
Abstract
Abstract
Objectives:
Pain continues to be the most important limiting factor affecting the early discharge of patients after laparoscopic cholecystectomy (LC). Our aim was to conduct a randomized case controlled study to predict the evolution of various components of postoperative pain by using ropivacaine 0.2% at intraperitoneal and intraincisional locations; and to further use this information to make a model predicting early discharge of patients.
Methods:
Two hundred forty-four patients underwent elective four-port LC. Patients were triple blindly randomized. All patients received ∼23 mL of solution, of which 20 mL was given intraperitoneally and ∼3 mL was given intraincisionally. Solution was either normal saline or drug (0.2% ropivacaine) depending on the group (controls [n = 77], intraperitoneal group [n = 80], and intraincisional group [n = 87]). Five different pain scales were used for assessment of overall pain. Only those patients with a Visual Analog Scale (VAS) ≤3, Numeric Rating Scale (NRS) ≤3, Visual Descriptor Scale (VDS) ≤ “Slight Pain,” Faces Pain Scale-Revised (FPS-R) ≤2, and Activity Tolerance Scale (ATS) ≤ “Can Be Ignored” along with absence of use of rescue analgesia and shoulder pain were considered for “Discharge Criteria.”
Results:
Incisional component of pain was found to be the main component of pain that predominated in the immediate postoperative period. However, it declined rapidly over 12 hours and was then dominated by the visceral component. Shoulder component peaked around the eighth postoperative hour. Seven percent of patients in controls could be discharged at the 12th postoperative hour and 18% at the 24th hour. In the intraperitoneal group, 18% and 61% patients could be discharged at the 12th and 24th hour, respectively, as compared with 57% and 78% in the intraincisional group using the “Discharge Criteria.” “Discharge Criteria” was 100% effective in predicting patients' acceptance to go home.
Conclusion:
The effect of local anesthetic at intraincisional and intraperitoneal sites is additive with drug catering to different components of pain. We recommend using the “Abbreviated Discharge Criteria” routinely in practice to check for patients' eligibility to be discharged.
Introduction
L
Pain in LC has multiple components. Pain is due to the skin incision made at port sites; it is due to the tissue dissection done to remove the gall bladder (GB), that is, the visceral component of pain; and it is also due to the stretching of the diaphragm caused by the pneumoperitoneum manifesting as shoulder pain. 8 Adequate control of all of these components of pain is required so that the patient remains relatively pain free and could be sent home early. Several modalities have been in use to control pain in patients undergoing LC. A paradigm shift has occurred with the identification of potential of early pain relief in operative surgery using local anesthetics (LAs). Ropivacaine seems to have the greatest margin of safety of all long-acting LAs that are in current common practice. 9 So we decided to use ropivacaine to cater to all components of pain as mentioned earlier and to see how pain evolves after LC!
Evolution of various components of pain have been the matter of discussion in several previous studies,5,8,10–12 but they have predicted its characteristics and evolution in vastly different manners. We have tried to resolve this debate in our study. The primary objective of this study was to conduct a randomized case controlled prospective study to predict the evolution of various components of pain after an uncomplicated LC by using ropivacaine 0.2% at intraperitoneal and intraincisional locations to curb the three main components of pain, namely, incisional, visceral, and shoulder components; and to further use this information to make a model predicting early discharge of patients.
Materials and Methods
The study was designed as a prospective randomized case control study involving patients who were subjected to LC in a single unit by a single surgeon in the Department of Surgery of a tertiary teaching government institute over a period of 36 months. Ethical approval was provided by the Ethical Committee of the University and was conducted in accordance with guidelines of “Good Clinical Practice” and the “Declaration of Helsinki.” Written informed consent was obtained from all patients for participation in the study. The drug used for the study was “Ropivacaine 0.2%” (Injection Ropin 0.2%; Neon Laboratories Ltd., Mumbai, India), which is dispensed as a 20 mL ampoule.
Inclusion criteria
Only female patients in the age group of 18–65 years conferring to Grade I or II of the American Society of Anesthesiologists (ASA) physical status classification system, undergoing elective uncomplicated LC for symptomatic cholelithiasis by a single surgeon, were included in this study.
Exclusion criteria
Patients with known allergic reactions to LAs; cases that were converted to open cholecystectomy, as well as patients with major intra-operative complications; patients suffering from acute cholecystitis, empyema or malignancy of GB, having history of chronic pain, or those taking frequent analgesics or opioids preoperatively; patients with peptic ulceration, bleeding disorders, impaired renal and/or hepatic function, and sensitivity to nonsteroidal anti-inflammatory drugs or opioids; patients in whom GB stones are found incidentally on ultrasonography (USG) (asymptomatic cholelithiasis); patients suffering from severe chronic medical diseases and morbid obesity; and patients unable to comprehend instructions or having communication problems were excluded from the study.
Patients with an operative duration of >75 minutes and intra-operative drain insertion (assuming that this predicted an intra-operative complication) were also excluded. Male patients are known to have better pain tolerance profile than female patients, 13 so they were excluded from this study as they could be readily discharged early and, thus, could have influenced final results. Patients who were not able to tolerate oral feeds (with or without postoperative nausea/vomiting) or having urinary retention at any point of time in the 24-hour postoperative period or who could not be ambulated at least once in the evening were excluded from final analysis so that the effect of pain alone could be studied to make a predictive model for discharge.
Study design and study groups
It was a prospective randomized case control triple-blind study in which neither the patient nor the investigator that is, myself, nor the operating surgeon knew whether the drug would be used or not; and if the drug is going to be used, what would be its location. Patients were, thus, divided into three groups—Controls: those who did not receive any drug but received normal saline (NS) at both sites, that is, intraperitoneally as well as intraincisionally; intraperitoneal ropivacaine group (IPR group): those who were given ropivacaine intraperitoneally and NS intraincisionally; and intraincisional ropivacaine group (IIR group): those who were given ropivacaine by infiltrating it locally at the skin incision site and given NS intraperitoneally.
Methodology
During initial outpatient visits, the patients were fully assessed and a confirmed diagnosis was made on the basis of USG abdomen. On admission, patients were explained about the study and informed consent was obtained for participation in the study. Pain was assessed at five points of time in the postoperative period, that is, at 30 minutes (0.5 hour), 4 hours, 8 hours, 12 hours, and 24 hours. Pain was assessed by both objective and subjective methods. The frequency of extra doses of analgesics (rescue analgesia [RA]) given over and above the standard analgesia and shoulder pain was also noted. The different pain scales used were as follows:
Subjective scales
1. Visual Analog Scale (VAS)—A 10 cm line was used, and the patient was told to mark on it by using a pen regarding the pain perceived by him/her.
