
Abstract
Abstract
Introduction:
Diagnostic laparoscopy (DL) is a well-accepted approach for penetrating abdominal trauma (PAT). However, the steps of procedure and the systematic laparoscopic examination are not clearly defined in the literature.
The aim of this study was to clarify the definition of DL in trauma surgery by auditing DL performed for PAT at our institution, and to describe the strategies on how to avoid missed injuries.
Methods:
The data of patients managed with laparoscopy for PAT from January 2012 to December 2015 were retrospectively analyzed. The details of operative technique and strategies on how to avoid missed injuries were discussed.
Results:
Out of 250 patients managed with laparoscopy for PAT, 113 (45%) patients underwent DL. Stab wounds sustained 94 (83%) patients. The penetration of the peritoneal cavity or retroperitoneum was documented in 67 (59%) of patients. Organ evisceration was present in 21 (19%) patients. Multiple injuries were present in 22% of cases. The chest was the most common associated injury. Two (1.8%) iatrogenic injuries were recorded. The conversion rate was 1.7% (2/115). The mean length of hospital stay was 4 days. There were no missed injuries. In the therapeutic laparoscopy (TL) group, DL was performed as the initial part and identified all injuries. There were no missed injuries in the TL group. The predetermined sequential steps of DL and the standard systematic examination of intraabdominal organs were described.
Conclusions:
DL is a feasible and safe procedure. It accurately identifies intraabdominal injuries. The selected use of preoperative imaging, adherence to the predetermined steps of procedure and the standard systematic laparoscopic examination will minimize the rate of missed injuries.
Introduction
L
Initially laparoscopy was used mainly as a screening or diagnostic tool, with a therapeutic role emerging as confidence around the safety and reliability increased.2,5–10 Today laparoscopy in trauma can be divided into screening, diagnostic and therapeutic applications.
The role of screening laparoscopy initially was to detect peritoneal breach which would then be followed by an exploratory laparotomy. 10
Diagnostic laparoscopy (DL) goes a step beyond screening and is used to assess the peritoneal cavity in a thorough, systematic and meticulous way. This is very much in line with what would be described in the open era as diagnostic exploratory laparotomy. DL not only identifies intraabdominal injuries but also makes therapeutic intervention possible. 11
Therapeutic laparoscopy (TL) for trauma is reported to be feasible and safe, provided appropriate expertise is available. The rate of TL is 55% in the recent study. 4
The definition of DL is not clear in the literature, with screening laparoscopy often being confused with DL. Some centers convert when there are any suspicious retroperitoneal injuries, peritoneal breach, signs of hollow viscera injuries, or organ evisceration.12,13 The steps of procedure and the systematic laparoscopic examination are not clearly described in the literature.
The aim of this study was to clarify the definition of DL in trauma surgery by auditing all DLs performed for penetrating abdominal trauma (PAT) at our institution. Following this we describe the strategies on how to avoid missed injuries. The study was approved by the Sefako Makgatho University Research Ethics Committee, Pretoria, South Africa.
Methods
This is a retrospective descriptive study from a prospectively collected database of patients admitted at Dr. George Mukhari Academic Hospital. This hospital is a tertiary referral institution in northwest Pretoria, South Africa. All adult patients with PAT who underwent DL from January 2012 to December 2015 were included in the study. Cases of patients under 12 years, hemodynamically unstable patients, or cases where there were missing or unclear records were excluded. All unstable patients were managed with laparotomy. Demographic data, mechanism of injury, location of injury, intraoperative findings, grading of injuries, intraoperative maneuvers, trauma scoring, length of hospital stay (LOS), and complications were interrogated. Strategies on how to avoid missed injuries were discussed.
Definitions
Penetration of the abdominal cavity was defined as a violation of the parietal peritoneum or retroperitoneal tract or hematoma signifying the possibility of injury to the intra- or retroperitoneal organs.
DL (nontherapeutic) was defined as procedure when there were no injuries or the identified injuries did not require repair. Evacuation of liquid blood or clots and mobilization of any intra- or retroperitoneal organs for diagnostic purposes were not considered therapeutic.
