
Abstract
Abstract
Aim:
To compare the safety of cholecystectomy in early laparoscopic cholecystectomy (ELC) and delayed laparoscopic cholecystectomy (DLC).
Methods:
We systematically searched PubMed, EMBASE, and Cochrane Library for studies that were published from January 1992 to March 2017. We included studies on patients with mild biliary pancreatitis and that reported the timing of cholecystectomy and the number of complications, readmissions, and conversion to open cholecystectomy. Moreover, we assessed the quality and bias risks of the included studies.
Results:
After screening 4651 studies, we included 3 randomized clinical trials and 10 retrospective studies. The included studies described 2291 patients, of whom 1141 (49.8%) underwent ELC and 1150 (50.2%) underwent DLC. The reported rate of complications for ELC (6.8%) was lower than that for DLC (13.45%). The reported rate of readmission for ELC was lower than that for DLC. The length of hospital stay was longer with DLC than with ELC. ELC and DLC did not have significantly different rates of conversion to open cholecystectomy and duration of surgery.
Conclusion:
This meta-analysis provides evidence that ELC is better than DLC in many aspects for acute mild pancreatitis patients undergoing laparoscopic cholecystectomy. ELC associated with few complications and readmissions, as well as a short length of hospital stay.
Introduction
A
Current international guidelines recommend early cholecystectomy in patients with mild biliary pancreatitis. However, different guidelines provide different definitions for “early.” The International Association of Pancreatology recommends cholecystectomy during the index admission of patients with mild biliary pancreatitis. 4 The American Gastroenterological Association suggests that cholecystectomy should be performed within the period of hospital admission and not beyond 2–4 weeks after discharge. 5 The British Society of Gastroenterology recommends cholecystectomy within the period of hospital admission or up to 2 weeks after admission. 6 This lack of consensus is reflected by several audits from the United Kingdom, Germany, 7 Italy, 8 and a large database study from the United States. 9
To determine the risk of recurrent biliary events in the period after mild biliary pancreatitis but before interval cholecystectomy and to determine the safety of cholecystectomy during index admission, van Baal et al. 10 conducted a systematic review of nine studies published until July 31, 2010. They found that a high rate of readmissions is clearly associated with interval cholecystectomy. They also suggested that randomized controlled studies on mild biliary pancreatitis should be performed. A meta-analysis 11 reported no difference in the number of complications between early laparoscopic cholecystectomy (ELC) and delayed laparoscopic cholecystectomy (DLC). However, this meta-analysis only included four articles with low methodological quality.
The related literature on the timing of surgery in mild biliary pancreatitis has grown substantially, and a multicenter randomized controlled trial (RCT) has been performed by the Dutch Pancreatitis Study Group.
In this study, we present an updated meta-analysis of the timing of cholecystectomy after mild biliary pancreatitis. We compare the outcomes of ELC and DLC in terms of the number of complications, readmission, and conversion to open cholecystectomy.
Materials and Methods
Literature search
We performed this systematic review and meta-analysis in accordance with the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis. 12 We searched the electronic databases PubMed, EMBASE, and Cochrane Library for “cholecystectomy” and “pancreatitis.” The language of full texts was limited to English. We only included studies that were published from January 1, 1992 to March 20, 2017. References to studies with potential relevance and review articles were manually screened to identify any previously unidentified eligible resources.
Inclusion and exclusion criteria
In this study, we defined ELC as initial cholecystectomy or laparoscopic cholecystectomy performed within 14 days after admission. The control group was defined as DLC. Mild pancreatitis was defined by either Ranson criteria or computed tomography criteria.
We included studies that: (1) compared ELC and DLC; (2) clearly defined ELC and DLC; (3) and provided information on the following essential outcomes: number of complications, readmission, and conversion to open cholecystectomy.
We excluded studies if they: (1) included children and pregnant patients; (2) included patients with pancreatitis of other origins; (3) included severe pancreatitis without separately reporting the results of mild pancreatitis; (4) included open cholecystectomy without separately reporting laparoscopic cholecystectomy; (5) did not report essential outcomes; and (6) were abstracts, case reports, case series, in vitro studies, and animal studies.
Outcome assessment
Primary outcomes included gallstone-related complications, which were defined as recurrent acute biliary pancreatitis, acute cholecystitis, cholangitis, or biliary colic. 13
Secondary outcomes included readmission, which was defined as rehospitalization before or after cholecystectomy; conversion to open cholecystectomy; duration of surgery; and length of hospital stay.
