
Abstract
Abstract
Background:
Laparoscopic cholecystectomy (LC) is commonly performed in patients who can pose technical challenges, such as obesity, prior surgery, and subsequent incisional hernias. A new technique, the subcostal trocar approach using four 5-mm with exclusive removal (STAUFFER) LC, was developed to diminish these impediments and is highly advantageous.
Methods:
A retrospective review was performed of medical records for 389 patients who underwent LC from June 2011 through December 2016. STAUFFER LC involves (1) steep patient positioning, (2) visualized 5-mm trocar entry in the right abdomen, (3) use of three additional right subcostal trocars, and (4) gallbladder extraction from the high right lateral trocar site. Patient characteristics, operative details, and outcomes were analyzed and compared.
Results:
STAUFFER LC was used in 255 patients (65.6%), and standard four-trocar LC (SLC) was performed in 134 patients (34.4%). Overall indications for surgery included chronic cholecystitis (71.7%), acute cholecystitis (19.8%), polyp (2.3%), and other (5.9%). No significant differences were detected in comorbidities and American Society of Anesthesiologists classification between the two patient groups. More patients in the STAUFFER LC group had previous midline abdominal surgery (P = .06) and significantly higher body mass index (P = .03), and they required less operative time (P < .001). No patient had an entry site injury. No significant difference was noted in morbidity. One patient required a second laparoscopic operation for bleeding. One patient with Crohn's disease and “hostile abdomen” had an enterocutaneous fistula that closed spontaneously. In the SLC group, trocar site hernia (TSH) developed in 3 patients.
Conclusions:
STAUFFER LC is widely applicable and effective, saving operative time and reducing the risk of TSH. It is especially advantageous for obese patients who have had previous surgery.
Introduction
L
As surgeons have gained experience, LC has undergone many refinements, including the use of fewer and smaller trocars.1,5–9 The safety of LC has improved with standardization and the inclusion of common central elements in each technique for minimizing the number of complications, particularly bile duct injuries. 10 Like other surgical procedures, gallbladder surgery is still developing, and techniques and protocols are focused on decreasing complications, length of stay, size of incisions, consecutive pain, and subsequent long-term complications, such as incisional hernia. 11 Montz et al. 12 reported that trocar site hernia (TSH) can be a serious complication after laparoscopic interventions and highlighted that most TSHs developed in the umbilical area (75.7%) with an incision diameter of 10 mm or more (86.3%). Umbilical wound enlargement to retrieve gallbladder specimens might be involved in TSHs. 13
Visceral obesity and previous midline surgery are two LC obstacles that surgeons frequently encounter. To address these two factors, a new technique was developed, the subcostal trocar approach using four 5-mm with exclusive removal (STAUFFER) LC. The aims of this study were to describe this technique, compare its outcomes with those of a standard LC approach, and highlight its advantages.
Methods
After the Mayo Clinic Institutional Review Board approved this study, a retrospective review was performed of medical records for all patients from June 2011 through December 2016 who underwent LC for gallbladder disorders by 1 surgeon (J.A.S.) at Mayo Clinic, Jacksonville, FL. Patients were excluded if they were younger than 18 years or had cholecystectomies performed in conjunction with other major procedures. Collected data comprised patient demographics, diagnosis, American Society of Anesthesiologists (ASA) classification scores, operative details, and postoperative morbidity and mortality. Complications were graded according to the Clavien-Dindo classification system 14 and were reported as minor (grades I and II) or major (grades III–V).
During this period, no cholecystectomies were performed by open technique. All patients were evaluated preoperatively with ultrasonography, computed tomography, or magnetic resonance imaging of the abdomen to evaluate the gallbladder. Perioperatively, a first-generation cephalosporin was given within 1 hour of the first incision.
Blood loss was estimated by both the surgeon and the anesthesiologist. Upsizing the trocar was defined as replacing a 5-mm port with a 12-mm port at the epigastric site. Concomitant procedures were defined as LC with simultaneous hernia repair or conversion to radical cholecystectomy. Operative time was calculated from the first incision to the last wound closure. Patients were discharged after they had adequate pain control and were tolerating their diet. Postoperative length of stay for outpatients was calculated in minutes from patient check-in until patient checkout from the recovery room according to the nursing documentation. Length of stay for inpatients was calculated from the first day of admission until the day of discharge. Patients were followed up at 1 month postoperatively. Subsequently, if any abdominal symptoms or protrusions persisted or developed, patients returned to the clinic for thorough evaluation, and suspected herniation at any trocar site was investigated.