TL was defined as the laparoscopic management of intraabdominal injuries (more than observation or hemostatic agent application).
Laparoscopic procedures were fully laparoscopic or laparoscopic-assisted. In the fully laparoscopic procedures all interventions were performed intracorporeally. In laparoscopic-assisted procedures the injured bowel was eviscerated through 4–8-cm assisted incision for extracorporeal inspection, repair, resection, or anastomosis, usually for multiple injuries. In some patients, intracorporeal procedures were combined with extracorporeal procedures to minimize trauma to the patient.
The locations of the injuries were subdivided into five areas: the anterior abdominal area, the right and the left lower chest, the flank, and the back. 8
Although the final decision on stability of patient was left for attending surgeon, the following criteria were commonly used to define an unstable patient: the systolic blood pressure below 90 mm Hg and the mean inspiratory pressure greater than 30 mm Hg.
Operative procedure
The operative procedure was performed under general anesthesia.
DL consisted of the following sequential steps of procedure:
1. Access, pneumoperitoneum, and ports placement The camera port (11 mm) was placed by open (Hasson) technique through the periumbilical area, Palmar point, or the injury site. Carbon dioxide pneumoperitoneum of 12–15 mm Hg was established. At least two working ports (5 or 11 mm) were placed at the mid-axillary line in the right and left iliac fossae. If necessary, additional ports were placed at the hypogastrium, right and left hypochondrium (Fig. 1). 2. Quick assessment of the abdomen and bleeding control A 30-degree telescope, suction-irrigation and one or two atraumatic forceps were used for this step. Liquid blood, clots, and gastrointestinal contents were suctioned and active bleeding was sought. Bleeding was controlled with atraumatic forceps followed by laparoscopic vascular clamp, clips, energy source, over-suturing, or ligation. If hemostatic agent application only was used to control minor bleeding, the procedure was treated as DL. If more advanced therapeutic options were used, the procedure was referred to as TL. If bleeding could not be controlled promptly, the procedure was converted to laparotomy. 