Data extraction
After the exclusion of duplicated studies, 2 investigators (D.-J.Y. and H.-M.L.) independently evaluated the studies for eligibility. Disagreements between the reviewers concerning the inclusion or exclusion of a study were resolved by consensus and by consultation with a third reviewer (Q.G.) when necessary. We extracted the following information from each eligible article: name of the first author, publication year, country, study design, sample size, demographic characteristics, number of complications, hospital readmission, number of conversion to open cholecystectomy, duration of surgery, and length of hospital stay.
Quality assessment
Two authors (D.-J.Y. and H.-M.L.) used the Newcastle–Ottawa Scale (NOS) to assess the methodological quality of the included studies. Quality was calculated based on the following three aspects of study design: patient selection, cohort compatibility, and outcome. Funnel plots were used to examine publication bias.
Statistical analyses
Dichotomous variables were analyzed by estimating the odds ratio (OR) with a 95% confidence interval (95% CI), whereas continuous variables were analyzed using the weighted mean difference with 95% CI. If continuous variables in the article only included the median and range or interquartile range, we converted these variables to mean and standard deviation (SD) using a formula.14,15 Heterogeneity across trials was investigated using the Cochran Q test and measured with the I2 statistic. I2 values that exceeded 25%, 50%, and 75% represented low, moderate, and high heterogeneity, respectively. 16 If no heterogeneity was absent, then a fixed effects model based on the Mantel and Haenszel estimator was used. Otherwise, a random effects model based on the DerSimonian and Laird estimator was used. For all statistical analyses, except for heterogeneity and publication bias, at two-sided, P < .05 was regarded as statistically significant. Statistical analyses were performed with Review Manager Software program version 5.3.
Results
The flow diagram of the study is shown in Figure 1. A search of the electronic databases, PubMed, EMBASE, and Cochrane Library, yielded 7736 records. After duplicates were removed, 4651 records remained. After screening titles and abstracts, 54 abstracts were selected for detailed assessment, and 41 articles were excluded. The reasons for excluding these articles are detailed in Figure 1. Finally, 13 studies17–29 were included for data extraction.
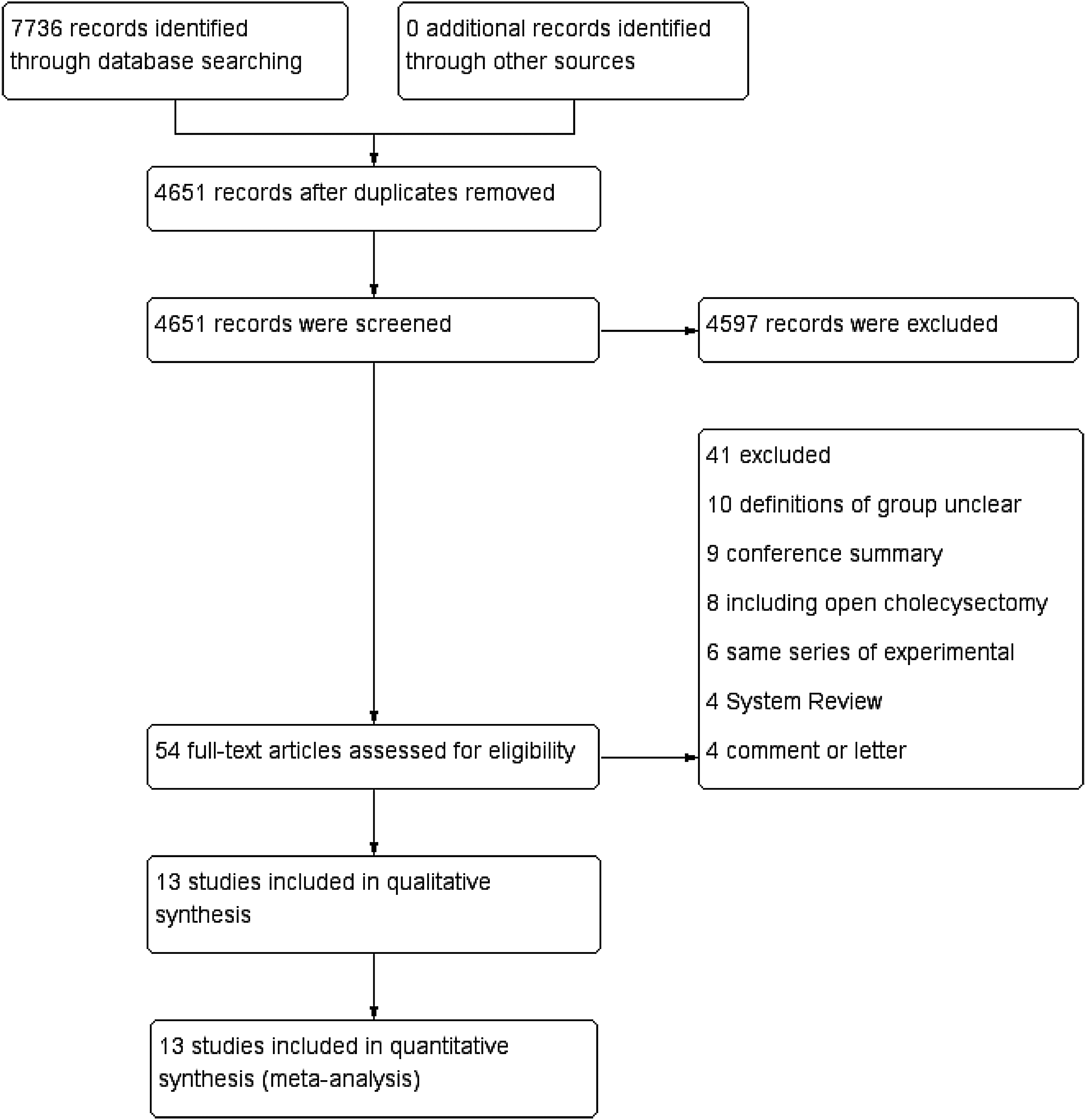
The flow diagram.
