
Abstract
Abstract
Background:
Continuous efforts to reduce the numbers and size of incisions led to the emergence of a new technique, single-incision laparoscopic surgery (SILS). It has been rapidly accepted as the preferred surgical approach in the colorectal area. In the age of SILS, what is the role of hand-assisted laparoscopic surgery (HALS)? We introduce the way to take advantage of it, as an effective alternative to avoid open conversion.
Methods:
This is a retrospective review of prospectively collected data of SILS colectomies performed by a single surgeon in Samsung Medical Center between August 2009 and December 2012.
Results:
Out of 631 cases of SILS colectomy, 47 cases needed some changes from the initial approach. Among these, five cases were converted to HALS. Four of them were completed successfully without the need for open conversion. One patient with rectosigmoid colon cancer invading bladder was finally opened to avoid vesical trigone injury. The mean operation time of the 4 patients was 265.0 minutes. The mean estimated blood loss was 587.5 mL. The postoperative complication rate associated with the operation was 25%.
Conclusions:
Conversion from SILS to HALS in colorectal surgery was feasible and effective. It seemed to add minimal morbidity while preserving advantages of minimally invasive surgery. It could be considered an alternative to open conversion in cases of SILS, especially when the conversion to conventional laparoscopy does not seem to be helpful.
Introduction
L
Conversion is a major concern in laparoscopic surgery, and it has been noted to be associated with adverse short-term and long-term outcomes.1,13,14 In conventional multiport laparoscopy, conversion generally means switching the procedure to traditional open laparotomy. In SILS, there are more options for conversion: SILS can be converted to conventional multiport laparoscopy or directly to open laparotomy. However, conversion to HALS in colorectal laparoscopy, which has been described in a few articles as an effective transit option,15,16 was rarely highlighted in publications separately. When a decision is made to convert from SILS or conventional multiport laparoscopy, HALS might be a safer and potentially more advantageous alternative compared with conversion to open laparotomy.
In this article, we introduce our technique and result in five cases of colorectal procedure involving conversion from SILS to HALS.
Materials and Methods
The data of all patients who underwent SILS in Samsung Medical Center have been collected prospectively in the SMC SILS database. Out of them, all cases of SILS colectomy for benign or malignant disease, performed by a single surgeon between August 2009 and December 2012, were reviewed. Patient demographics, indications for surgery, operative details including operation time, estimated blood loss (EBL), conversion from the planned surgery, and perioperative complications were evaluated. In each case, the operative records were reviewed and the reason for conversion was determined.