Continuous variables were expressed as mean (range), and categorical variables were reported as number (percentage). Standard statistical analysis was performed. Significance was defined as P less than .05.
Standard technique
In the standard four-trocar LC (SLC) approach, the patient is positioned in a flat, supine, arms-out position, and the surgeon stands to the left of the patient. The initial trocar, a 12-mm periumbilical Hasson trocar, is used to gain access to the abdomen and to create pneumoperitoneum. Next, an epigastric 12-mm trocar and two right subcostal trocars are inserted. After cholecystectomy, the gallbladder is placed in a retrieval bag and removed through the periumbilical incision. When the operation is concluded, the specimen extraction site is closed with figure-of-8 heavy braided absorbable sutures. The fascia at the 12-mm epigastric trocar site is rarely closed because it is not dilated to remove a specimen, and the trocar is frequently placed through the falciform ligament.
STAUFFER technique
For the STAUFFER approach, the patient is positioned in a flat, supine, arms-out position. The patient is securely fixed to the bed with a circumferential strap or wide silk tape around the patient's chest, hips, and thighs to prevent any slippage on the bed during extreme positioning. The surgeon and the assistant stand to the left of the patient on a platform that elevates them to allow the operation to proceed at an ergonomically appropriate height when the patient is in extreme positioning. For abdominal access, the patient is tilted in a slightly reversed Trendelenburg position with the right side up, and a site on the right hemiabdomen is chosen (Fig. 1A).

Patient position.
In a patient with a normal body mass index (BMI), abdominal girth, and expected location of the umbilicus, the site chosen for visualized entry is ∼2 to 4 cm lateral and 2 to 4 cm superior to the umbilicus (Fig. 2A). Ideally, the entry is directed through the middle of the right rectus muscle equidistant between the midline and the lateral rectus sheath. In obese patients, the entry trocar is moved to the extreme right upper quadrant. In combination with changing the patient's position, this allows an optimal view of the gallbladder and the hepatoduodenal ligament.

Trocar placement.
The inferior margin of the right subcostal space is palpated and the visualized entry trocar is placed 10 to 12 cm inferior to this in the midclavicular line (Fig. 2B). Visualized entry is performed by placing a 0° laparoscope into an optical viewing trocar. After a 5-mm incision is made, the laparoscope and trocar are advanced carefully through the subcutaneous tissue, anterior rectus sheath, rectus abdominis muscle, and posterior rectus sheath into the abdomen under direct vision with insufflation. Pneumoperitoneum is ensured by watching the insufflation pressure decrease to less than the maximum limit as the abdomen inflates. The trocar obturator is removed, and the laparoscope is advanced into the abdomen to ensure that a safe entry was made and that the trocar tip is clearly within the abdominal cavity through the posterior rectus sheath and thin layer of peritoneum (Supplementary Videos S1 and S2; Supplementary Data are available online at www.liebertpub.com/lap). The 0° camera is then exchanged for a 30° laparoscope, and the abdomen is thoroughly explored.
The patient is next moved into a very steep reversed Trendelenburg position with the right side up (Fig. 1B) to allow for gravity retraction of the omentum and colon away from the gallbladder and right lobe of the liver in the right upper quadrant. Three additional right subcostal trocars are placed. The most lateral trocar is placed in the right anterior axillary line directly under the caudal extent of the 12th rib (Fig. 2A, B).
The epigastric trocar is again placed through the falciform ligament. The fourth trocar is placed in a configuration that allows for triangulation of the instruments in relation to the camera. After the cystic duct and cystic artery are clipped with a 5-mm clip applier and the gallbladder is separated from the liver, the gallbladder is placed into a specimen retrieval endoscopic bag and brought to the trocar at the right anterior axillary line. The trocar is removed, the skin incision is enlarged up to the expected size, the muscle and fascia are dilated with a long Kelly clamp, and the gallbladder is removed (Supplementary Videos S3 and S4.). At this point, the abdomen is completely desufflated through the trocars, and they are removed. The skin incisions are closed with a running subcuticular stitch, and no fascial closures are necessary.