Study characteristics
The characteristics of the included studies are presented in Table 1. We included 13 studies with 2291 patients in our meta-analysis, including 3 randomized clinical trials19,21,24 and 10 retrospective studies.17,18,20,22,23,25–29 The sample size of the studies varied from 44 to 350. A total of 1141 patients underwent ELC and 1150 patients underwent DLC.
DLC, delayed laparoscopic cholecystectomy; ELC, early laparoscopic cholecystectomy; IQR, interquartile range; n, number of patients; RCT, randomized clinical trial; SD, standard deviation.
Quality assessment using the NOS showed that the 13 included studies were of high quality (Table 2).
COC, conversion to open cholecystectomy; DLC, delayed laparoscopic cholecystectomy; DOS, duration of surgery; ELC, early laparoscopic cholecystectomy; LOS, length of hospital stay; NOS, Newcastle–Ottawa Scale; NR, not reported; SD, standard deviation.
Meta-analysis results
The results of data extraction are shown in Table 2 and those of meta-analysis are shown in Figures 2–6.

Gallstone-related complications. 95% CI, 95% confidence interval; DLC, delayed laparoscopic cholecystectomy; ELC, early laparoscopic cholecystectomy; NRCT, nonrandomized controlled trial; RCT, randomized clinical trial.
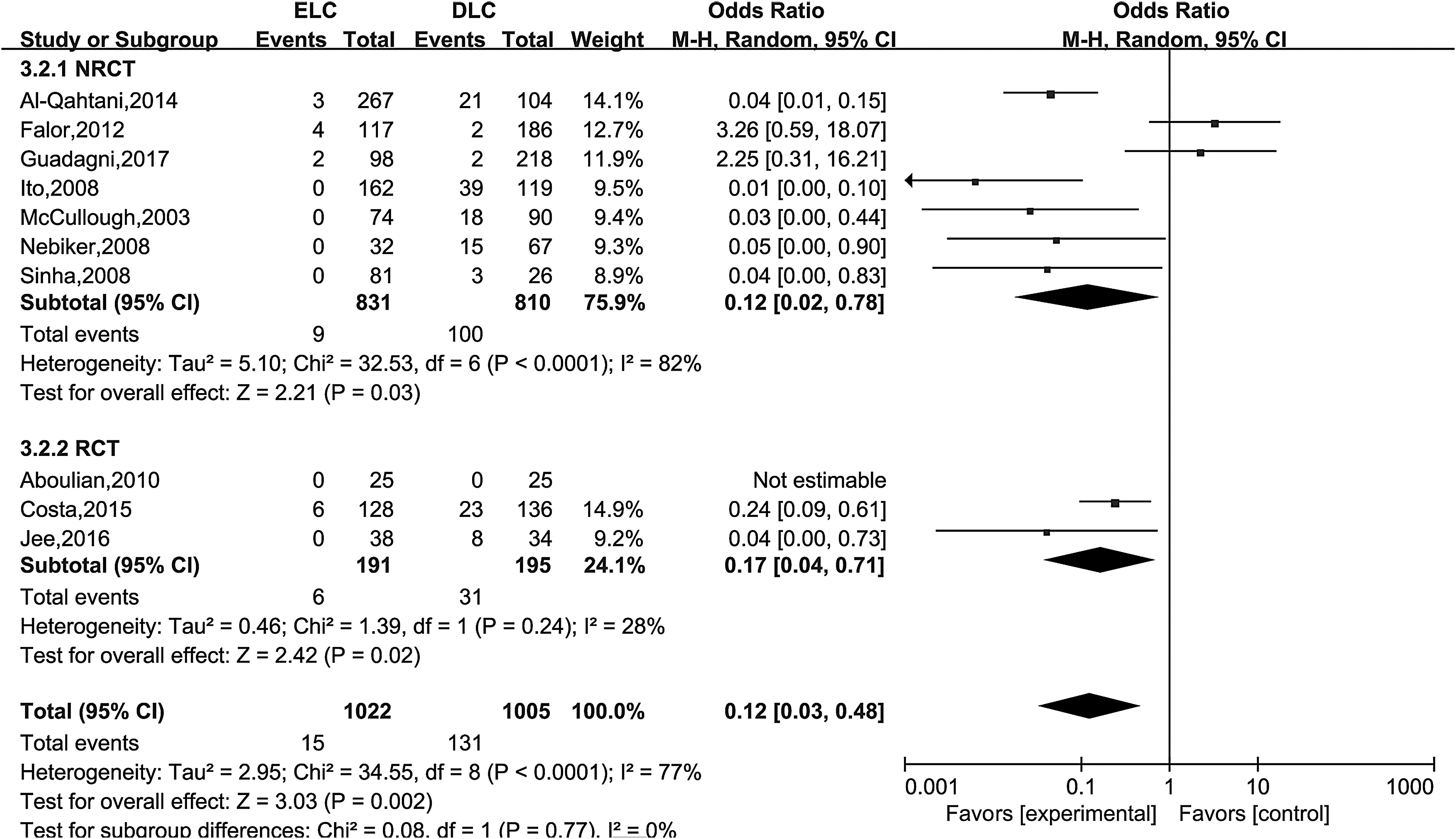
Readmission. 95% CI, 95% confidence interval; DLC, delayed laparoscopic cholecystectomy; ELC, early laparoscopic cholecystectomy; NRCT, nonrandomized controlled trial; RCT, randomized clinical trial.
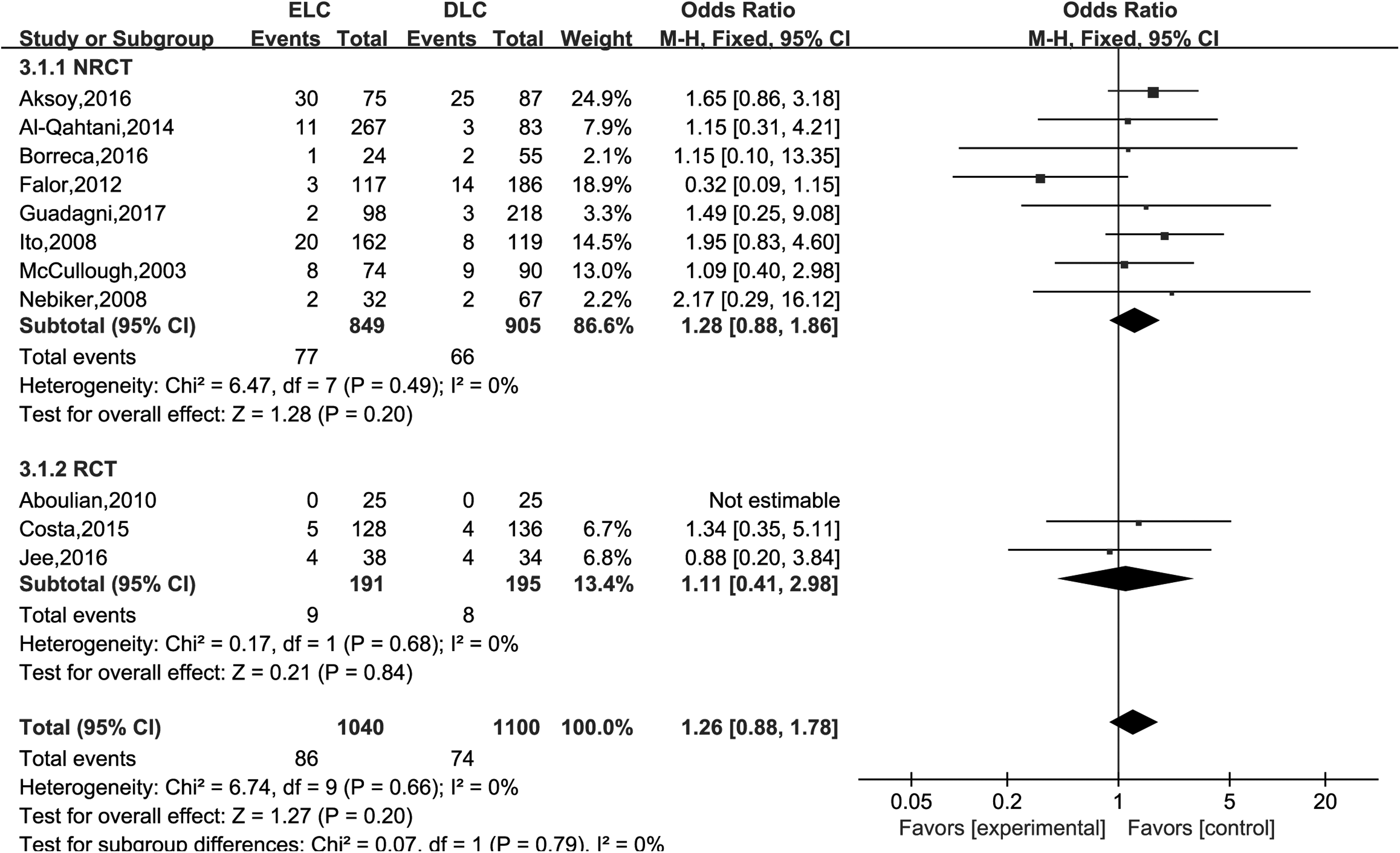
Conversion to open cholecystectomy. 95% CI, 95% confidence interval; DLC, delayed laparoscopic cholecystectomy; ELC, early laparoscopic cholecystectomy; NRCT, nonrandomized controlled trial; RCT, randomized clinical trial.