2. Eleven-Point Numeric Rating Scale (NRS-11/NRS)—The patient was asked to assign a number to pain, what he/she thought was appropriate to describe the pain.
0—None; 1, 2, 3—Mild; 4, 5, 6—Moderate; 7, 8, 9, 10—Severe
3. Visual Descriptor Scale (VDS)—A 7-point subjective scale in which the patient was told to indicate verbally about the perception of pain as experienced.
No Pain (NP)/Slight Pain (SLP)/Mild Pain (MLP)/Moderate Pain (MP)/Severe Pain (SP)/Extreme Pain (EP)/the Most Intense Pain Imaginable (MIPI)
Objective scales
1. Faces Pain Scale-Revised (FPS-R)—This is an objective method of pain assessment in which facial expressions of the patient are assessed by the investigator, as depicted in Figure 1 and scored accordingly.
2. Activity Tolerance Scale (ATS)—This is a combined objective and subjective method in which the patient is asked subjectively for the five grades of activity mentioned later and the criterion told by the patient is further objectively assessed by the investigator. By convention, this scale was not used to assess the patient at 30 minutes postoperatively as all the patients remained in the recovery room at that time on the stretcher.
No Pain (NP)/Can Be Ignored (CBI)/Interferes With Task (IWT)/Interferes With Concentration (IWC)/Interferes With Basic Needs (IWBN)/Complete Bed Rest Required (CBRR)

Faces Pain Scale-Revised (FPS-R).
Patients were explained about the usage of the subjective pain scales and how to convey them to the investigator. The objective pain scales were assessed by the investigator. After routine standardized preoperative evaluation, patients were shifted to the operating room (OR) where they were made to choose from three preformed envelopes. These contained the information as to in what study group the patients would belong to. The chosen envelope was then given to an independent OR attendant from a different OR, who then prepared one 20 mL and one 5 mL syringe. The 20 mL syringe contained either 20 mL of undiluted drug or 20 mL of NS depending on the group. Similarly, the 5 mL syringe contained either 5 mL of undiluted drug or 5 mL of NS, again depending on the group. Thus, for the control group, both syringes contained NS. For the IPR group, the 20 mL syringe contained the drug whereas the 5 mL syringe contained NS. In the IIR group, the 20 mL syringe contained NS whereas the 5 mL syringe contained the drug. Thus, all patients received intraperitoneal instillation as well as intraincisional infiltration at all points of time but nobody in the OR knew what was being given. The patient's name and hospital admission number was written on the envelope and it was put in a locker. The envelopes were opened only after completion of the study.
Anesthetic technique protocol
All patients received the same anesthetic technique. Anesthesia was induced with intravenous (IV) fentanyl 1.5 μg/kg, propofol 2 mg/kg, and atracurium 0.6 mg/kg. Fentanyl was used for pain relief because it has a duration of analgesic action of 30–60 minutes, 14 so it was not likely to affect the postoperative assessment of pain. After tracheal intubation, the patient's lungs were mechanically ventilated and anesthesia was maintained with 60% nitrous oxide, oxygen, and one minimum alveolar concentration isoflurane. A further bolus of fentanyl 50 μg was given after 45 minutes of the initial dose or earlier if heart rate or BP increased by more than 20% of baseline value after incision. At the end of the surgery, residual neuromuscular blockade was antagonized with IV neostigmine 2.5 mg and glycopyrrolate 0.5 mg.
Operative technique protocol
All the operations were performed by a single surgeon, so the basic operative technique was similar in all the patients. A standard four-port LC was performed in all patients. A 10-mm horizontal skin incision was made at the superior aspect of the umbilicus and then deepened through the subcutaneous fat to the anterior rectus sheath. The infra-umbilical skin was pinched up with the left hand along with the underlying soft tissue (to avoid injury to viscera and bowel, especially in the case of any adhesions). A Veress needle was inserted through the incision with the right hand, directed toward the midline. The Veress needle was connected to the insufflator. Carbon dioxide (CO2) was insufflated into the peritoneal cavity at the rate of 2 L/min, up to a pressure of 10 mm of Hg. The Veress needle was then removed. A 10-mm bladed trocar with a sheath was placed at the umbilical port. The trocar was removed, keeping the sheath in place. Insufflation of CO2 was initiated at the rate of 2 L/min, up to a maximum pressure of 12–14 mm Hg. The gas flow rate was then kept at 6 L/min during the procedure. The 10-mm epigastric port incision and the 5-mm right midclavicular and right anterior axillary incisions were given under vision.
At the end of the procedure, intraperitoneal instillation was done by using the irrigation apparatus under the right hemi-dome of the diaphragm and in the GB fossa. The amount of intraperitoneal instillation was kept at 1 mL/cm of length for uniformity of comparison at the two locations. We took the length of the right hemi-dome to be roughly 16 cm and, thus, used 16 mL intraperitoneal instillation along the right hemi-dome. We also used 4 mL of solution in the GB fossa.
All of the skin incisions were closed with 3-0 nonabsorbable monofilament nylon suture on a cutting needle, followed by aseptic dressing. Intraincisional infiltration was done by using the standardized amount, that is, 1 mL/cm of length of incision. For this, length of the incision site was measured by using a scale and the drug was infiltrated accordingly. Thus, if a port had to be increased to 12 mm for some reason, 1.2 mL of intraincisional infiltration was used. This ensured the uniformity of drug dosage used in the IPR and IIR groups. The duration of surgery was measured from the time of the first incision to the final stitch taken at port sites.
Postoperative pain control protocol
Pain control in postoperative patients was in two forms: Standard Pain Control: Injection diclofenac sodium 75 mg/1 mL (aqueous) IV 12 hourly was used as standard analgesia in all the patients irrespective of what study group the patient belonged to; RA: Injection tramadol 100 mg IV stat was used for providing analgesia at any point of time for those patients who demanded for additional pain relief, in case the pain was very distressing to them. Moreover, all the patients who had a VAS and/or NRS >6 or agonizing pain at any point of time were offered rescue analgesic, especially at the 0.5th hour when the pain is usually higher. Some patients might still need additional analgesia beyond this point. But the dose of injection tramadol cannot be repeated for the next 6–8 hours due to the possibility of drug accumulation/toxicity. 15 So, a dermal patch of Diclofenac Diethyl Amine (Nupatch 100 mg/50 cm2; Zydus Cadila, Ahmedabad, India), which is a slow-release drug delivery system, was used as a second line of RA. It was offered to all the patients who had already been given injection tramadol and even after 2 hours of its administration as timing of peak effect of tramadol ≈2 hours, 15 if the patient had a VAS and/or NRS >6, if the patient had agonizing pain, or if the patient still asked for additional pain relief.
