial logistic regression for discharge destination, and linear regression for length of stay and cost. An interaction between age and colectomy approach was included, and all models controlled gender, income, insurance status, All Patients Refined Diagnosis Related Groups (APR-DRG), Elixhauser comorbidities, hospital bed size, ownership, and teaching status.
Results:
Of 79,581 colectomies, 40.2% were laparoscopic. Laparoscopic colectomy was more frequent in younger patients (41.9% versus 38.5%, p < .0001). Regardless of age, patients undergoing laparoscopic colectomy were 20% less likely to be readmitted within 30 days (odds ratio [OR] 0.80, confidence interval [95% CI] 0.75–0.85). For postdischarge destination, laparoscopic colectomy offered higher benefits to younger patients (SNF/ICF: OR 0.42, 95% CI 0.36–0.49; home health: OR 0.32, 95% CI 0.30–0.35) than older patients (SNF/ICF: OR 0.50, 95% CI 0.47–0.54; home health: OR 0.59, 95% CI 0.55–0.62). Regardless of age, laparoscopic colectomy resulted in 1.46 days (p < .0001) shorter hospital stays compared to open colectomy. Laparoscopic colectomy had significantly lower cost compared to open approach, particularly in younger ($1,466) versus older ($632) patients.
Conclusions:
Laparoscopic colectomy is superior to an open approach, with fewer 30-day readmissions, fewer discharges to SNF/ICF or home health, shorter hospital stays, and less overall cost; younger patients benefit more than older patients.
Introduction
L
With colon and rectal cancer being the third most common cancer in the United States and with an increasing incidence, the benefits of laparoscopic approaches to colorectal resection in adults of all ages are of great interest.6,7 In contrast to the decreasing incidence of colon and rectal cancer in Americans older than 55 years, since 1990 the incidence of colon cancer has increased nearly 50%, and the incidence of rectal cancer has doubled, in the younger adult population. 8
Research supporting the clinical benefits of colon resections performed laparoscopically has spurred its continuously increasing preference by surgeons over a traditional open colectomy approach.9,10 A systematic review of laparoscopic versus open colorectal resection demonstrated the safety and benefits of the laparoscopic approach in the elderly.11,12 Laparoscopic colectomy also resulted in lower healthcare costs and utilization in younger patients insured through private insurance. 13 However, laparoscopic colectomy has been reported to improve short-term postoperative outcomes more in elderly (70 years or older) than in younger patients (younger than 70 years). 12
Despite the increasing incidence of colorectal cancer in the younger population, little information is available about the clinical or economic benefit of performing colectomies using a laparoscopic approach in younger patients. Moreover, the advantage of laparoscopic colectomy in younger patients relative to older patients is not described. Therefore, the aim of this study was to examine the influence of colectomy approach on 30-day readmission, discharge destination, hospital length of stay, and cost in younger (19–65 years) and older adults (>65 years).
Materials and Methods
Data source and study design
This retrospective cohort study used the 2013 Nationwide Readmissions Database (NRD). The NRD is created from the State Inpatient Databases (SIDs) that contain reliable verified patient linkage numbers that can be used to track patients across hospitals within a state. The 2013 NRD is constructed from 21 SIDs. The NRD includes hospitalizations in the community, specialty and federal hospitals from 21 states, and accounts for 49.3% of the U.S. population and 49.1% of the U.S. hospitalizations reported in the American Hospital Association (AHA) Annual Survey Database. Unweighted, the NRD contains data from ∼14 million discharges each year. Weighted, it estimates roughly 36 million discharges in the United States. For this study, we used four files from the NRD: core file, severity file, hospital file, and cost-to-charge ratio file. The core file contains data elements about the index admission, clinical information, patient demographics, and readmission. The severity file contains the Agency for Healthcare Research and Quality Elixhauser comorbidity measures and All Patients Refined Diagnosis Related Groups (APR-DRG). The hospital file contains variables related to hospital characteristics. Because the NRD reports hospital charges, we used the cost-to-charge ratio file to convert hospital charges to cost.
Study cohort
The cohort included adult patients (age ≥18 years) who underwent elective colectomy (left hemicolectomy, right hemicolectomy, or sigmoidectomy). Patients were excluded if (1) they died during the index hospitalization (not at risk for readmission), (2) left against medical advice, (3) were transferred to other acute care hospital, (4) had missing length of stay, or (5) were discharged in December, as we could not calculate 30-day readmission for this group.