3. Systematic inspection of intraperitoneal and retroperitoneal organs The extent of mobilization was guided by clinical findings and preoperative imaging. There was liberal use of gravity retraction by changing the operating table position to retract bowel away from the area of examination to maximize visibility. Systematic inspection was performed in the following order: 3.1. The diaphragm Examined first after bleeding was controlled, because the communication with the pleural cavity can cause patient instability. 3.2. The liver and gallbladder Usually examined intraperitoneally but mobilized if needed (the peritoneal attachments or ligaments were divided to examine the area of interest). 3.3. The spleen Usually examined intraperitoneally but mobilized if needed (the peritoneal attachments or ligaments were divided to examine the area of interest). 3.4. The anterior wall of the stomach Examined intraperitoneally but mobilized if needed. 3.5. The gastrocolic ligament division The energy source was used. 3.6. The posterior wall of the stomach Elevated with graspers to examine from beneath. 3.7. The pancreas and related retroperitoneal area Examined intraperitoneally but mobilized if needed. 3.8. The duodenum above the mesocolon Usually examined intraperitoneally but, in case of penetration of the retroperitoneal space, the duodenum was mobilized and examined. 3.9. The duodenum below the mesocolon As in 3.8. 3.10. The small bowel run from the ligament of Treitz to the ileocaecal junction The careful inspection of small bowel was mandatory, if a violation of peritoneum was confirmed or pathological content discovered in the abdominal cavity, it was strongly recommended to run the small bowel twice from the Treitz to the ileocecal junction and back, especially for novice surgeons. Approximately 10 cm of the bowel is spread between two atraumatic graspers and then rotated around for full examination. This maneuver was repeated until the entire bowel is examined. Clots and fibrinous exudate were carefully removed by using suction and a dry small swab so as to examine the underlying bowel, where there was contusion or suspicious area, a blunt atraumatic grasper was used to probe the bowel wall to ensure that there was no partially sealed bowel injury. Hematomas around the bowel wall were carefully inspected with liberal bowel mobilization and a dry swab was used to remove the hematomas and enable adequate bowel wall examination. 