Patient ambulation, oral sips allowance, and the “Discharge Criteria” protocol
All patients were allowed oral sips 6 hours postoperatively and evaluated for any immediate increase in pain or any nausea/vomiting. Patients were ambulated in the presence of a resident and sent to toilet for passing urine at the same time. It was our experience that most of the patients having VAS ≤3 (collectively considering all components of pain), at any point of time postoperatively, when offered discharged were willing to go home. Similarly, the same values at which most of the patients were willing to go home when offered discharges, at any point of time postoperatively, for different pain scores were calculated. For NRS it was a score of ≤3, for VDS it was a pain level of at least “slight pain (SLP)” or less, for FPS-R this value was ≤2, and, finally, for ATS pain score it was a pain level corresponding to “can be ignored CBI” or less. Thus, only those patients having a VAS ≤3, NRS ≤3, VDS ≤ “SLP,” FPS-R ≤ 2, ATS ≤ “CBI,” no requirement of RA, and no shoulder pain were collectively considered for framing a “Discharge Criteria” model. This was done to minimize the number of patients who could be falsely assumed to be discharged based on one pain scale only.
Statistical analysis
At the end of the study, the envelopes were opened and statistical calculations were made. Data analysis was done with IBM SPSS Statistics® (Statistical Package for Social Sciences) software version 24 (IBM Corp., Armonk, NY). Mean and standard deviation were observed for continuous forms of data such as age, operative duration, numeric pain scores, and so on. Such data were further evaluated for significance by Student's t-test (for comparing two groups), analysis of variance (ANOVA) (for comparing more than two groups), and post hoc analysis in the form of Tukey's Honest Significance Difference (HSD) test. Tukey's HSD test is more conservative in nature as compared with t-test, so it has more value in the interpretation of results. So, wherever the findings of t-test and Tukey's HSD test disagreed, the results of the latter presided over the former. For categorical data, such as results of VDS, FPS-R, ATS, and so on, significance testing was done by Fisher's exact test (FET). A P value of less than .05 was considered statistically significant for all practical applications.
Observations and Results
Figure 2 shows the flowchart of study design for inclusion of patients. Three hundred twelve female patients were eligible for inclusion, but only 291 of them gave consent for inclusion in the study. Further, 33 patients could not be randomized because they either withdrew their consent or did not meet inclusion criteria or had intra-operative technical problems/conversions or were operated as emergency cases (Fig. 2). Thus, 258 patients underwent standard four-port LC. Further, 14 patients could not be included in the final analysis as they had significant complaints other than pain such as postoperative nausea or vomiting and/or inability to tolerate oral feeds, inability to fully mobilize postoperatively, and urinary retention or burning micturition. Two hundred forty-four patients completed 4-port LC and the 24-hour post-LC evaluation period and were, thus, considered for final analysis. The age distribution of patients is depicted in Figure 3. The mean age of patients was 37 ± 13 years (range 18–65 years). Fifty-five percent patients had a body mass index (BMI) of <25. The mean operative duration of patients in our study was 43 ± 12 minutes. Thus, an uncomplicated LC usually took less than an hour.
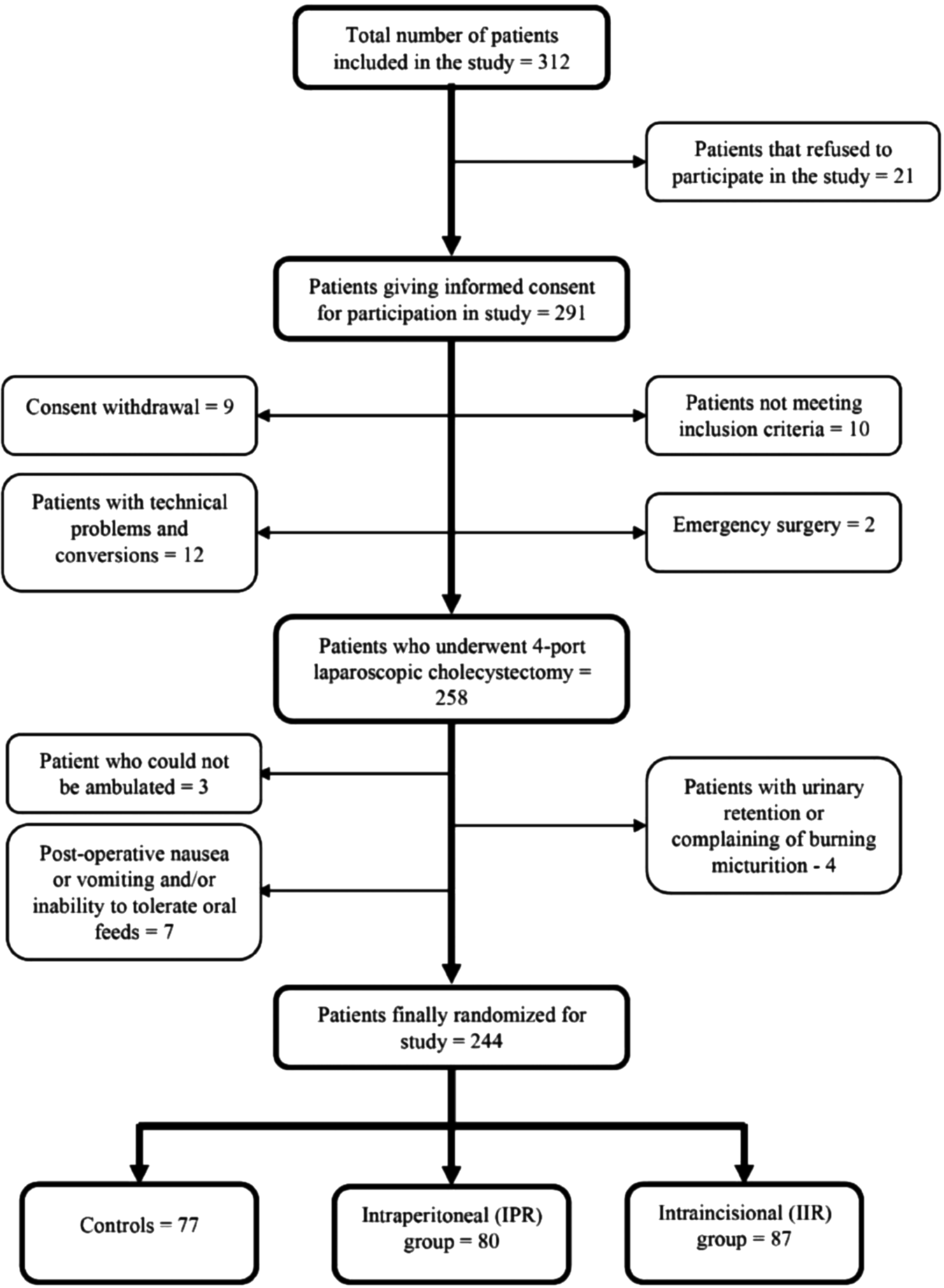
Flowchart of study design for inclusion of patients.