Exposure
The primary exposure was laparoscopic (International Classification of Disease, ninth revision, [ICD-9] procedure codes: 1733, 1735, and 1736) versus open (ICD-9 procedure codes: 4573, 4575, and 4576) colectomy.
Outcome
Four outcomes were considered in this study: (1) 30-day readmission (yes versus no), (2) discharge destination (home, SNF/intermediate care facility [ICF], home healthcare), (3) length of stay, and (4) cost.
Covariates
We included patient and hospital characteristics as covariates. Patient characteristics were age (18–64 years, 65–90 years), gender (male, female), median household income (quartiles: $1–$37,999, $38,000–$47,999, $48,000–$63,999, ≥$64,000), payer type (Medicare, Medicaid, private insurance, self-pay, no charge/other), Elixhauser comorbidity score, APR-DRG, and discharge diagnosis. We derived the summary Elixhauser comorbidity index using weights derived by wan Walraven et al. 14 APR-DRG were classified as minor, moderate, major, and extreme loss of function. Based on the primary discharge diagnosis, we classified each patient's diagnosis as cancer, diverticulitis, or other. Hospital characteristics were hospital volume of colectomy (classified in quartiles), ownership (government, nonfederal; private, not-for-profit; private, investor owned), bed size (small, medium, high), and teaching status (metropolitan nonteaching, metropolitan teaching, nonmetropolitan). Bed size categories are based on hospital beds and are specific to the hospital's location and teaching status. 15
Statistical analyses
Baseline characteristics of the study cohort were described using descriptive statistics (mean with standard deviation or proportions). Baseline characteristics between laparoscopic and open colectomy were compared using chi-square for categorical and t-test analyses for continuous variables. Descriptive statistics was used to report outcome rates across age groups for the laparoscopic and open colectomy approach.
To determine the adjusted association of laparoscopic colectomy on outcome, a multivariable model was chosen based on the outcome: logistic regression for 30-day readmission; multinomial logistic regression for discharge destination; and linear regression for length of stay and cost. In all multivariable models, the primary independent variables were colectomy approach (open versus laparoscopic) and age group (18–64 years versus 65–90 years); we performed an interaction of these variables to determine whether the benefits of laparoscopic colectomy on our four outcomes of interest differed by age group. All models controlled for the patient- and hospital-level covariates mentioned above. If the interaction was not significant, the variable was not included in the final model.
All analyses were adjusted for NRD survey design (cluster, strata, and weight) to allow for generalization of results at the national level. All statistical analyses were performed using SAS 9.4 (SAS Institute, Inc., NC). This study was considered non-human subject research and was deemed exempt by the Institutional Review Board at the University of Texas Medical Branch, Galveston.
Results
Descriptive statistics of the cohort
The study included 93,590 patients who underwent colectomy in 2013. After applying the exclusion criteria, the study cohort included 79,581 patients (Fig. 1). Half of the patients (n = 39,791) were younger (age 18–64 years) and half (n = 39,790) were older (age 65–90 years). Table 1 reports baseline characteristics of the study cohort. The mean age of the cohort was 63.2 ± 14.7 years, and 53.9% were female. Over half of patients (50.3%) were covered by Medicare and 36.9% by private insurance. The mean Elixhauser comorbidity score was 4.2 ± 6.9; 16.4% patients had no comorbidity; and 24.7% patients had four or more comorbidities. As per the APR-DRG, 22.7% of patients had major and 11.0% had an extreme loss of function. Most patients undergoing colectomy had a diagnosis of cancer (47.5%) or diverticulitis (26.8%). Most of the colectomies were performed in larger hospitals (64.3%), private, not-for-profit hospitals (74.1%), metropolitan teaching (47.8%), or nonteaching (44.1%) hospitals.