3.11. The right colon (the caecum, ascending colon, and the hepatic flexure) with the right kidney, hilum, and ureter The colon was mobilized in appropriate settings and the retroperitoneal content was examined. 3.12. The transverse colon The examination was done in the same way as for the small bowel. 3.13. The left colon (the splenic flexure, the descending and sigmoid colon) with the left kidney, hilum, and ureter As for 3.11. 3.14. The pelvic cavity (the rectum and the urinary bladder) Usually examined intraperitoneally but, in case of penetration of the retroperitoneal space, the content was mobilized and explored. 3.15. The additional areas of interest and other areas requiring extra attention (e.g., the IVC, aorta) To ensure a standard systematic, complete inspection of intraperitoneal and, if required, retroperitoneal organs, we used a memory aid in the form of the following rhyme. Memory aid (Fig. 2) 4. Decision to proceed with laparoscopy, laparoscopic-assisted approach (LAA) or conversion Depending on the findings, further management was decided upon by the operating surgeon. Where injuries were found, these were dealt with laparoscopically either as totally laparoscopic or laparoscopic-assisted. Patients were admitted to the general ward for hemodynamic monitoring after the operation and were discharged once they tolerated oral feed and were stable.

Most common (open circles) and additional (gray circles) port placement sites.
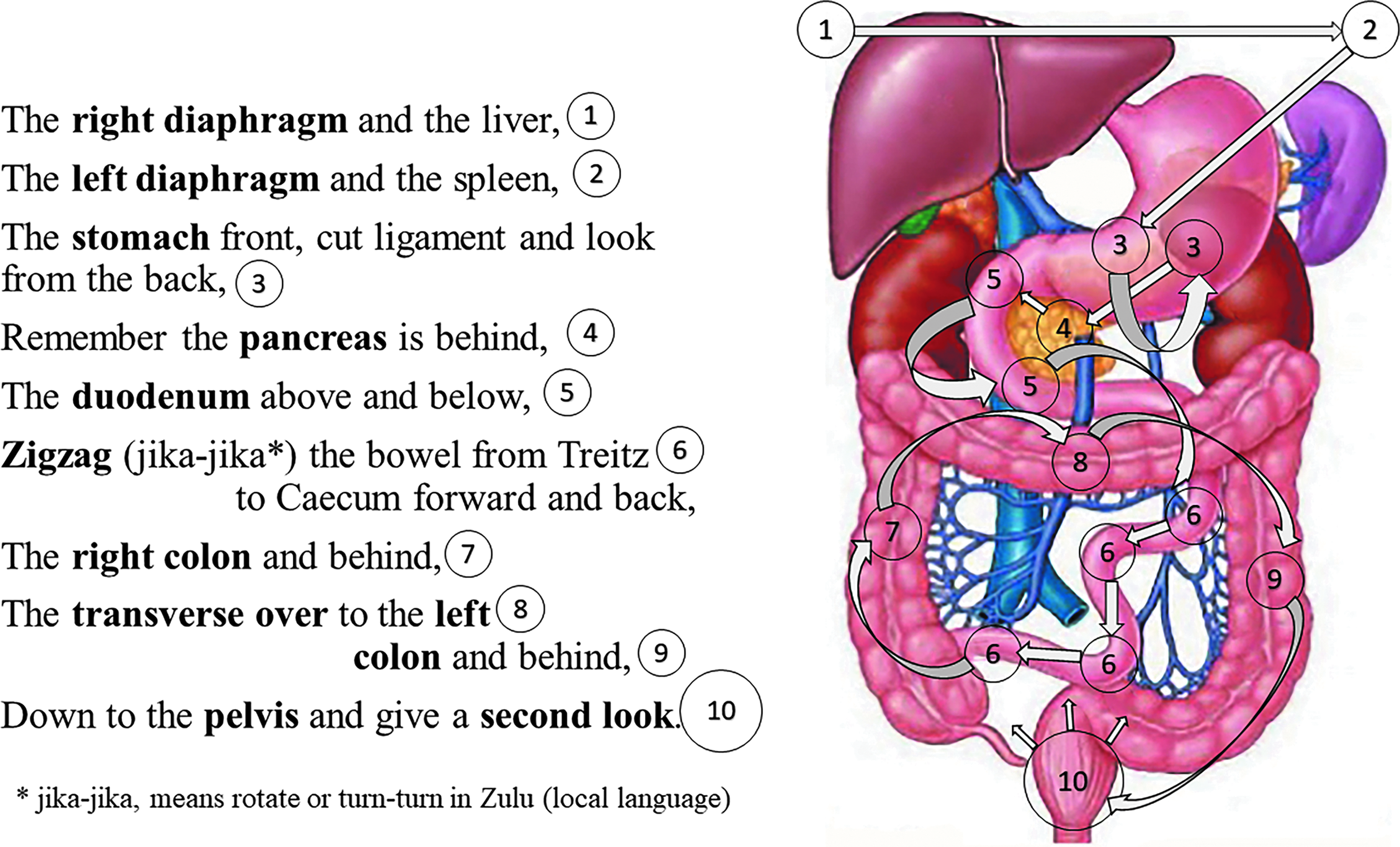
Memory aid for laparoscopic systematic inspection of intraabdominal organs.
Data analysis
Demographic details of the patients were summarized descriptively by mean, minimum, and maximum values for continuous variables and frequency count and by percentage calculations for categorical variables. The Fisher's exact test was used for comparisons. A value of P < .05 was considered significant. All statistical procedures were performed with SAS software (SAS Institute, Cary, NC).
Results
A total of 318 trauma patients were approached laparoscopically (Fig. 3). Thirty-five patients with blunt abdominal trauma were excluded from the study. Out of 283 patients with PAT, 33 (11.7%) patients were converted to laparotomy. TL was performed in 137 (55%) cases. DL was performed on 113 (45%) patients and this group was analyzed.
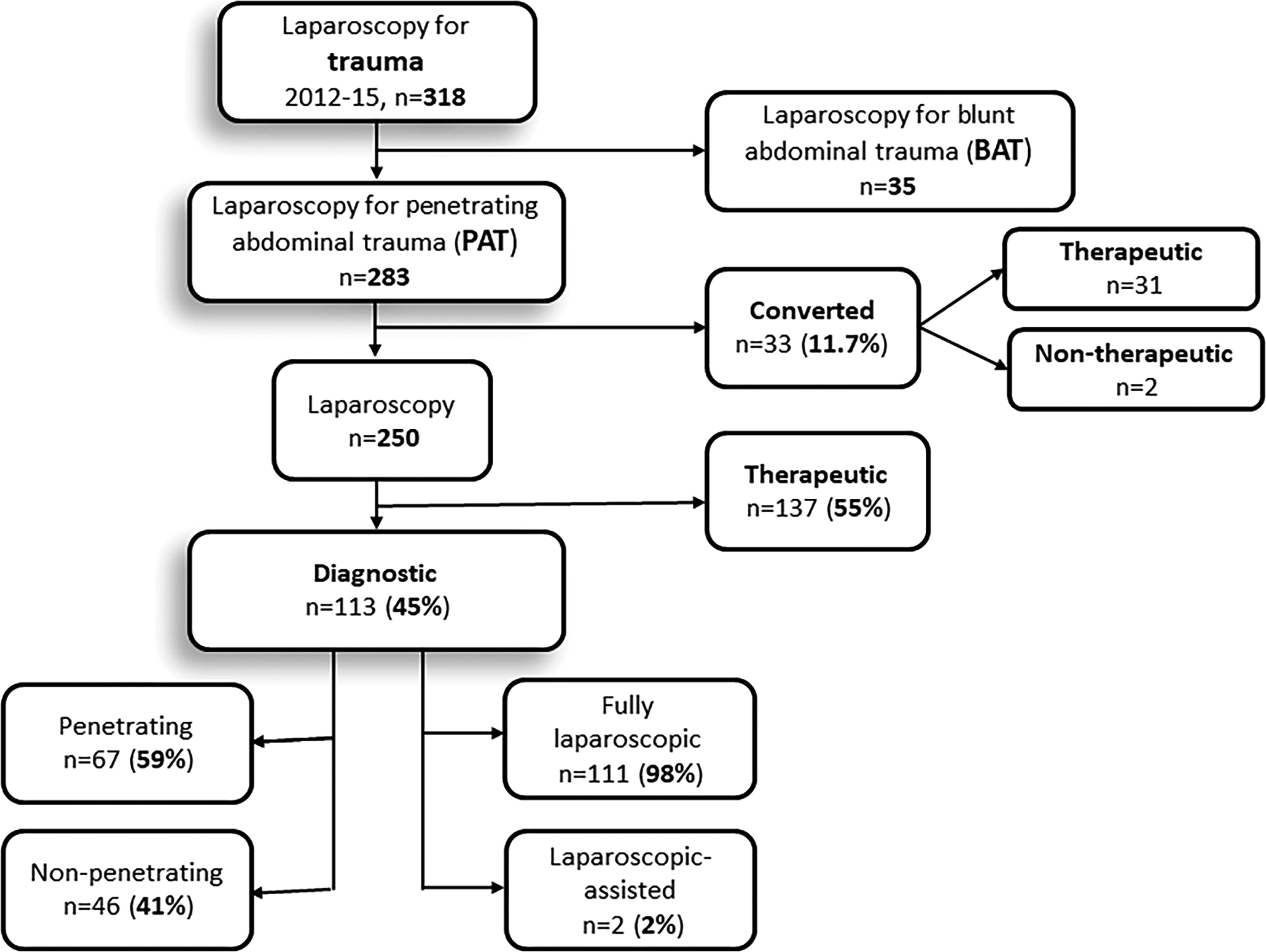
Study diagram.