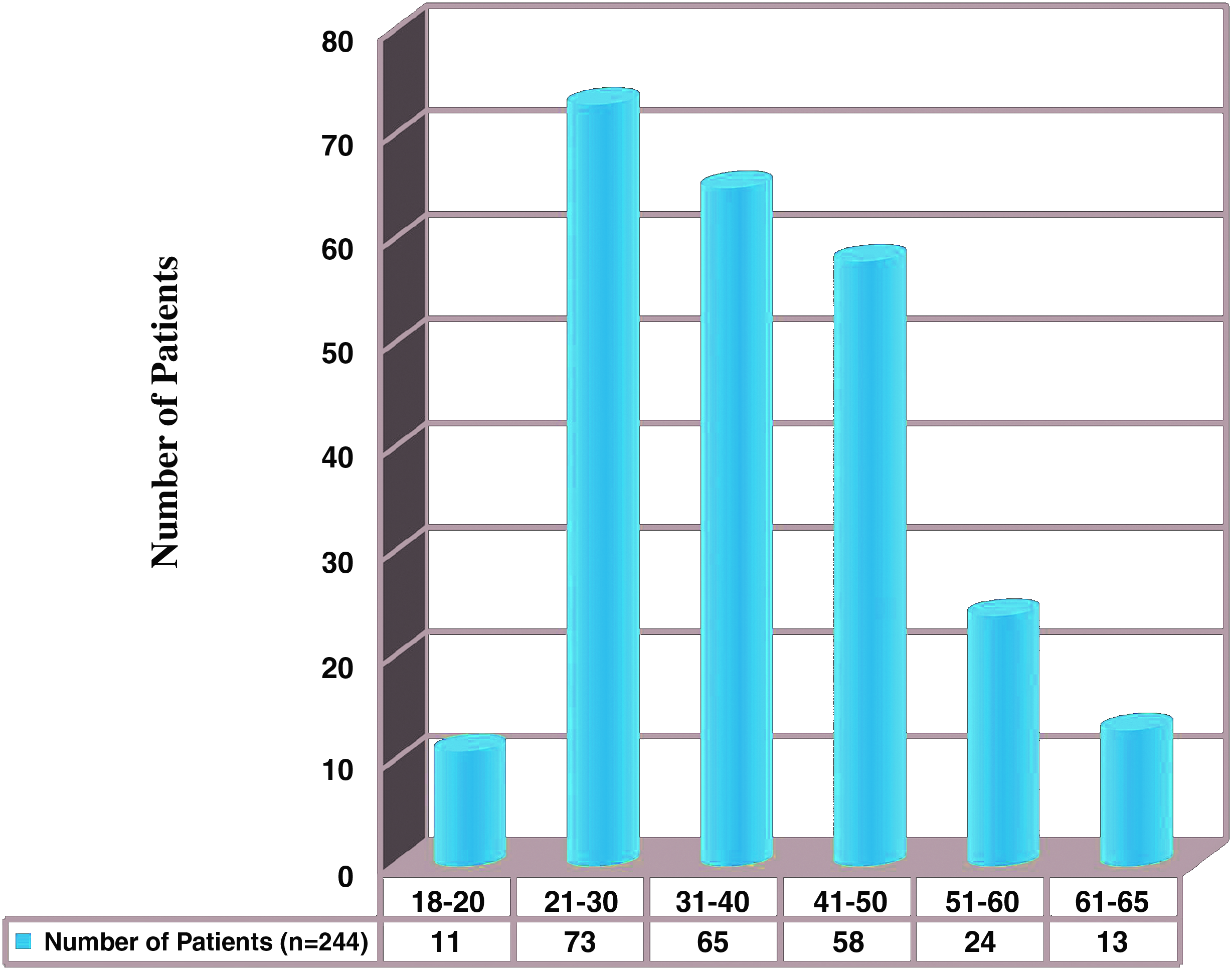
Distribution of patients by age groups.
Study groups: distribution of patients by the location of drug use
Since this was a randomized triple-blind study in which the envelope method was used as a means of randomization, the unequal size of groups is purely on chance basis and, hence, contributes to normal Gaussian distribution of patients. The number of patients, after opening envelopes, in the three study groups was found to be—controls with 77 patients, IPR with 80 patients, and IIR with 87 patients (Fig. 4). The three study groups were age, BMI, and operative duration matched, that is, there was no significant difference among the three study groups in terms of the earlier mentioned parameters (P > .05, as calculated from ANOVA and Tukey's Post hoc analysis).