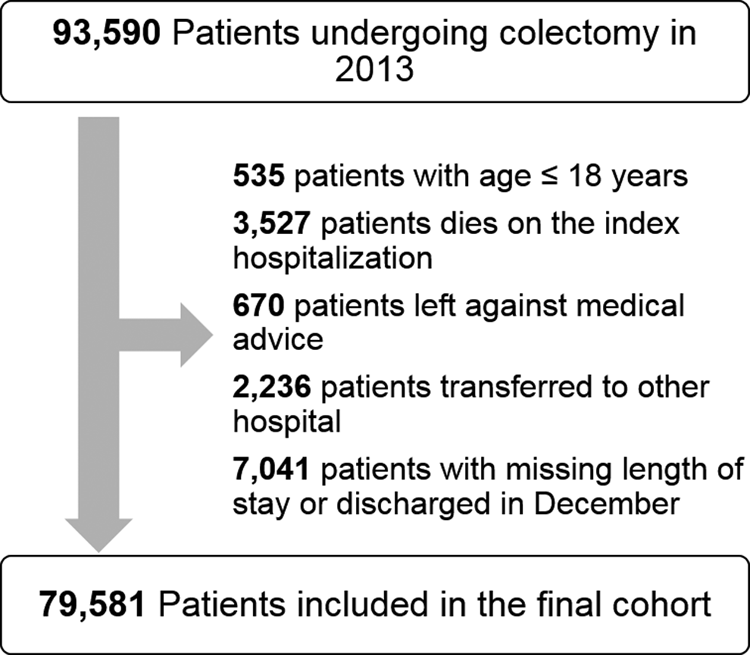
Cohort selection.
APR-DRG, All Patients Refined Diagnosis Related Groups; SD, standard deviation.
In 2013, 40.2% of patients underwent laparoscopic colectomy. The rate of laparoscopic colectomy was higher in younger patients (41.9%) than in older patients (38.5%). Patients undergoing laparoscopic colectomy were younger, more likely to be male, had higher household income, were covered by private insurance, had lower Elixhauser comorbidity scores, were more likely to have minor loss of function, and more likely to be diagnosed with cancer (Table 1). Laparoscopic colectomy was significantly more likely to be performed in hospitals with a high volume of colectomy procedures, private hospitals, large, and metropolitan teaching or nonteaching hospitals (Table 1).
Outcome rates in younger and older patients by colectomy approach
In unadjusted analyses, outcomes were better in patients undergoing laparoscopic colectomy compared to open colectomy, regardless of age group (Fig. 2). Compared to the open approach, laparoscopic colectomy resulted in lower 30-day readmission rates in both younger (8.1% versus 14.2%) and older (9.7% versus 16.1%) patients. Significantly fewer patients were discharged to SNF/ICF and home health following laparoscopic colectomy compared to open colectomy. Length of stay (younger: 5.2 days versus 9.5 days; older: 6.2 days versus 10.5 days) and median cost (younger: $14,033 versus $18,993; older: $14,979 versus $20,641) were lower in patients undergoing laparoscopic colectomy compared to open colectomy.

Outcome rates: overall and by age group.
Multivariable regression results
30-Day readmission
Patients undergoing laparoscopic colectomy were 20% less likely to be readmitted within 30 days (odds ratio [OR] 0.80, confidence interval [95% CI] 0.75–0.85). The interaction of age group with colectomy approach was not significant, indicating that laparoscopic colectomy offered similar benefits in reducing 30-day readmission rates to both age groups (Table 2).
Interaction of age group with colectomy approach was not significant. Therefore, it was removed from the model.
APR-DRG, All Patients Refined Diagnosis Related Groups; CI, confidence interval; OR, odds ratio.
Discharge destination
Patients undergoing laparoscopic colectomy were less likely to be discharged to SNF/ICF or home health, and the effect differed by age group (interaction was significant). Laparoscopic colectomy offered greater benefits to younger patients (SNF/ICF: OR 0.42, 95% CI 0.36–0.49; home health: OR 0.32, 95% CI 0.30–0.35) compared to older patients (SNF/ICF: OR 0.50, 95% CI 0.47–0.54; home health: OR 0.59, 95% CI 0.55–0.62) (Table 3).
APR-DRG, All Patients Refined Diagnosis Related Groups; CI, confidence interval; ICF, intermediate care facility; OR, odds ratio; SNF, skilled nursing facility.
Length of stay
Patients undergoing laparoscopic colectomy had 1.46 days (p < .0001) shorter stays compared to those receiving open colectomy. The effect was similar for both age groups; the interaction of age group with colectomy method was not significant (Table 4).
Interaction of age group with colectomy approach was not significant. Therefore, it was removed from the model.
APR-DRG, All Patients Refined Diagnosis Related Groups; SE, standard error.
Cost
Patients undergoing laparoscopic colectomy had significantly lower cost than those receiving the open approach; the effect was greater in younger patients than in older patients. Among younger patients, those undergoing laparoscopic colectomy had $1,466 (−$1,466−$0) lower cost (−1466 × 1−748 × 0 + 834 × 1 × 0 = −$1,466) compared to open colectomy (−1466 × 0−748 × 0 + 834 × 0 × 0 = $0). Older patients who underwent laparoscopic colectomy had $632 [−$1,380−(−$748)] lower cost (−1466 × 1−748 × 1 + 834 × 1 × 1 = −$1,380) compared to open colectomy (−1466 × 0−748 × 1 + 834 × 0 × 1 = −$748) (Table 4).