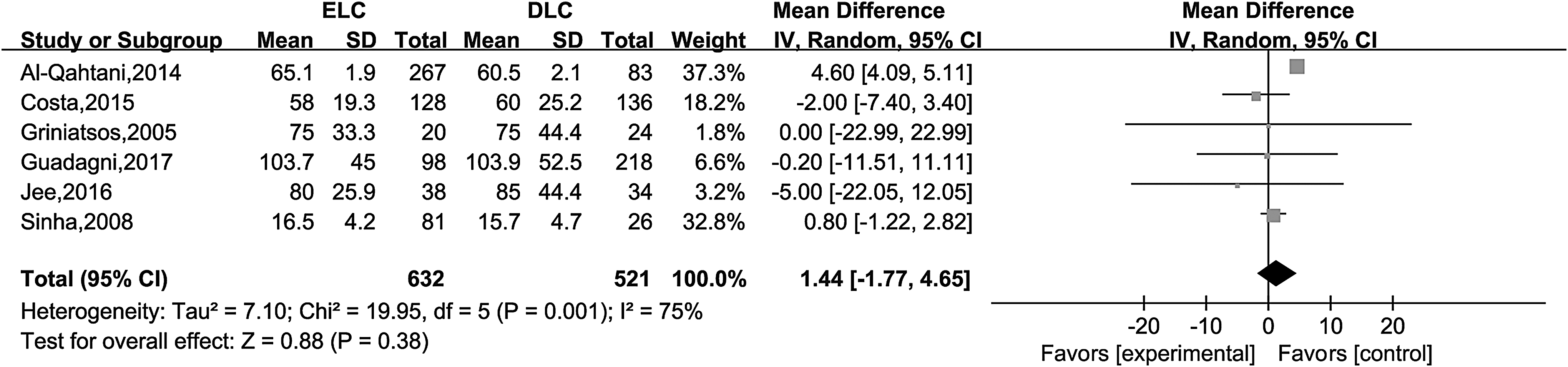
Duration of surgery. 95% CI, 95% confidence interval; DLC, delayed laparoscopic cholecystectomy; ELC, early laparoscopic cholecystectomy; SD, standard deviation.