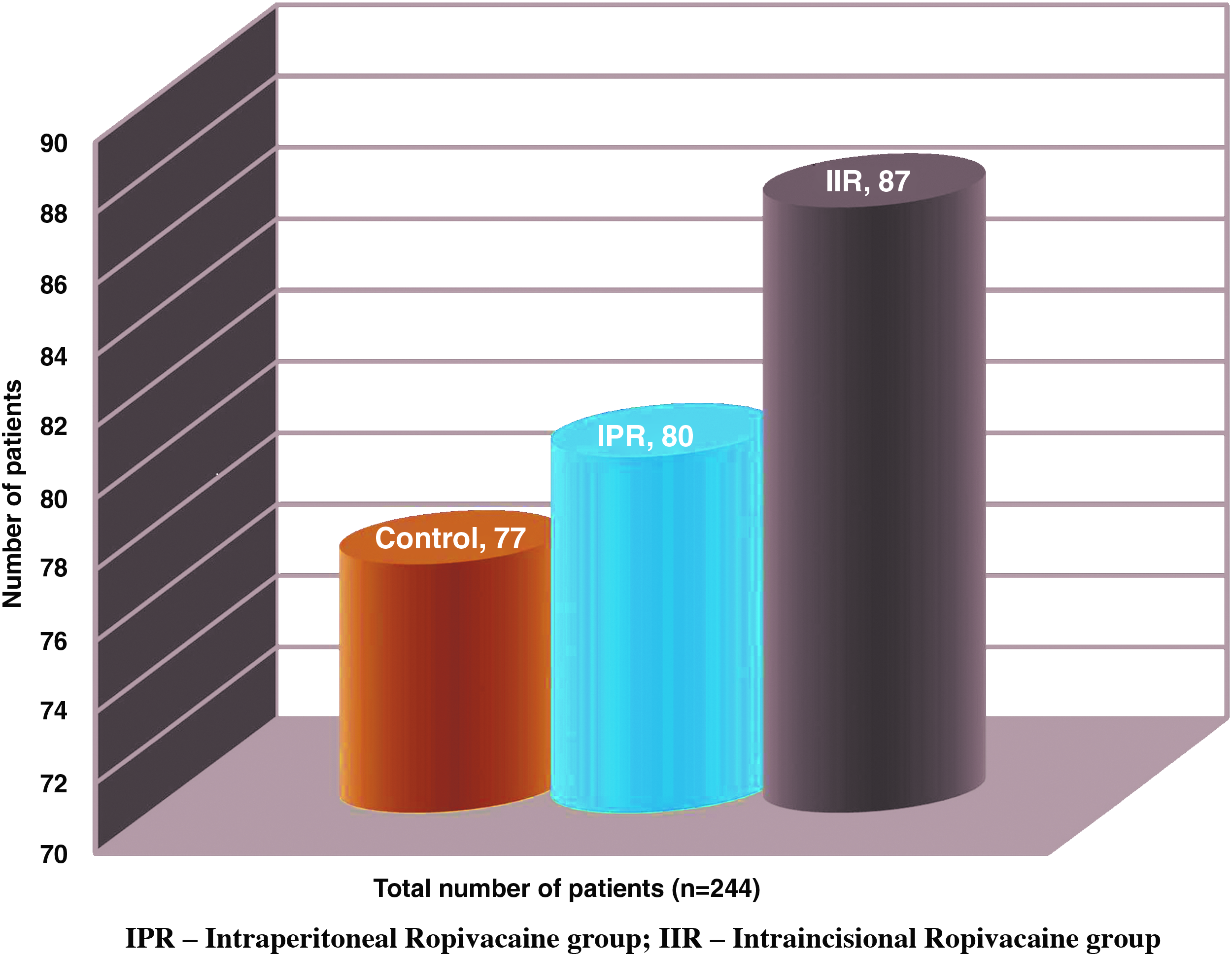
Distribution of patients by the location of drug use, that is, the study groups.
Postoperative pain evaluation
Shoulder pain
The incidence of shoulder pain in our study was 17.6%, that is, a total of 43 patients experienced shoulder pain in the three study groups (controls—23; IPR—7; IIR—13). The distribution of patients with shoulder pain by study groups is shown in Figure 5. As we can see from Figure 5, 42.6% of controls complained of right shoulder pain as against 17.6% in the IIR group and 9.6% in the IPR group (P < .05). So FET was applied between an individual pair of study groups to check the significance of association of shoulder pain. A P value <.05 indicated significant control of shoulder pain with intraperitoneal instillation of drug as compared with controls; and also as compared with its intraincisional infiltration. However, a P value of >.05 was obtained when the IIR group was compared with controls, indicating an insignificant difference in the perception of shoulder pain between these two groups.

Distribution of patients by study groups with regards to shoulder pain.
Out of the 43 patients with shoulder pain, 36 (83.7%) experienced it before the 12th postoperative hour. Among these 36 patients, 15 (41.7%) developed shoulder pain between the 0.5th and 4th hour, meaning that this was the most frequent time when shoulder pain arose. The order of frequency of postoperative shoulder pain appearance was: 0.5th to 4th hour (15) > 4th to 8th hour (9) > 8th to 12th hour (7) = 12th to 24th hour (7) > immediate postoperative period (5). Shoulder pain then reached a peak within 2–4 hours in most patients and then gradually tapered off over the next 12–24 hours. Thus, in 19 patients (44.2%), the timing of peak incidence of pain was between the fourth and eighth hour, implying that this was the most common time for shoulder pain, when present, to being at maximal intensity.
Shoulder pain was severe in 11 (25.6%) (6 controls, 1 IPR, and 4 IIR) patients, and these patients demanded for RA. Three (2 in controls and 1 in IIR) of these patients complained that their shoulder pain was even more severe than the abdominal pain. Two patients complained of severe shoulder pain in the night leading to disturbed sleep. Further, only 5 patients had some form of shoulder pain remaining after the 24th postoperative hour. Thus, among the nondischargeable patients (by “Discharge Criteria” given in Table 1) at the 24th hour, 113 patients were nondischargeable, and the contribution of shoulder pain was 9.7% (11 patients).
ATS, Activity Tolerance Scale; CBI, Can Be Ignored; CBRR, Complete Bed Rest Required; EP, Extreme Pain; FPS-R, Faces Pain Scale-Revised; IIR, intraincisional ropivacaine group; IPR, intraperitoneal ropivacaine group; IWBN, Interferes With Basic Needs; IWC, Interferes With Concentration; IWT, Interferes With Task; MIPI, The Most Intense Pain Imaginable; MLP, Mild Pain; MP, Moderate Pain; NP, No Pain; NRS, Numeric Rating Scale; SLP, Slight Pain; SP, Severe Pain; VAS, Visual Analog Scale; VDS, Visual Descriptive Score.
The observations mentioned earlier made us to come to the conclusions that shoulder pain is effectively taken care by peritoneal instillation of drug and it is not a very important source of pain as it only affected discharge of 4.5% (11/244) of patients and in only 1 patient in the IPR group it would have led to delayed discharge. Moreover, we found no significant role of incisional infiltration of LA in combating shoulder pain. However, since it became prominent most commonly around the eighth postoperative hour and some patients might experience it in the night, we included it as part of our “Discharge Criteria” so that we do not underestimate the pain experience of any patient.
Use of RA
A total of 49 (20.1%) patients required RA in our study in the three study groups (controls—26; IPR—15; IIR—8). Among the patients, the requirement of RA is distributed as shown in Figure 6. An FET was applied (3 × 2 contingency table) to see whether the usage of RA was significantly high. A P value of <.05 was obtained, which was significant. FET was also applied to individual groups to check what groups of associations were significant. For control versus IIR (2 × 2 contingency table), a P value of <.05 was obtained, thus depicting that the usage of RA was significantly less in the IIR group as compared with controls. However, for control versus IPR, and IIR versus IPR groups, the two-tailed P value from FET was found to be >.05, which meant that there was no significant difference in the usage of RA in these comparative groups. This observation implied that incisional infiltration of LA is significantly more important in reducing the requirement of RA than the peritoneal instillation; and incisional component of pain is more prominent in the initial period.