Association of other factors with outcomes
Several other patient and hospital factors were significantly associated with outcomes. Supplementary Table S1 (Supplementary Data are available online at www.liebertpub.com/lap) summarizes the significant factors. Females had a higher risk of 30-day readmission and were more likely to be discharged to SNF/ICF or home health, but had a shorter length of stay and lower cost. Patients with higher comorbidities and APR-DRG had increased risk of 30-day readmission, discharge to SNF/ICF or home health, greater length of stay, and higher cost. Median household income was associated with lower risk of home health discharge and lower length of stay, but higher cost. Medicaid patients had a higher risk of 30-day readmission, higher length of stay, and cost, whereas privately insured patients had a lower risk of all outcomes. The length of stay and cost were lower in private hospitals; however, patients admitted to private investor-owned hospitals were more likely to be discharged to SNF/ICF or home health. Large hospital size and metropolitan teaching hospitals were associated with increased home health discharge, length of stay, and cost.
Discussion
Using a nationally representative readmission database, our study described the association of laparoscopic colectomy with outcomes in younger and older patients. In 2013, 4 out of 10 patients underwent laparoscopic colectomy, with a slightly higher rate in younger patients. Laparoscopic colectomy patients had lower 30-day readmission rates, lower need for higher levels of care, shorter hospital stays, and less cost. Both younger and older patients undergoing laparoscopic colectomy benefited equally with lower risk of readmission and shorter hospital stays; however, younger patients benefited more with less discharge to SNF/ICF or home health and lower cost.
Since its introduction, the use of laparoscopic colectomy has increased from 2.2% in 1996 to 31.4% in 2009. 16 Our study found that, by 2013, 40.2% of all colectomies were performed laparoscopically. According to a study by Tsui et al., the adoption rate of laparoscopic colectomy was the lowest among all gastrointestinal surgical procedures. 17 Several factors may contribute to slow adoption of laparoscopic colectomy: a lack of knowledge about the benefits of minimally invasive surgery of the colon, the learning curve, the number of procedures performed by an individual surgeon, and the complexity of the procedure itself.
Since its introduction, a number of randomized controlled trials and observational studies have shown the advantages of laparoscopic colectomy. A Cochrane review of 25 randomized controlled trials demonstrated short- and long-term benefits of laparoscopic colectomy over open colectomy.18,19 Relatively less evidence is available in younger patients. One randomized controlled trial of postoperative complications and length of stay in 535 patients reported that laparoscopy colectomy improved short-term postoperative outcomes more in elderly (≥70 years) than in younger (<70 years) patients. 12 In contrast, our study showed that laparoscopic colectomy offered benefits over open approach; the benefit was greater in younger patients, especially for discharge destination and cost. The differences in results between this study and Frasson et al. can be explained by sample size, age group categorization, study design, and outcomes studied.
The need for postdischarge care was significantly lower for patients undergoing laparoscopic colectomy compared to open colectomy; only 6% (versus 19.3%) and 10.8% (versus 24.5%) patients were discharged to SNF/ICF and home health, respectively. These study findings were consistent with a prior study that also reported that laparoscopic colectomy patients were more likely to be discharged home without nursing care (OR 0.70). 1 Our study additionally found that younger patients were more likely than older patients to be discharged home without further postdischarge care.
The strengths of our study include the use of nationally representative readmission datasets and the inclusion of all patients 18 years and older and of all insurance statuses, including uninsured. Our study had the following limitations. We could not track readmission for patients hospitalized in one state and readmitted or transferred to a hospital in another state, because each SID uses different coding for its patient linkage numbers. NRD includes data from only 22 states. NRD does not provide information on patients' race and ethnicity; therefore, we were not able to adjust for this variable. We were unable to assess the penetration of enhanced recovery protocols between hospitals or between age groups.
In conclusion, the data reaffirm that laparoscopic surgery for colorectal resection is more beneficial than open surgery with fewer 30-day readmissions, fewer discharges to SNF/ICF or home health, shorter hospital stays, and less overall cost for both younger and older patients. As expected, younger patients benefit more from laparoscopic surgery than older patients; however, benefits accrue incrementally to all patients managed with laparoscopic resection.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.