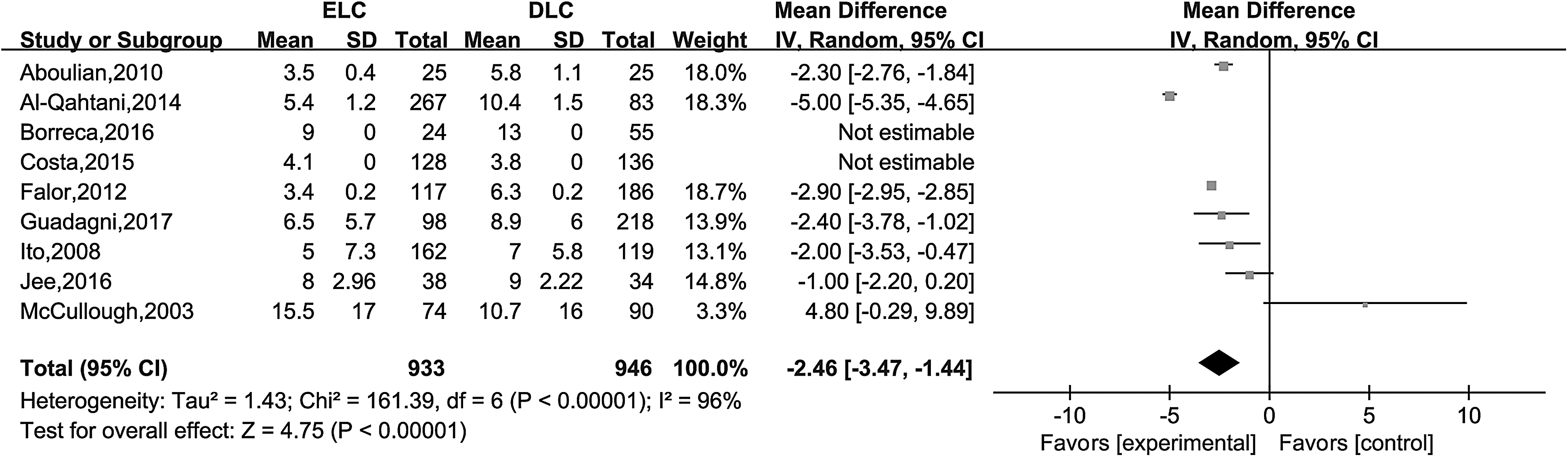
Length of hospital stay. 95% CI, 95% confidence interval; DLC, delayed laparoscopic cholecystectomy; ELC, early laparoscopic cholecystectomy; SD, standard deviation.
Complications
All studies reported primary outcome. The overall rate of complications is 231/2291 (10.1%). The rate of complications was 78/1141 (6.8%) and 154/1150 (13.45%) in the ELC and DLC groups, respectively. The result of the meta-analysis showed that complications between ELC and DLC group were significantly different (OR: 0.45, 95% CI: 0.33, 0.61; P < .00001; Fig. 2) with a high degree of heterogeneity (I2 = 76%, P < .00001).
Readmission
The overall readmission rate reported in 10 articles17,19,21–27,29 was 146/2027 (7.2%). ELC (1.5%) and DLC (13.0%) had significantly different rates of readmission (OR: 0.11, 95% CI: 0.07, 0.19; P < .00001; Fig. 3) with a high degree of heterogeneity (I2 = 77%, P < .00001).
Conversion to open cholecystectomy
Conversion to open cholecystectomy was reported in 11 studies17–25,27,29 that included 2140 patients. Conversion to open cholecystectomy occurred in 160 patients (7.5%). ELC (8.3%) and DLC (6.7%) did not have significantly different rates of conversion to open cholecystectomy (OR: 1.26, 95% CI: 0.88, 1.78; P = .20; Fig. 4) and without heterogeneity (I2 = 0%, P = .66).
Duration of surgery
Six articles18,19,21,22,26,28 reported the duration of surgery. The duration of surgery was not significantly different between groups (OR: 1.44, 95% CI: −1.77, 4.65; P = .38; Fig. 5) and had a high degree of heterogeneity (I2 = 75%, P < .00001).
Length of hospital stay
Nine articles17,19–24,27,29 reported the length of hospital stay, and only seven articles17,19,22–24,27,29 provided data. The length of hospital stay in the remaining two articles20,21 was not estimated due to incomplete data. The length of hospital stay was significantly different between groups (OR: −2.46, 95% CI: −3.47, 1.44; P = .38; Fig. 6; P < .00001) and with a high degree of heterogeneity (I2 = 96%, P < .00001).
Subgroup and sensitivity analysis
Complications and readmission exhibited substantial heterogeneities of I2 = 76% and I2 = 77%, respectively. Therefore, subgroup and sensitivity analyses were performed (Table 3). The included studies were divided into subgroups on the basis of study design, publication date, and study area. The types of study design included RCT and non-RCT (NRCT). The boundary point for publication date was set at 2011.
95% CI, 95% confidence interval; NRCT, nonrandomized controlled trial; OR, odds ratio; RCT, randomized clinical trial.
No heterogeneity (I2 = 0%) was observed in the RCT, NRCT, and BEFORE subgroups. High heterogeneity was observed in the AFTER (I2 = 83%), European and American (I2 = 78%), and Others (I2 = 79%) subgroup. RCT was statistically significantly different between ELC and DLC. The Other subgroups were not different between ELC and DLC.
Readmission was not heterogeneous (I2 = 0%) in the BEFORE and Others subgroup. High heterogeneity (I2 = 82%) was observed in the NRCT, AFTER, and European and American subgroup. And RCT had a moderate degree of heterogeneity (I2 = 28%). There was significant difference in the rate of readmission between ELC and DLC in NRCT, RCT, BEFORE, and Others subgroup. AFTER and European and American subgroups were not different.