If patients have a large cystic duct that prevents complete occlusion with a smaller clip, or if patients have severe inflammatory changes requiring packing of hemorrhage with surgical gauze, the 5-mm epigastric trocar is upsized to a 12-mm trocar. Generally, in those patients, the gallbladder is removed through this epigastric trocar site and the site is closed with a braided absorbable heavy fascial stitch.
Abdominal access and exploration are different in patients who have had multiple abdominal operations or who have “hostile abdomens.” In those patients, a visible entry access is chosen just inferior to the right subcostal region in the place of the left-hand trocar, and entry is performed as described above (Fig. 2A). Additional upper abdominal working space can then be created (often with blunt 0° laparoscope dissection) to allow further placement of the 5-mm trocar. If two trocars are inserted in a free space of the peritoneal cavity, additional room in the right subcostal region and right hemiabdomen for the third and fourth trocars is created with visualized dissection. After this, the camera is moved to the usual right hemiabdomen location for a conventional view for cholecystectomy.
Results
The total number of patients included in our study was 389. In 134 patients (34.4%), the SLC technique was performed; 255 patients (65.6%) underwent STAUFFER LC. The mean follow-up for patients was 18 months (range 1–64 months). Demographics and patient characteristics are shown in Table 1. Overall, 232 patients (60%) were female, mean age was 58 years (range 18–85 years), and mean BMI was 29.6 (range 17.6–49.5) (calculated as weight in kilograms divided by height in meters squared). Indications for surgery included chronic cholecystitis (71.7%), acute cholecystitis (19.8%), polyp (2.3%), and other (5.9%). Most patients (62.7%) had major medical comorbidities; the ASA scores are shown in Table 1. Previous abdominal surgery had been performed in 163 of the patients (41.9%), including 74 (19.0%) with previous upper abdominal surgeries and 8 (2.1%) with hostile abdomen. Mean BMI was higher for patients in the STAUFFER LC group than in the SLC group (P = .03). Comorbidities and ASA classification were not significantly different between the two groups. A higher percentage of patients in the STAUFFER LC group had previous abdominal upper or midline surgery compared with patients in the SLC group (22.4% versus 12.7%, P = .06). All the patients with hostile abdomen were operated on with the STAUFFER technique (P = .05).
Continuous data are presented as mean ± SD; categorical data, as number of patients (percentage of sample).
ASA, American Society of Anesthesiologists; BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); LC, laparoscopic cholecystectomy; SLC, standard four-trocar laparoscopic cholecystectomy; STAUFFER, subcostal trocar approach using four 5-mm with exclusive removal.
Operative details are shown in Table 2. Mean operative time was significantly higher in the SLC group (42 minutes versus 65 minutes, P < .001). Cholecystectomy in the SLC group was accompanied by concomitant procedures more frequently than in the STAUFFER LC group (0.8% versus 12.7%, P < .001); the vast majority of the procedures were hernia repair (95%). One patient in the STAUFFER LC group had a radical cholecystectomy that included full portal lymphadenectomy and partial hepatectomy. No entry site injuries occurred in either group. In 30 patients (11.8%) in the STAUFFER LC group, the medial subcostal trocar was upsized to a 12-mm trocar for reasons given below. No patient in this case series required conversion to open surgery.
Continuous data are presented as mean ± SD; categorical data, as number of patients (percentage of sample).
LC, laparoscopic cholecystectomy; NA, not applicable; SLC, standard four-trocar laparoscopic cholecystectomy; STAUFFER, subcostal trocar approach using four 5-mm with exclusive removal.
Pathologic findings, duration of stay, postoperative complications, and follow-up data are summarized in Table 3. Most LCs (77%) were performed as outpatient procedures. The percentage of patients who were outpatients was higher among those undergoing the STAUFFER LC compared to SLC (87% versus 58%, P = .02). The diagnosis of acute cholecystitis was more frequent in the SLC group than in STAUFFER LC group (30% versus 15%, P = .007), and the prevalence of acute inflammation with enlarged gallbladder and large gallstones influenced the decision about operative technique in favor of SLC.
Continuous data are presented as mean ± SD; categorical data, as number of patients (percentage of sample).
LC, laparoscopic cholecystectomy; SLC, standard four-trocar laparoscopic cholecystectomy; STAUFFER, subcostal trocar approach using four 5-mm with exclusive removal.