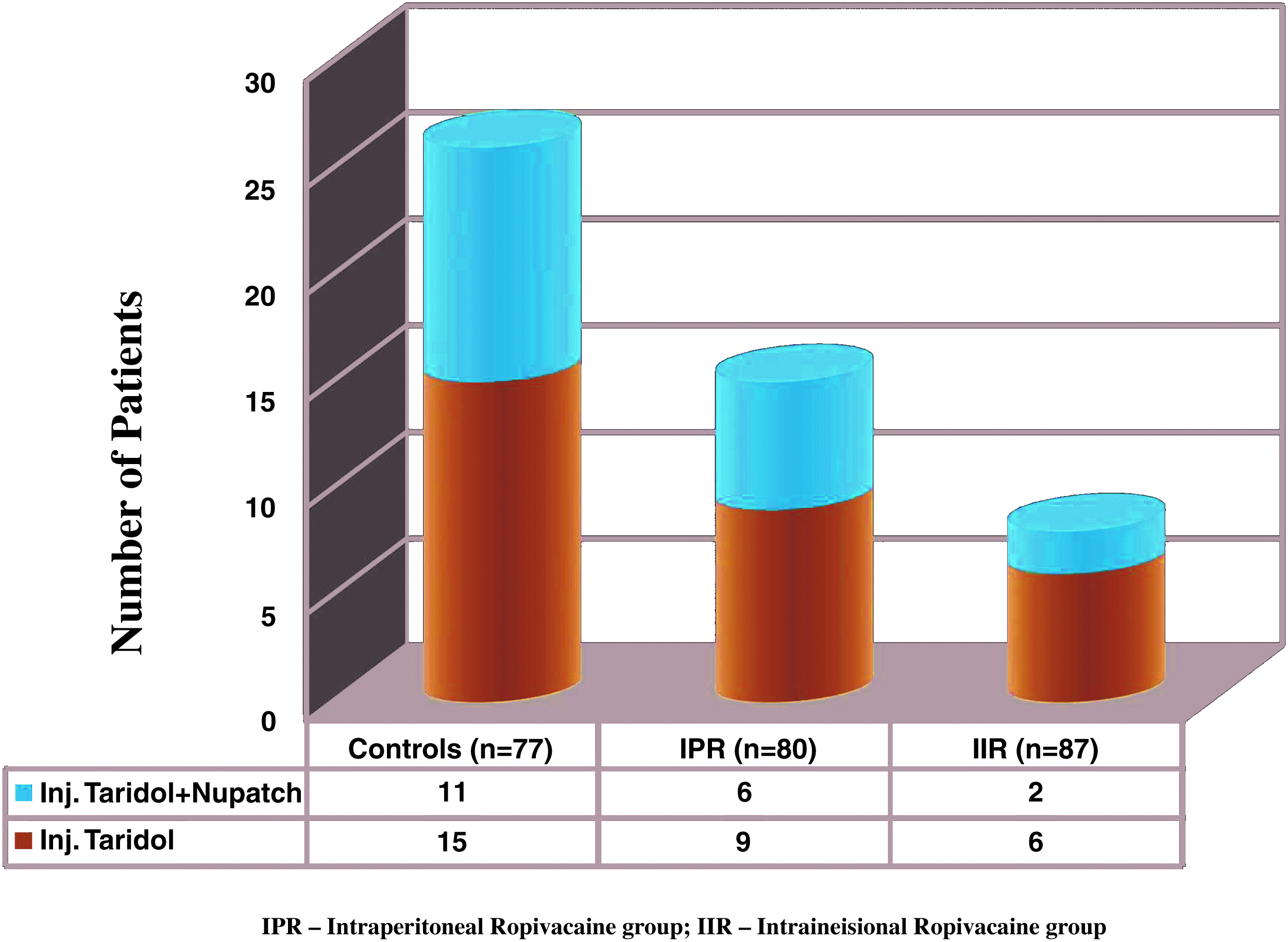
Distribution of patients by study groups with regards to the usage of rescue analgesia.
We have taken the requirement of RA by a patient as an indicator of severe pain, and, hence, none of these patients was considered to be given discharge. Nineteen patients (38.8%) further required dermal analgesic patch application for additional pain relief. In the remaining 30 patients, pain then reduced proportionately as was the trend in that particular group but still remained at relatively higher levels as compared with other patients in that group. If we subtract the patients of severe shoulder pain who required RA, that is, 11 patients, then we can infer that 38 out of 113 nondischargeable patients (33.6%) were not discharged due to the use of RA.
Since patients receiving RA might have an additional requirement of analgesics, their pain scores are at relatively higher levels as compared with similar patients in their respective groups, and they contribute to a significant number of nondischargeable patients, we have included it as part of our “Discharge Criteria.”
Pain assessment using pain scores
Pain assessment was done at five points of time by using five different pain scales; some of them measured pain objectively, and others measured it subjectively. Table 1 is the master table for different pain scores. For the numeric scales of VAS and NRS, mean scores of pain are given in the table at different time intervals. However, for categorical data of VDS, FPS-R, and ATS scales, the number of patients in individual grades of pain has been mentioned in the table. There was a reduction of pain on consecutive measurement of pain scores at 4-hourly intervals even in controls, thereby meaning that with passage of time pain spontaneously decreases.
Table 2 shows the significance of pain reduction at five points of time by using the five pain scales in the three comparative study groups. One hundred percent patients when offered discharge were found to be willing to go home while using the “Discharge Criteria” that is, “VAS ≤3, NRS ≤3, VDS ≤“SLP,” FPS-R ≤2, ATS ≤“CBI,” no rescue analgesia requirement and no shoulder pain.” However, it may be cumbersome to use all these pain scales simultaneously for predicting discharge. So, we made Table 3 to check which single pain scale was the most valid to predict the discharge rate so that when used with absence of shoulder pain and absence of use of RA, it can be used to predict the discharge of patients.
IIR, intraincisional ropivacaine group; IPR, intraperitoneal ropivacaine group; NRS, Numeric Rating Scale; VAS, Visual Analog Scale.
ATS, Activity Tolerance Scale; CBI, Can Be Ignored; IIR, intraincisional ropivacaine group; IPR, intraperitoneal ropivacaine group; NRS, Numeric Rating Scale; SLP, Slight Pain; VAS, Visual Analog Scale; VDS, Visual Descriptor Scale.