Assessment of publication bias
To examine any publication bias in the included studies, we constructed funnel plots of the included ORs using Review Manager 5.3. The funnel plots are shown in Figure 7. Performance bias was observed in complications (Fig. 7A) and readmission (Fig. 7B). No evidence of publication bias of conversion to open cholecystectomy was observed (Fig. 7C).
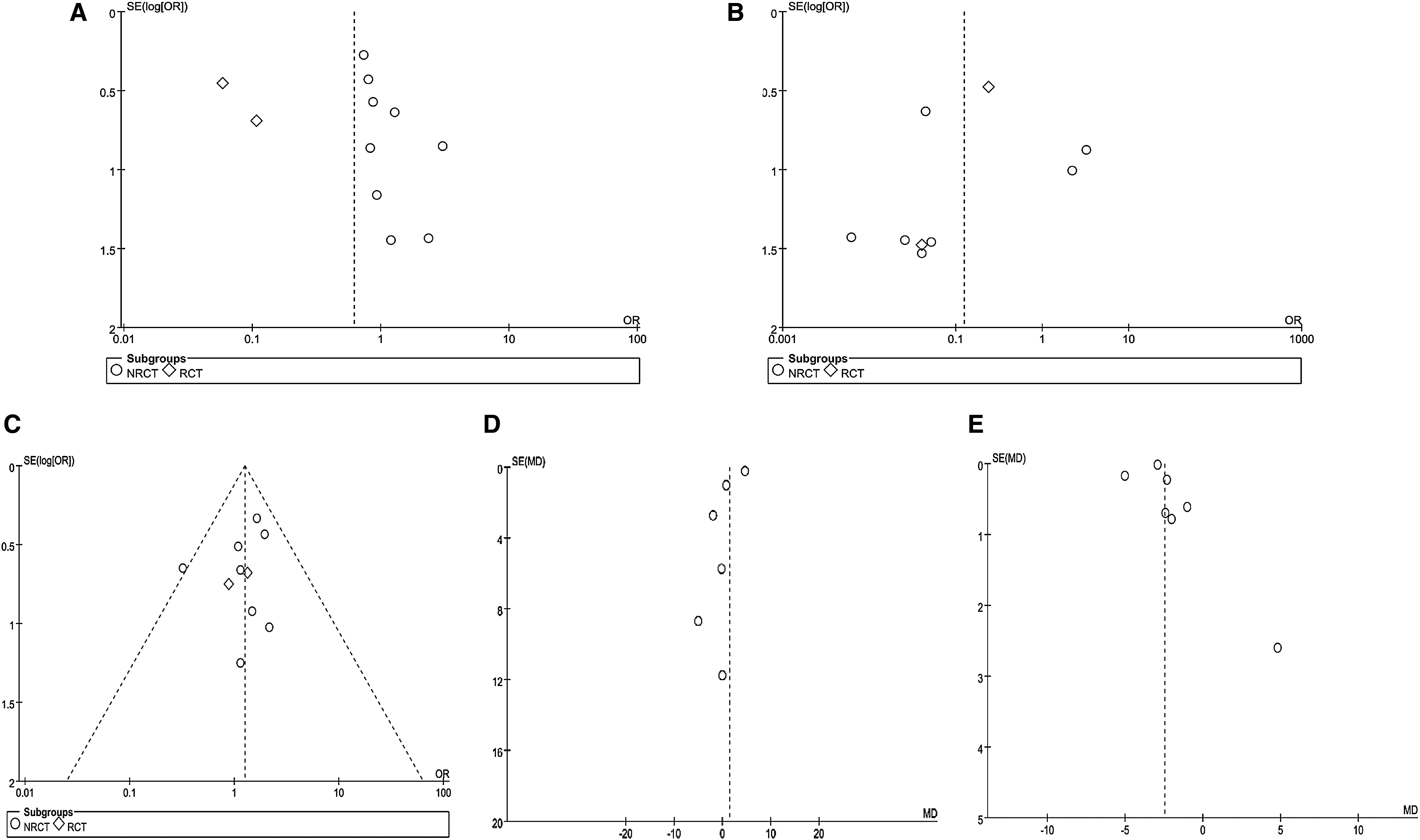
Outcomes of studies as funnel plots.
Discussion
We found that DLC resulted in higher rates of complications and readmission than ELC. The rates of conversion to open cholecystectomy between ELC and DLC were comparable. However, we cannot be certain that the two groups are truly comparable given that baseline characteristics were often not provided in the included articles.