Overall, postoperative complications were rare, and no differences were noted between the groups. There were no bile duct injuries. In the STAUFFER LC group, 1 patient with a history of hematologic disease required a second laparoscopic operation for bleeding from the cystic artery, and 1 patient with a history of Crohn's disease, previous abdominal operations, and hostile abdomen had an enterocutaneous fistula develop in the left lateral trocar site postoperatively. The fistula was treated conservatively and closed spontaneously within 1.5 months. Mean length of hospital stay was significantly shorter for outpatients in the STAUFFER LC group than in the SLC group (293.04 ± 116.40 minutes versus 327.71 ± 126.19 minutes, P = .007). Overall mean follow-up was 17.69 ± 18.01 months and it was significantly longer for patients in the SLC group (25.40 months versus 13.64 months, P < .001), but SLC was the more common procedure in the first half of the study period (Fig. 3).
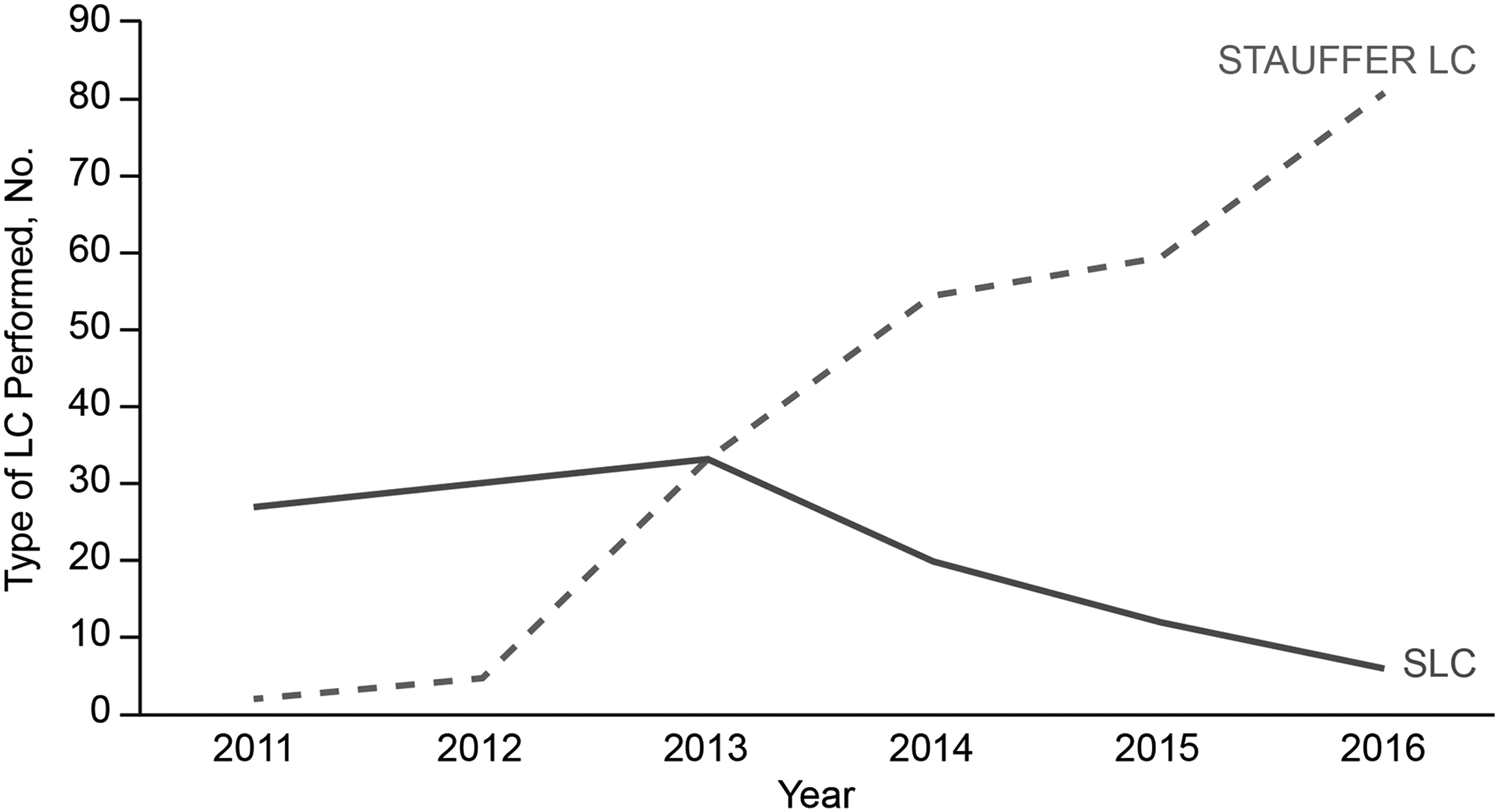
Types of LC performed, from June 2011 through December 2016. LC, laparoscopic cholecystectomy; SLC indicates standard four-trocar LC; STAUFFER, subcostal trocar approach using four 5-mm with exclusive removal.