The mean age was 32 years and 86% of patients were male (Table 1). The majority of the patients (n = 94, 83%) sustained stab wounds. The penetration to the peritoneal cavity or retroperitoneum was documented in 67 (59%) patients and 46 (41%) patients didn't have penetration. Organ evisceration was present in 21 (19%) patients and 7 (33%) of them had small bowel evisceration. LAA was used in 2 (2%) patients with organ evisceration. No injuries were recorded. The traumatic hernia site was repaired extracorporeally in all cases. The most common location of injury was the anterior abdominal wall (45%) and in 84% of cases the peritoneum was violated. In 31% of cases the injury was located on the lower chest and penetration was recorded in 26%. However, the diaphragm was not injured in any of the cases. Flank injuries were present in 21% and the back was in 3% (Table 2). Multiple injuries were present in 22% of cases. The chest was the most common associated injury. Pneumothorax was present in 26%, and clotted hemothorax was diagnosed in 6%. One patient had penetrating cardiac injury diagnosed during diagnostic thoracoscopy and sternotomy was performed for cardiac injury repair. The mean injury severity score (ISS) was 6, abdominal new ISS (aNISS) was 5 and penetrating abdominal trauma index (PATI) was 0.9.
SD, standard deviation; ISS, the Injury Severity Score; aNISS, the abdominal New Injury Severity Score; PATI, the Penetrating Abdominal Trauma Index; LOS, the length of hospital stay.
GSW, gunshot wound; CD, Clavien-Dindo classification.
The colon was mobilized in 19 patients and the liver in 1 patient. The isolated retroperitoneal exploration was reported in 3 cases. However, the details of exploration were not provided in operative notes. The location and grade of injuries discovered during DL are listed in Table 3. None of the injuries required any therapeutic procedures.
Two (1.8%) iatrogenic injuries were recorded. One patient had a serosal injury of the small bowel and pinpoint perforation that required stitch-repair, the second patient had minor bleeding from the splenic capsule injury that was controlled by diathermy. Two patients in the converted group had nontherapeutic laparotomy, which constituted the conversion rate of 1.7% (2/115) for DL (Fig. 3). Visualization problems necessitated the conversion in 1 patient and the need for exploration of a zone 1 retroperitoneal hematoma in second patient.