We found that ELC and DLC had significantly different complication rates (Fig. 2). The outcomes of the subgroup analysis of 10 retrospective articles (NRCT subgroup) showed no difference in complications between ELC and DLC, whereas those of 3 RCT articles (RCT subgroup) showed that DLC has a higher rate of complications than ELC. The results of RCT are more reliable than those of retrospective studies owing to the study design and control of confounding factors in RCT. Therefore, in RCT, the characteristics of the patients in different groups are homogenous. By contrast, retrospective studies are prone to selection bias. For example, interval cholecystectomy might be performed in patients with advanced age, with substantial comorbidity, or with severe pancreatitis. ELC decreases the risk of recurrent gallstone-related complications. Cholecystectomy in patients with mild gallstone pancreatitis can be performed safely during ELC. ELC and DLC in the BEFORE and AFTER subgroups did not have significantly different complication rates (Table 3).
The overall readmission rate reported in eight articles was 146/2017 (7.2%), which was lower than the 18% reported in an accent systematic review. 10 This result indicated that ELC decreases the rate of readmission. In subgroup analysis, the RCT and NRCT groups showed the same result, which favors DLC in mild blood pressure, resulting in readmission (Fig. 3). The high heterogeneity of the NRCT group was contributed by the studies of Falor et al. 23 and Guadagni et al. 17 Removing these studies decreased the heterogeneity of NRCT to 0%. In cases where gallstones were untreated, the recurrence rate of BP was 32%–61%. 30 Therefore, ELC during the first admission is safe and recommended.4,31
The rates of conversion to open cholecystectomy have been reported in the literature as 0%–27.7%.3,32,33 We found that the rate of conversion to open cholecystectomy is 7.5%, indicating that DLC does not increase the need for conversion to open surgery. However, we were unable to analyze the reason for this result because some studies did not report the reasons for conversion. An accent article reported that the risks of conversion might be related to gender, age, acute cholecystitis, previous upper abdominal surgery, and the experience of the surgeon. 34
Only one in six analysis articles directly provided the mean and SD of surgery duration. We calculated other mean and SD values from formula, thus causing a high degree of heterogeneity. The timing of laparoscopic cholecystectomy did not affect the duration of surgery. This outcome is different from the assumption that ELC will increase the difficulty of surgery. We also converted the data on the length of hospital stay using formula. We found that DLC is associated with a significantly longer length of hospital stay and that DLC patients require readmission and a longer duration of conservative treatment. Thus, DLC increases hospitalization costs and consumes more medical resources.
An accent review article 10 provided an important information on the high readmission rates (18%) for interval cholecystectomy, leading to delayed multicenter RCT. 21 However, several included articles did not provide comparison groups. Moreover, some articles may be considered as reporting on outcomes before and after cholecystectomy and not on the outcomes of early and delayed cholecystectomy. The methodological quality of most articles is moderate or low. An accent meta article 11 defined early cholecystectomy as cholecystectomy within 48 hours and thus included only four articles for analysis. Three of the four articles were written by the same research group and had poor or extremely poor methodological quality. Therefore, the result of this meta-analysis may be inaccurate.
Although most guidelines recommend early cholecystectomy, many studies have shown that interval cholecystectomy is usually performed in mild biliary pancreatitis patients. For example, a Swedish study 35 that included more than 1500 patients with mild acute biliary pancreatitis showed that up to 10% of LC cases are performed with interval procedures within 30 days of admission and that 68% of patients do not receive surgery or sphincterotomy within 30 days of admission. A British study reported that only 14.7% of 25,000 patients with gallstone-related disease underwent cholecystectomy within the same admission period after acute hospitalization. 36 Several international audits10,37 had shown that cholecystectomy is often not performed until 6 weeks after discharge and not at all in many patients.
The recurrent attack of biliary pancreatitis could be severe and threaten life.27,38 Why, then, do so many doctors delay cholecystectomy? On the one hand, inflammation and edema are believed to distort the anatomy of the biliary tract, thereby complicating dissection and increasing the risks of conversion to open cholecystectomy and of surgical complications, such as bile duct injury, during early cholecystectomy.39,40 On the other hand, emergency resources are often scarce; thus, by delaying cholecystectomy, the surgeon could schedule surgical treatment. Doctors who support ELC believe that it reduces the risk of recurrent gallstone-related events (e.g., recurrent acute biliary pancreatitis, acute cholecystitis, cholangitis, or biliary colic).6,41
Our study was limited by the following factors: First, the unclear definition of ELC. In 13 articles, ELC was performed within 2, 3, 7, or 14 days within admission, or even within the same time as admission (without providing the specific time). Therefore, the precise timing of early cholecystectomy remains unclear. Second, the included studies were highly heterogeneous because of their different study designs. Finally, we only included three randomized trials.
Footnotes
Author Contributions
All of the authors contributed to the collection and analysis of the data and to the preparation of the report. The corresponding author had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Disclosure Statement
No competing financial interests exist.