Three patients required TSH repair after SLC, but no patients in the STAUFFER LC required TSH repair (P = .042). All three TSHs were at the umbilical area at the site of the 12-mm Hasson trocar and specimen extraction. One of the patients was a 76-year-old man with a BMI of 29, and the TSH developed 5 months after the SLC. The second TSH occurred 5 months after the SLC in a 74-year-old woman with diabetes mellitus and a BMI of 26. The third patient was a 72-year-old woman with a BMI of 39 who presented with a large, symptomatic TSH 2 years after SLC (Fig. 4). All patients underwent laparoscopic hernia repair with a 15 × 15-cm mesh.
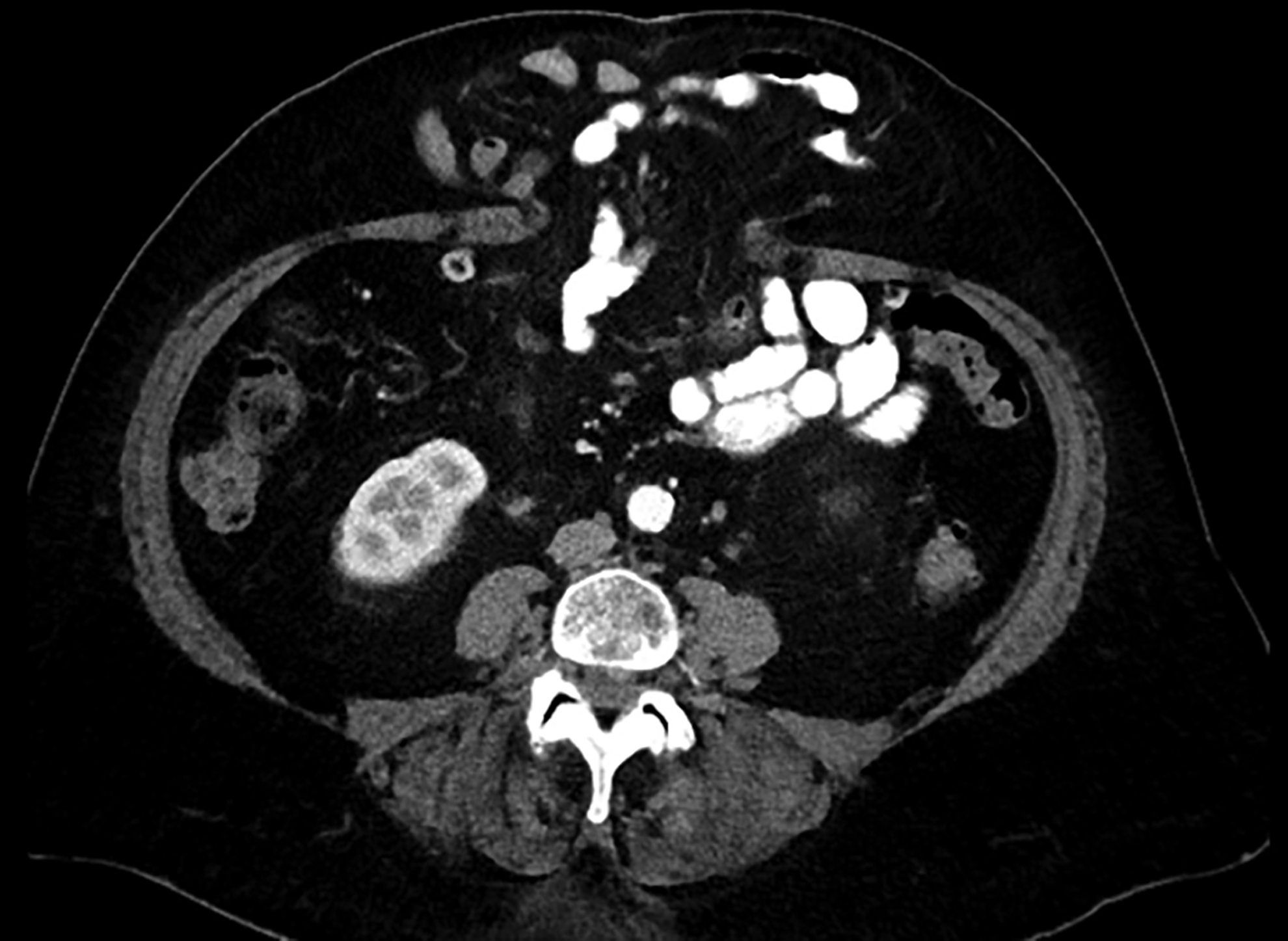
Large TSH. This TSH in a 72-year-old woman was detected 2 years after standard four-trocar LC with umbilical gallbladder extraction. LC, laparoscopic cholecystectomy; TSH, trocar site hernia.