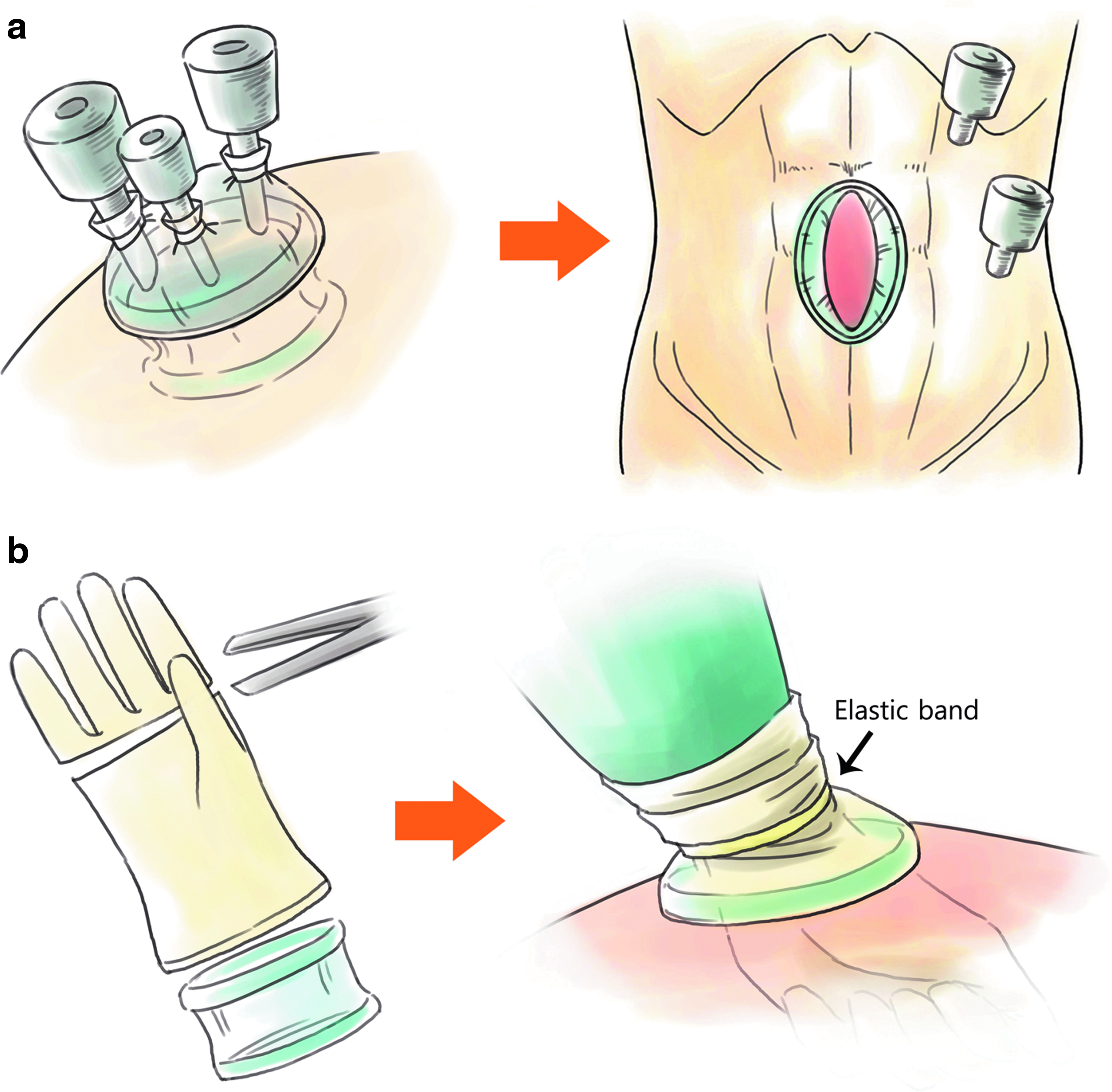
For SILS colectomy, we mainly used a custom-made glove port and conventional straight instruments. The port was made up of a powder-free surgical glove, three or four trocars, and a wound protector. A detailed description of SILS technique is beyond the scope of this article, and details of the procedure have been reported in our previous reports. 17
Any changes to the incision or insertion of an additional trocar were considered as a conversion, except for extension of the SILS port site for extraction of a bulky specimen. One additional trocar for low anterior resection (LAR) or abdominoperineal resection was not counted as a conversion, because we always considered SILS plus one additional trocar as a second-string procedure during SILS LAR because of its special complexity and difficulty on distal division with insufficient angled stapler and proper total mesorectal excision.
HALS was performed with a custom-made glove hand port or GelPort® Laparoscopic System (Applied Medical, Rancho Santa Margarita, CA). Conversion was completed by lengthening the SILS port incision, initially 3.5 to 4 cm, to a 7 cm in-length hand port incision. The hand port was placed in this incision, and the camera was moved to the 12-mm trocar. We disassembled the custom-made glove port for SILS and used each trocar for the camera and instruments (Fig. 1).
Results
A total of 631 SILS colectomies were performed by a single surgeon within the study period. Among them, 611 (96.8%) involved colectomy for colorectal malignancy or a premalignant condition and the other 20 (13.2%) for benign diseases, including diverticulitis or inflammatory bowel disease. The indications of surgery, type of operation, American Society of Anesthesiologists Score, body mass index, EBL, time to bowel function recovery, postoperative hospital stay, and complications are presented in Table 1.
Including 41 patients who underwent simultaneous procedure on different site of the colon or other organs.
Including 107 cases of single-incision laparoscopic LAR (or abdominoperineal resection) plus one trocar.
Including a case that was initially converted to hand-assisted technique.
ASA, American Society of Anesthesiologists; BMI, body mass index; EBL, estimated blood loss.
Forty-seven cases needed some changes from the initial approach. We converted from SILS to a hand-assisted procedure in 5 patients. Of these five cases, four were completed successfully with HALS. One needed open conversion to complete the operation. Perioperative variables for each patient are outlined in Table 2. More detailed characteristics and clinical course of the patients are described later.
AR, anterior resection; ASA, American Society of Anesthesiologists; BMI, body mass index; EBL, estimated blood loss; HALS, hand-assisted laparoscopic surgery; LAR, low anterior resection; RH, right hemicolectomy.