Table 3 shows the percentage overestimation of number of patients eligible for discharge from the “Discharge Criteria” proposed in the Methodology section. Some important inferences can be drawn from Tables 1 to 3. The following inferences are based on the assumption that the amount of drug used at both sides is comparable, the rate of absorption of the drug is similar at two sites, and the effect of the drug starts to wear off in a similar manner at different locations; these seem to be logical assumptions under the given circumstances. The inferences include:
1. The numeric pain scales that are considered better for pain evaluation agree in their findings that, indeed, there is a significant reduction in pain with the use of IIR as compared with the other two groups, at all points of time, as can be seen in Table 2. So, intraincisional infiltration of the drug is desirable. Moreover, the two scales agree to the fact there is significant pain reduction in the intraperitoneal group as compared with controls at all points of time except at the 24th hour where the two scales disagree. Considering the fact that IPR groups produce a moderate amount of analgesia as compared with its infiltration, this might be true that there might not be actually any significant difference in pain perception in the two groups. However, two other scores (VDS, FPS-R) show a significant difference, so we conclude that intraperitoneal infiltration of ropivacaine causes a significant reduction of pain, even at the 24th hour as compared with controls. 2. The three categorical data-based scales (VDS, FPS-R, and ATS) agree that at 0.5 hours there is no significant difference in pain reduction between the IPR and IIR groups. This can actually be either due to delay in the onset of action of the drug or due to the fact that the investigator under-rates the patients' experience of pain. 3. Subjective pain scales should ideally guide us in deciding to discharge a post-LC patient because they tell us about the patients' own perception of pain. We also corroborate the earlier statement by our study as the percentage overestimation by using our “Discharge Criteria” in Table 3 was found to be the least while using subjective pain scales, particularly the numeric pain scale, that is, VAS and NRS. Among the subjective pain scales, numeric pain scales (VAS and NRS) seem to have more validity than the categorical scale of VDS. When VAS or NRS was used along with no shoulder pain and no use of RA as a criterion for predicting discharge, it corroborated 94% with the “Standard Criteria,” which is within the margin of error. The VDS score corroborated 90%, FPS-R 86% whereas the ATS score only corroborated in 73% cases along with no shoulder pain and no RA, with the number of patients capable of being discharged as compared with “Standard Criteria.” 4. The investigator according to the ATS score seems to misinterpret patients' feelings toward pain, and, thus, significantly more patients are eligible for discharge by using the criteria ATS ≤“CBI” alone as compared with the standard set criteria of all pain score cutoffs+no shoulder pain+no use of RA (“Discharge Criteria”). The same appears to be partly true for the other objective pain scale, that is, FPS-R. 5. At the 12th postoperative hour, the number of patients willing to go home in controls as compared with the IPR group is not significantly high (FET two-tailed P value .09; P > .05) by the “Discharge Criteria.” This insignificant difference tells us that the visceral component of pain that has been tackled by intraperitoneal instillation of ropivacaine in the IPR group, though accounting for some pain, is not predominant in the first 12 hours. 6. At the 12th postoperative hour, the number of patients willing to go home in the IIR as compared with the control group is significantly high (P < .05) by our “Discharge Criteria.” This significant difference tells us that the incisional component of pain is the predominant component in the first 12 hours as the incisional infiltration of ropivacaine has taken care of the incisional component in the IIR group, leading to this significant difference. 7. At the 12th postoperative hour, the number of patients in the IIR as compared with the IPR group is significantly higher (P < .05) according to “Discharge Criteria.” This significant difference tells us that the incisional component of pain is significantly a greater contributor to the pain of patients up to the first 12 hours. 8. In the IPR group, the number of patients willing to go home at the 12th hour and at the 24th hour is significantly high (P < .05) by “Discharge Criteria.” This can only be explained by the fact that either the incisional component of pain is not the predominant component of pain after the 12th postoperative hour or the action of the drug at the intraperitoneal location is longer as compared with at the intraincisional location. Since the absorption of the drug through surrounding capillaries is a rule and occurs at both sites, the latter fact does not seem to hold true. So, our inference is that the incisional component of pain is not the predominant component of pain after the 12th postoperative hour. 9. If we see the patients in the control group, then the number of patients at the 12th hour and at the 24th hour who are willing to go home is insignificant (P > .05). Based on the earlier assumption that incisional pain is not predominant after the 12th hour, it can be inferred that there is still a component of pain that is causing significant pain to the patient, that is, the visceral component. By corollary, we can say that the visceral component of pain is the predominant component of pain after the 12th hour. 10. However, if we compare the IIR group at the 12th hour with the IIR group at the 24th hour, then the number of patients willing to go home does not rise significantly (P > .05) as compared with “Discharge Criteria.” This signifies that some other cause of pain (visceral) is still prevailing, has taken predominance over the incisional component, and is holding the patients from going home. 11. At the 24th hour, the number of controls as compared with the IPR group who are willing to go home is significantly high (P < .05). This again signifies that desensitization of nociceptors caused by the drug at the intraperitoneal location is still causing significant pain relief and indicates the predominance of visceral pain at this time. 12. At the 24th hour, the number of patients willing for discharge in the IIR group is not significantly different as compared with the IPR group (P > .05), again thereby meaning that the visceral component of pain predominates over the incisional component at this time.
Discussion
LC has become a day care procedure in most parts of the world. 16 Day care surgery has been defined by the Royal College of Surgeons as when the surgical day case patient is admitted for investigation or operation on a planned nonresident basis and who nonetheless requires facilities for recovery. 16 Nowadays, many day units operate an “extended” or “23 hour” stay policy, which means that patients can stay in the unit up to 23 hours 59 minutes and still be categorized as a day case. 16 However, pain continues to be an important limiting factor in the early discharge of patients.8,17
Pain after LC is highly variable among patients.4,10 Pain intensity peaks during the first 4–8 postoperative hours and usually declines over the next 2–3 days. 18 Previous studies have suggested that pain after LC characteristically involves several pain components with different pathophysiologic mechanisms, intensity, and time course.10,19 This has been extensively studied by Schoeffler et al. 20 They report that surgical exploration is associated with tearing of blood vessels, traumatic traction of nerves in the skin and at the operative site. Pneumoperitoneum leads to additional distension of the peritoneum, which is quite sensitive to this rapid distension. This further leads to limited peritoneum inflammation. The presence of shoulder pain can be explained by the stretching of the diaphragm by the pneumoperitoneum thus created. This leads to an excitation of the phrenic nerve. 21 A peritoneal biopsy done 2–3 days after laparoscopy showed peritoneal inflammation and neuronal rupture, and there was a linear inverse relationship between abdominal compliance at the time of laparoscopy and the severity of postoperative pain. 22
The pain after LC can be considered to arise from three main sources: the incision sites; the pneumoperitoneum in association with both local (peritoneal and diaphragmatic stretching, ischemia, and acidosis) and systemic (hypercarbia causing sympathetic nervous system excitation resulting in amplification of the local tissue inflammatory response) changes; and the postcholecystectomy wound within the liver. Pain in LC is usually located at the incision site and is described as sharp piercing-type pain or in the (right) upper abdomen or a constant dull ache that the patient describes as to be coming from inside or the pain may be referred to the tip of the right shoulder. 22 There is minimal stretching of the left hemi-dome of the diaphragm, so it usually does not contribute to any pain. Initial sharp piercing pain at the operative site gradually wears off over time. Later on, the pain is described as a constant dull ache coming from the inside.8,22
In a study of 40 patients, Joris et al. 10 reported that visceral pain defined as deep intra-abdominal pain dominated over incisional and shoulder pain after LC. Joris demonstrated that visceral pain featured in the first 24 hours postoperatively, but was short-lived, whereas shoulder-tip pain was minor and featured on postoperative day 2. He further concluded that intraperitoneal bupivacaine was not effective for treating any type of pain after LC. Fu et al. 11 also found in their study that 81.7% of patients had visceral pain, 50% experienced parietal pain, and 26.7% reported shoulder pain after LC and they concluded that visceral pain is prominent after LC.