Discussion
Ever since LC was introduced in 1987,2,3 a host of technical modifications have been devised to improve the safety, ease, and effectiveness of this procedure for patients with biliary disease. These modifications include cholecystectomy techniques with three-port, two-port, and single umbilical incisions.1,9,15 Nevertheless, the advantages of those methods are still debatable because of their limitations, such as technical challenges and longer operative times.1,9,10 Commonly encountered obstacles include visceral obesity, previous abdominal surgery resulting in adhesions, and long-term risks such as TSH.16–19 To lessen the effect of those factors, the STAUFFER LC technique was developed.
A common factor for gallstone formation is obesity, which increases the risk of a patient having gallstone-associated complications.20,21 According to a 2005–2011 American College of Surgeons National Surgical Quality Improvement Program database analysis of 73,540 patients undergoing cholecystectomy, 25% of the patients had a BMI greater than 35. 22 Obese patients undergoing LC pose challenges related to unclear anatomy because of increased visceral fat, difficulties with liver retraction, poor ergonomics because of an excessively thick abdominal wall, and related challenges of instrument manipulation.19,23 Placing the patient in a steep reversed Trendelenberg position with the right side up (Fig. 1B) and using high trocar placement (Fig. 2B) allow an anterior/posterior approach to the gallbladder, avoiding an inferior medial angle and greatly improving visualization over the transverse colon in obese patients.
Another well-known risk factor for intraoperative LC complications (bleeding, bile duct injury, and visceral perforation) is a previous upper abdominal operation, which can result in dense abdominal adhesions. 24 To avoid complications related to insertion of the first trocar in the abdominal cavity, we used a visualized entry away from the midline and umbilicus (the two areas most affected by adhesions from previous operations). This is also our preferred approach in patients with a hostile abdomen (rather than using a standard Hasson cutdown open technique), and we have not had any entry injuries. With the STAUFFER LC technique, a cholecystectomy can be performed through a small working space created in the right upper quadrant with four 5-mm trocars. This avoids other anatomical areas (which may increase the risk of complications related to adhesiolysis), as required with the SLC technique. Nevertheless, 1 patient in the STAUFFER LC group who had multiple previous abdominal operations for Crohn's disease and a hostile abdomen requiring adhesiolysis during LC had an enterocutaneous fistula develop postoperatively, but it resolved spontaneously within 1.5 months.
For a challenging gallbladder dissection, clinical practice guidelines of the European Association for Endoscopic Surgery 25 recommend performing partial cholecystectomy or conversion to open surgery. During the period of the present study, the surgeon (J.A.S.) did not perform any open cholecystectomies, partial cholecystectomies, or conversions to open surgery, largely because the STAUFFER LC was useful for patients with gangrenous cholecystitis, massive obesity, hostile abdomen, or severe liver cirrhosis. Thus, the STAUFFER LC technique can be used for essentially all cholecystectomy indications.