There were no missed injuries. Two patients suffered complications. One patient with the gunshot wound required thoracoscopy for clotted hemothorax evacuation on postoperative day 8, the second patient with stab wound developed renal arteriorvenous fistula and was managed endovascularly. Both patients recovered uneventfully. All patients were followed until discharge from hospital, but most failed to come for their scheduled follow-up visit in 2 weeks after discharge. The overall mean LOS was 4 days, and in patients without comorbidities LOS was 3.4 days. The LOS did not differ significantly between patients with penetration and without penetration.
In the TL group, DL was performed in all patients as the initial step and identified all injuries. There were no known missed injuries in the TL group.
Discussion
Currently, DL in trauma is an accepted technique. 9 At first, laparoscopy started as a screening tool with laparotomy being performed for any uncertainties. The initial attempts of laparoscopic exploration of abdominal cavity resulted in the high rate of missed injuries. 2 With the improvement of laparoscopic equipment and surgical techniques, and development of systematic laparoscopic examination of the abdominal cavity, the rate of missed injuries decreased and is reported to be far below 1%.9,14,15 Moreover, the recent studies report no missed injuries.4,16
Definitions of DL in trauma vary. Many investigators use laparoscopy in trauma to identify those patients with penetrating injuries where there is a breach in peritoneum and laparotomy would follow. 17 This should be referred to as screening laparoscopy. This approach has been shown to decrease the rate of nontherapeutic laparotomy quite substantially. 18 The current role of screening laparoscopy is limited, however, it can be used under local anesthesia and intravenous sedation in the trauma bay as Laparoscopic Assessment in Surgical Trauma.18–20 The significant advantage of screening laparoscopy is an early discharge and the mean LOS of 6.4 hours was reported. 21
In our view, DL in trauma identifies and possibly grades all intraabdominal injuries by using the standard systematic complete inspection of intraperitoneal and, if required, retroperitoneal organs, and to attend to minor injuries not requiring major therapeutic options, like clots evacuation or hemostatic agent application. DL identifies all injuries as effectively as a diagnostic laparotomy would. Hypothetically, DL should be more accurate than laparotomy, due to superior visualization with high definition magnified imaging of all inaccessible during laparotomy areas. This hypothesis is to be tested in the future.
The introduction of a systematic examination in trauma laparoscopy has reduced the rate of missed injuries from 13% to below 1%.2,3,9 However, the extent of laparoscopic exploration differs between centers. Kawahara et al. stopped laparoscopic exploration at the blind spots zones: the retroperitoneum, injuries to the bare area or segments VI and VII of the liver, or posterior area of the spleen. 12 Other surgeons aborted laparoscopic exploration at the sight of intestinal content in the peritoneal cavity, a visible bowel injury, or mesenteric or solid organ injury.20,21 In this study, complete inspection of all organs was performed, if required.
In order not to miss injuries, DL follows the predetermined steps. 4 The standard systematic examination is the most important step in identification of injuries, however, the technique was not clearly described in the literature. Kawahara et al. suggested examining inframesocolic and then supramesocolic spaces with concentration on hollow viscera, and at the end examine the liver and spleen. 12 Uranues began systematic exploration with the right upper quadrant and proceeded clockwise. 10 Our study presented the standard systematic examination, memorized as a rhyme by the surgeons, which begins from the diaphragm and follows the digestive tract and related anatomical regions. For easy recollection, the memory aid in rhyme and visual form was provided (Fig. 2). We find that this sequence of intra-abdominal examination offers economy of movement and avoids a nonstructured examination that may result in missed injuries. Initial control of encountered bleeding (Step 2) should precede any systematic examination. After bleeding is controlled, the next possible injury to cause patient instability is the diaphragm. That is why the systematic examination (Step 3) usually starts from inspection of the diaphragm. The missed injuries of gastrointestinal tract are the most ominous. We recommend to follow the systematic examination along the gastrointestinal tract and at the same time examine organs in related anatomical regions.