Case 1
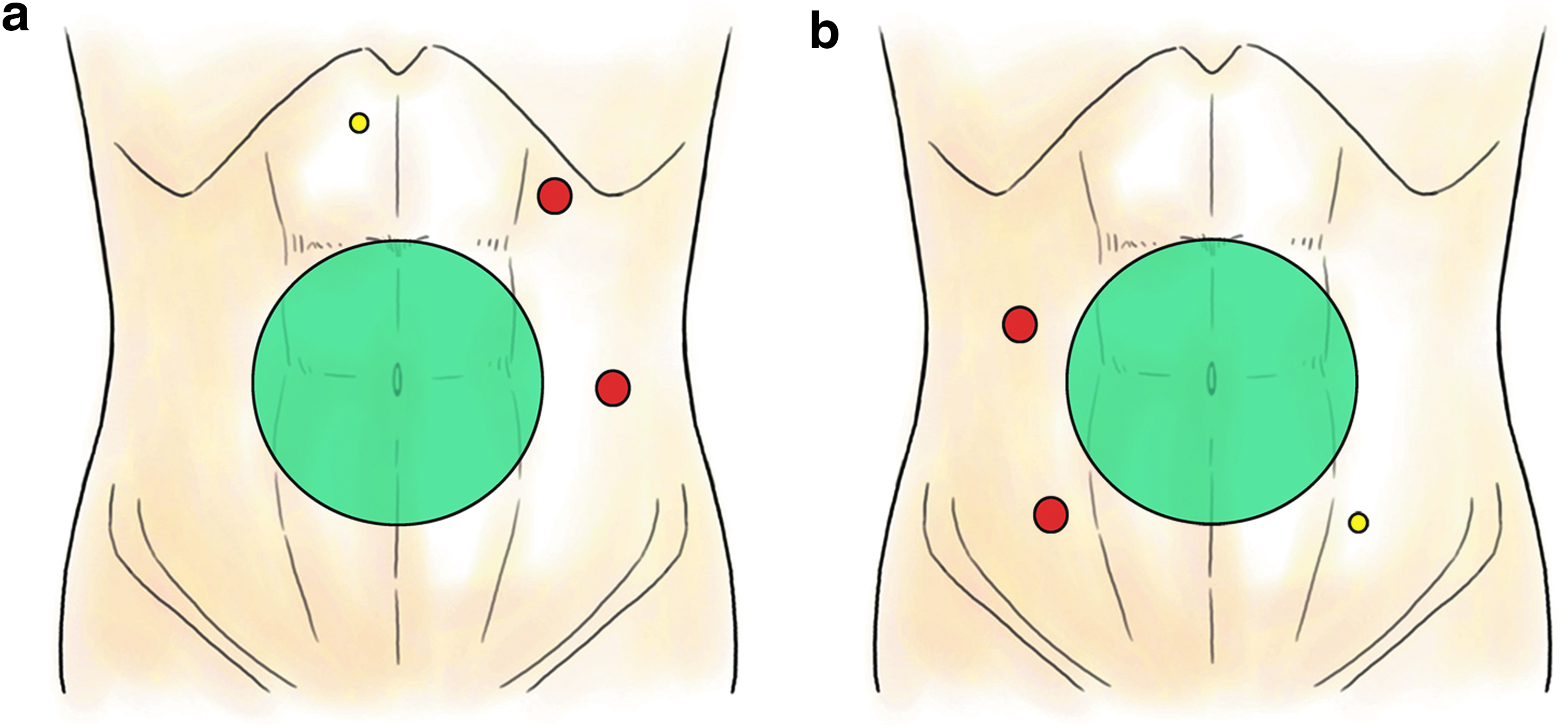
Patient 1 was a 51-year-old man who presented with a history of diverticulitis. Colonoscopy showed diverticulosis in the cecum and proximal ascending colon. The last attack was about 2 months before surgery. Although he had no symptoms or signs of acute inflammation at the time of operation, his right colon was so badly inflamed that we could not dissect through the exact plane and it was impossible to locate the right ureter. We decided to apply the HALS technique to prevent injury to the ureter. A 4-cm transumbilical incision initially made for SILS was extended to 7 cm, and the surgeon's left hand was inserted through a custom-made glove port. Two 12-mm trocars from the disassembled SILS port were inserted in the left subcostal area for a camera, and in the left middle abdomen for an instrument (Fig. 2a). The inserted hand helped to find the ureter and to progress with the careful dissection assisted with the tactile feedback in the most inflamed area. The patient recovered without complications and was discharged on the sixth postoperative day.