Bisgaard et al., 8 however, found that incisional pain dominated over visceral pain, which, in turn, dominated over shoulder pain. They divide total abdominal pain after LC as follows: largest component (50%–70%) arising from the incision sites, then the pneumoperitoneum (20%–30%), and, finally, cholecystectomy dissection (10%–20%). The finding that incisional pain dominated over other pain components in incidence and intensity in the first postoperative week is in accordance with findings in patients in whom LAs were not used (Bisgaard et al. 19 ; Ure et al. 5 ). Lee et al. 12 also reported the predominance of incisional pain for the first 2 days after LC. The findings of our study also corroborate with these studies that initially the pain is predominantly due to the skin incisions and manipulation done at parieties and it reduces rapidly in the first 12 hours and then reduces slowly; and the visceral pain decreases slowly as compared with incisional pain and is the predominant pain after the 12th postoperative hour.
Shoulder pain is reported to be a common complaint after laparoscopic surgery. Several causes of shoulder pain after laparoscopic surgery have been suggested: the effect of CO2 gas, 23 peritoneal stretching, diaphragmatic injury, diaphragmatic irritation, and even shoulder abduction during surgery. 24 The incidence varies, being reported by Lepner et al. and Sarli et al.25,26 approximately in one third of patients after LC. Joris et al. 10 demonstrated that shoulder-tip pain is minor and features on postoperative day 2. Sarli et al., 26 however, report that shoulder-tip pain starts at 3–6 hours postoperatively, peaks at 12 hours, and rapidly improves thereafter. Bisgaard et al. 8 report pain due to the pneumoperitoneum to constitute 20% to 30% of total pain. Shoulder pain is often mild in intensity and can remain for 24 hours or even longer in some cases. 27
In our study, we found a 17.6% incidence rate of shoulder pain and it most commonly appeared between the 0.5th and 4th postoperative hour, and most frequently peaked 2–4 hours later, that is, between the 4th and 8th hour. We further found that shoulder pain then reduced gradually and was almost absent in 90% of patients who initially experienced it, at the end of the 24th hour. Methods investigated to control it include: low-pressure insufflation, slow rate of insufflation, no CO2 insufflation, warmed gas, pre-emptive anti-inflammatory medication, pre-emptive diaphragmatic LA irrigation, postoperative sub-diaphragmatic suction, and regional anesthesia to peritoneal surfaces in the operative area. 28
Multiregional uses of LA, that is, both intraperitoneally and at the incision site, are found to be better than its use only at one site in most studies.29–34 However, some authors could not find any evidence that the combined approach is any way effective and they recommend use of the incisional approach only.12,19,35 Grecu et al. 31 used preincisional infiltration and intraperitoneal instillation of ropivacaine 0.25% combinedly and alone, and they found significant favorable effects on postoperative pain after LC only when using combined preincisional local infiltration and intraperitoneal instillation. Nicolau et al. 29 tested the effects of preincisional parietal and intraperitoneal infiltration with ropivacaine on postoperative pain after elective LC. They concluded that ropivacaine showed significant favorable effects on postoperative pain after LC when using both parietal and intraperitoneal instillation as compared with when used at one site alone.
Di Pace et al. 32 demonstrated that the combination of local infiltration and intraperitoneal instillation of ropivacaine was more effective for pain relief in children after laparoscopic surgery than the administration of ropivacaine only at the trocar sites. Cha et al. 34 again confirmed that peri-trocal infiltration of ropivacaine significantly decreased parietal pain and intraperitoneal instillation of ropivacaine significantly decreased visceral and shoulder-tip pain. Their effects were reported to be additive with respect to the total pain. At the end of our study, we also came to the conclusion that the effect of LA at intraincisional and intraperitoneal sites is additive, with the drug at both sites catering to different components of pain and, thus, both contributing significantly to overall pain control. Peritoneal instillation of drug effectively combats shoulder pain and, hence, is desirable along with its incisional use.
Finally, we formulated 100% fail-proof “Discharge Criteria” consisting of “VAS ≤3, NRS ≤3, VDS ≤ “SLP,” FPS-R ≤ 2, ATS ≤ “CBI,” no requirement of rescue analgesia and no shoulder pain,” which predicted the acceptance of discharge by patients accurately. Since, numeric subjective scales were found to corroborate with the earlier formula in 94% cases, the earlier criteria can be simplified to form the “Abbreviated Discharge Criteria” consisting of “Numeric subjective pain score (VAS or NRS) ≤3 with no requirement of rescue analgesia and no shoulder pain.” No such study was found during our literature review, which had used LA to predict the discharge of post-LC patients in an objective way and, thus, suggests the uniqueness of the current discussion.
Conclusion
The effect of LA at intraincisional and intraperitoneal sites is additive, with the drug at both sites catering to different components of pain and, thus, both contributing significantly to overall pain control. The use of a numeric pain score with score ≤3 along with the absence of use of RA and the absence of shoulder pain can effectively predict the discharge of a patient (“Abbreviated Discharge Criteria”). This study is unique as this is the first study in which only a local anesthetic has been used to make a model to predict the early discharge of patients. We recommend using the earlier mentioned criteria routinely in practice to check for patients' acceptance to go home at any point of time postoperatively in a nondiscriminatory unbiased empirical manner, when pain is the main complaint postoperatively.
Footnotes
Acknowledgment
The authors are grateful to Professor Ramesh C. Goel, Department of Statistics, PGIMER Chandigarh, for helping in conducting the statistical analysis.
Disclosure Statement
No competing financial interests exist.