Routine exploration of retroperitoneal organs cannot be justified if there is no clinical indication. The proximity of injury, presence of penetration or pathological content in the retroperitoneal space, or any other suspicion for the retroperitoneal injuries requires full laparoscopic mobilization and exploration of related organs. In this series, preoperative imaging with the CT scan was found to be beneficial to guide the extent of laparoscopic exploration of retroperitoneal organs. CT scan may also be used to select patients who will benefit from nonoperative management and will avoid laparoscopy.22,23 We suggest preoperative CT scan where retroperitoneal injuries are suspected, as it contributes to the laparoscopic exploration of the retroperitoneum.
DL precedes all therapeutic laparoscopies. If injuries requiring repair are identified, the procedure will progress to TL. In this study, DL identified all injuries in DL and TL groups.
LAA is mainly used for multiple bowel injuries as a part of TL.24,25 However, this study reported 2 cases of anterior abdominal stab wounds and organ evisceration where LAA was used for diagnostic purpose. Traumatic hernia was extended and the bowel was eviscerated through the injury site for inspection.
Organ evisceration carries a high rate (65%) of significant intra-abdominal injuries and needs exploration.1,26 In this study, laparoscopy ruled out intra-abdominal injuries in all 21 (19%) patients with evisceration. The patients diagnosed with significant injuries were treated with TL. There were no missed injuries in either groups. The laparoscopic management of patients with organ evisceration is reported to be feasible and safe. 26
Two iatrogenic (1.8%) injuries occurred in this series. Those were minor injuries and required minimal therapeutic procedures. By definition, it should have been regarded as TL, however, we decided to include those cases in the study to highlight the possibility of iatrogenic injuries. Such minor injuries usually happen during laparoscopy and laparotomy, but not always reported. 17
This study reported the conversion rate 1.7% in the DL group. Prompt conversion to laparotomy is required in cases of continuous intraoperative bleeding, complexity of injuries, deterioration of the patient, poor visibility, and equipment failure. 4
The indications for diagnostic laparotomy and DL in the trauma setting are the same, but DL is minimally invasive with all the related benefits. If there is enough expertise in laparoscopy, all stable trauma patients should be explored laparoscopically. 4 Laparotomy is reserved for unstable trauma patients. However, Cherkasov et al. reported the safe use of laparoscopy in unstable patients. 27 In this study, all patients were stable. We do not recommend laparoscopy for unstable trauma patients, as besides other issues, an unstable patient forces a surgeon to rush through procedure to finish operation quickly, and that may pose the high risk of missed injuries.
In this study, we reported that the overall LOS for DL was 4 days and in patients without any associated injuries was 3.4 days. The interpretation of this LOS should be made with caution. The study was retrospective and LOS was not strictly monitored. Often patients stayed in hospital longer than needed due to logistics issues rather than requiring hospital care.
Conclusions
This study outlined the following strategies on how not to miss injuries during trauma laparoscopy:
1. selection of patient for initial laparotomy (unstable patients, limited laparoscopic expertise); 2. the use of CT scan imaging, in appropriate setting, to identify the tract and plan laparoscopy (instances of injuries to retroperitoneal space, the patient who qualifies for nonoperative management, the delay in waiting for operation is expected); 3. strict adherence to the predefined steps of DL; 4. implementation of standard systematic exploration of all intraabdominal organs; 5. surgeon's complete satisfaction with laparoscopic procedure: laparotomy would not offer more than laparoscopy.
DL is a feasible and safe procedure. The selected use of preoperative imaging, adherence to the predetermined steps of procedure and the standard systematic laparoscopic examination will minimize the rate of missed injuries.
Authors' Contributions
Study conception and design (M.K., O.M.); literature search and data collection (O.M.); data analysis, data interpretation, and article preparation (O.M., M.K.); critical review and revision of the article (C.A.); and mentoring throughout the article preparation (C.A.).
Footnotes
Disclosure Statement
No competing financial interests exist.