Case 2
Patient 2 was a 69-year-old man with a 3.5-cm cecal cancer and a 2-cm ascending colon polyp. The initial plan was for a right hemicolectomy using SILS. This patient was diagnosed with a duodenal ulcer and treated with oral medication about 40 years before surgery. The middle portion of the ascending colon and proximal jejunum adhered firmly to the second portion of the duodenum. We could not proceed with a safe dissection, and conversion was made to HALS. A custom-made hand glove port was used, and the trocars were located in a similar position to Case 1. A 5-mm trocar was added to provide traction in the epigastric area. The ascending colon was separated successfully. The proximal jejunum was divided from the duodenum, however, with a small injury on its wall. Although this penetrated the whole layer of the bowel, it was very small and we could repair it with a single interrupted suture. The patient recovered without complications and was discharged on the fifth postoperative day.
Case 3
Patient 3 was a 67-year-old man with a 2.5-cm cancer on his sigmoid colon. A SILS anterior resection was planned. The patient had suffered from alcoholic liver cirrhosis for a long time. Although the preoperatively calculated Child-Pugh classification was grade A, there was massive venous bleeding that could not be controlled easily. Moreover, the mesocolon was so edematous and thickened that we could not identify the vessels in it. During dissection of the inferior mesenteric vein, we encountered diffuse bloody oozing from the cut surface of the mesocolon. This was not controlled with monopolar coagulation or a more advanced energy device, and clipping was revealed to be useless. Therefore, conversion to HALS was made. A custom-made hand port was used, and two trocars were inserted in the right upper and lower abdomen (Fig. 2b). The bleeding mesocolon was compressed with the surgeon's left hand, and monopolar coagulation was applied. After this, the amount of bleeding was significantly reduced and the operation was safely completed. The patient developed uncontrolled ascites in the early postoperative period, which seemed to be associated with underlying liver cirrhosis. He was discharged on the 15th postoperative day without operation-related complications, after management with oral diuretics.
Case 4
Patient 4 was a 48-year-old man with advanced rectosigmoid junction cancer. We planned curative LAR. The cancer was considered to be invading the bladder dome and both ureters abutted onto it. Conversion to HALS using a GelPort was performed for safe dissection, and the right ureter was successfully divided from the cancer. Two trocars were used for a camera and instrument, and partial cystectomy progressed from the right to the left side. However, the left ureter and its insertion into the bladder at the trigone seemed to be very close to the cancer. We decided to change to an open surgical procedure. After en bloc LAR and removal of the invaded bladder wall, a urologist examined the trigone. It was not directly injured, but the defect of the bladder wall was very close to it and it was possible that it would be sutured and obstructed during bladder wall repair. After insertion of a double-J ureteral stent, the urologist repaired the bladder. The patient developed a deep surgical site infection at the wound site, which needed repeated dressing and repair under general anesthesia. He was discharged on the 31st postoperative day.
Case 5
Patient 5 was a 53-year-old man with advanced upper rectal cancer. He also had a chronic hepatitis B virus infection and liver cirrhosis; Child-Pugh classification grade A. Our initial plan was SILS LAR with one additional 12 mm trocar for distal division in the right lower quadrant. The cancer had infiltrated onto the perirectal tissue, especially to the left side. The tissue was stony hard, and dissection failed to progress. Conversion was made to HALS with a GelPort and three additional trocars. Two trocars were located in a similar position as in Case 2, and a 5-mm trocar was inserted in the left lower abdomen. After mesorectal excision and distal division, additional resection of the left lateral pelvic wall was performed. Soft tissue beyond the “holy plane” was completely resected. Pathology reports revealed cancer in this specimen. The patient suffered from postoperative ileus and wound infection, which improved after conservative management. He was discharged on the 34th postoperative day.
Discussion
HALS, a hybrid form of open and laparoscopic surgery, was initially introduced in answer to the question: Is there a way to offer patients the perioperative advantages of minimally invasive surgery (MIS) without the technical difficulty and increased time associated with conventional laparoscopy? It has carried out its expected role well for about 10 years with the addition of tactile feedback to standard laparoscopy. However, it needs an incision up to 6 to 8 cm for one hand and two or more incisions for the camera and instruments. On the other hand, as the techniques and technologies of laparoscopy advances, surgeons have become familiar with a laparoscopic technique and confident in performing it. Many surgeons have now completed their own learning curve and believe that they can do well enough, without the assistance of their hands. If so, is HALS now obsolete?