Furthermore, the STAUFFER LC drastically decreases operative time, mainly by saving time during abdominal entry and by not requiring fascial closure at the end of the operation. Improving visualization and avoiding midline adhesiolysis also contributed to a mean operative time of 42 minutes, which compares favorably to operative times in other series, ranging from 57 to 154 minutes.5,6,26
There is direct correlation between incision size and the frequency of TSH. Several studies16,17 have reported a higher incidence of TSH related to larger umbilical incisions in single-port cholecystectomy groups than in conventional LC groups. Moreover, 75% of TSHs after multiport laparoscopic interventions were identified at the umbilical site. 12 This fact may be explained by the use of an enlarged umbilical incision for specimen extraction 13 and abdominal wall anatomy. 27
The lateral abdominal wall contains the external oblique, internal oblique, and transversus abdominis muscles (Fig. 5). According to Duron et al., 27 the anatomy of the lateral abdominal wall, with these three muscular structures, makes it more difficult for hernias to occur at these sites than at the one-layer midline abdominal wall. In the STAUFFER LC technique, the most lateral trocar is inserted through an incision high under the right 12th rib created by insufflation of the abdomen. This wound is located at the level of the ribs and is covered by the deep sulcus of the right lobe of the liver (Fig. 2) after desufflation, obviating TSH, even after wound dilation and enlargement to accommodate specimen removal. At this site, even massively enlarged gallbladders and gallstones can be removed without fascial closure.
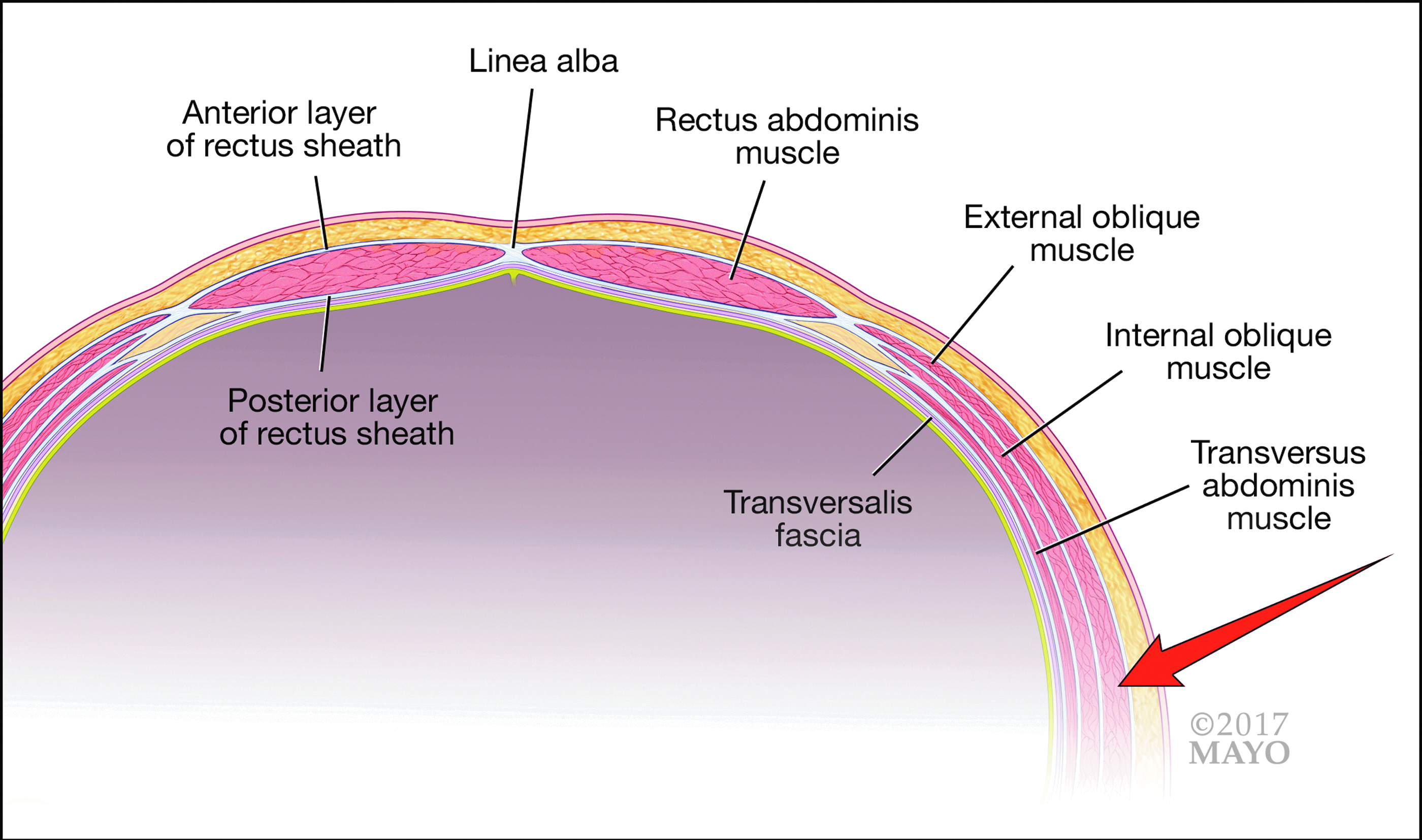
Anatomy of the abdominal wall. Arrow indicates lateral trocar insertion site. Used with permission of Mayo Foundation for Medical Education and Research.