A gap still remains between conventional laparoscopy and open surgery in the ability of the surgeon to control the surgical field. This fact is underscored by the occasional need for conversion to an open laparotomy during laparoscopic procedures. Although the advancement in instruments and experience has narrowed the gap to an unidentifiable level in ordinary conditions, it becomes wider in some situations, in which HALS offers an exclusive benefit.
The common reasons for conversion are injury to adjacent organs, bleeding, unclear anatomy, failure to progress, adhesions, and/or oncologic concerns.13,16,18 With these problems, conversion should be viewed as a wise decision to avoid risking the patient's safety. It is not a complication in itself but just a limit that has been reached in the feasibility of the original procedure. However, it has been noted that conversion cases are associated with longer operative time, prolonged hospitalization, higher incidence of postoperative complications, and poorer long-term oncologic outcome.13,14,18,19 Conversion to open laparotomy seems to circumvent the postoperative advantages of laparoscopic surgery. Moreover, there exist several literatures reporting poorer postoperative outcomes of converted cases compared with classic open laparotomy. 20 These problems might be influenced by the nature of the disease, such as advanced stage or unresolved chronic inflammatory condition, which are strongly associated with the reasons for conversion. They might be consequences of the intraoperative complications that caused conversion. In either case, it is an obviously disappointing event for both surgeon and patient.
Conversion rates in randomized controlled trials comparing conventional laparoscopic with open colectomy ranged from 14% to 20%. 1 In SILS, the conversion rate to multiport laparoscopy in various colectomy series ranged from 0% to 20% and that to open laparotomy ranged from 0% to 5%. 12 These reduced conversion rates to open laparotomy might have been associated with the highly selected study populations in the early phase of SILS and/or the advancement of laparoscopic techniques during the time gap between the conventional laparoscopic and SILS studies. In this study, the rate of conversion to multiport laparoscopy was 5.1% (when including 107 cases of “SILS LAR with one additional trocar,” it was 22.0%). The conversion rate to open laparotomy was 1.4%.
In SILS, most surgeons would think that the first choice of conversion is conventional multiport laparoscopy with the addition of one or two trocars. However, having gained much experience, we came to the conclusion that the technical difficulty of SILS was generally similar to that of conventional multiport laparoscopy, especially as regards understanding how triangulation of SILS works in a different way. The exception to this finding was left-side colectomy, including dissection and distal division under the pelvic promontory. For these cases, we frequently needed one or more trocars for safe dissection and distal division. All 32 patients who experienced conversion to multiport laparoscopy in this study needed additional trocars for this reason. That is why we excluded “SILS LAR with one additional trocar” cases from our count of conversion. We have described this in another manuscript in detail.
When we were unable to progress with one or two more trocars, conversion to open laparotomy seemed to be inevitable. We did not consider HALS as a conversion option in the early days of SILS. After several experiences of conversion, we started to find ways to avoid open laparotomy. In addition to returning to the use of tactile sensation via the surgeon's hand, HALS allows manual vascular control, safe traction of inflamed or edematous tissues, and blunt dissection with minimal injury, without relinquishing perioperative advantages of MIS.15,21–23 These were almost all and even more of the advantages we expected from conversion.
In this study, we have reported five cases of HALS colectomy that were converted from SILS. The indications for conversion were thick adhesion to adjacent structures caused by previous inflammation in 2 patients, excessive tumor fixit in 2 patients, and uncontrolled bleeding in another 1 patient. Four of them were completed without the need for open conversion, and another 1 finally went to open laparotomy because of concern over vesical trigone injury. The postoperative complication rate in the completed with HALS cases was 50% (2/4). This is higher than that of the SILS completion group (17.6%, 103/586) and of the multiport conversion group (19%, 6/32), but lower than that of the open conversion group (67%, 6/9) (Table 3). Moreover, in patient 3, who suffered from uncontrolled ascites, the direct cause of complication was his underlying liver cirrhosis, not the operation itself. The patient's bowel function recovered rapidly on the second postoperative day, and his general performance was good. Therefore, we consider that the advantages of MIS were maintained in this patient.
HALS hand-assisted laparoscopic surgery; SILS, single-incision laparoscopic surgery.
Although HALS might not present a high-end option as a primary surgical approach, it could provide great benefit in conversion from difficult and complicated laparoscopic cases, before resorting to open surgery. When a decision is made to convert from SILS, conversion to HALS may be a feasible, safe, and potentially more advantageous alternative compared with conversion to open surgery. In an age of more advanced and complex laparoscopy, HALS will survive with this exclusive value.
Footnotes
Disclosure Statement
No competing financial interests exist.