Accounting for all the risk factors mentioned above, the STAUFFER LC technique is highly advantageous for nearly all patients for the following reasons: (1) Better intraoperative visualization is achieved in obese patients. The BMI in the STAUFFER LC group was significantly higher than in the SLC group (mean 30.12 ± 6.80 versus 28.54 ± 6.87) because STAUFFER LC was the preferred approach for those patients. (2) The STAUFFER LC technique provides easier entry in patients who have had a previous abdominal surgery or hostile abdomen, and it minimizes the risk of entry injuries. This is achieved with a carefully visualized trocar entry into the abdominal cavity in the right subcostal area. Previous midline abdominal surgery had been performed in 22% of patients in the STAUFFER LC group compared with 13% in the SLC group. An off-midline approach for patients with midline adhesions prevents inadvertent visceral injury and saves time by not requiring adhesiolysis. All the patients with hostile abdomen were operated on with the STAUFFER LC technique, and none of them had an entry site injury. (3) STAUFFER LC is faster than SLC (mean operative time 42.05 ± 16.0 minutes versus 64.74 ± 28.50 minutes; P < .001). The difference was mostly the result of worse visualization in obese patients in the SLC group and the additional time required for closing the 12-mm umbilical incisions. (4) In a mean follow-up of 17.69 ± 18.01 months, no patient in the STAUFFER LC group had a TSH, but 3 patients in the SLC group had paraumbilical hernias, all 3 of which required surgical repair. For all patients in the SLC group, the gallbladder was removed through the umbilical port, where herniation later developed (Fig. 4). In our opinion, exclusive removal of the gallbladder through the lateral 5-mm trocar site nearly eliminates the risk of TSH.
Regardless of all its advantages, the STAUFFER LC technique has three limitations that may preclude broad, worldwide implementation: (1) It requires a 5-mm clip applier, which may not be available in every hospital. (2) It is mandatory to have high-quality, 5-mm, 0° and 30° laparoscopes that allow adequate visualization. The optical quality of newer models is sufficient, but older models may provide subpar images. (3) A 5-mm endoscopic bag for gallbladder retrieval greatly facilitates gallbladder removal through a small dilated lateral incision, but, again, that may not be available in limited-resource areas.
In addition to the above technical limitations, our study itself also has several limitations: (1) It was a retrospective review, so selection bias was unavoidable. (2) A longer follow-up of all patients would be ideal to get a better sense of the rate of postoperative delayed complications such as TSH. Although most patients would likely follow up with the surgeon for TSH evaluation and repair, it is conceivable that some patients may present to surgeons elsewhere for diagnosis or repair. (3) Postoperative pain medication requirements were not measured; therefore, we cannot determine whether the STAUFFER LC approach results in less objective pain than the SLC approach. Subjectively, however, patients in the STAUFFER LC group reported a much faster recovery with diminished postoperative pain and earlier return to physical activity. Further studies will focus on this aspect of the technique.
In conclusion, the STAUFFER LC technique is widely applicable and effective, saving operative time and reducing the risk of incisional hernia. The STAUFFER LC technique is especially advantageous for obese patients and patients who have had previous surgery, and because of its many benefits, it is now the technique of choice for nearly all patients undergoing LC except for patients who are thin and who also need umbilical hernia repair.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.