
Abstract
Abstract
Background:
Laparoscopic isolated caudate lobectomy remains a challenging procedure because of its deep location and proximity to the important vessels. We present a novel technique, Arantius ligament suspension, which could improve operative field exposure in laparoscopic isolated caudate lobectomy through retraction of the left lateral lobe liver.
Materials and Methods:
The Arantius ligament suspension technique was performed in 6 selected patients during laparoscopic isolated caudate lobectomy in our center: 2 with symptomatic hepatic cavernous hemangioma and 4 with hepatocellular carcinoma (HCC). The Arantius ligament suspension technique was performed using a 2-0 polypropylene suture (Prolen2-0®; Ethicon, Somerville, NJ), which was secured to the Arantius ligament with surgical clips at its halfway point and the left lateral lobe of liver would be retracted toward the abdominal wall when the suture was tightened. Perioperative data of these patients and follow-up data of HCC patients were retrospectively reviewed.
Results:
All 6 procedures were completed without conversion to open surgery or requiring additional ports. The mean tumor size was 5.4 cm (2.2–7.8 cm), the mean blood loss was 260 mL (50–440 mL), and no patients required blood transfusion during the operation. The mean time required for this technique was 2 minutes 5 seconds (1 minutes 36 seconds–2 minutes 44 seconds) and the mean duration of entire surgery was 249 minutes (173–300 minutes). The mean postoperative hospital stay was 7 days (5–9 days) and no postoperative complication related to the suspension procedure occurred.
Conclusions:
Our outcomes demonstrated the Arantius ligament suspension technique is a feasible and ideal method during laparoscopic isolated caudate lobectomy for providing a rapid and safe left lateral lobe retraction.
Introduction
T
Despite the increasing number of laparoscopic liver resection reported, there are very few studies about isolated caudate lobectomy using laparoscopic methods.4–11 The caudate lobe is described as an autonomous segment of the liver with its own vascularization and biliary drainage. And it is surgically difficult to approach due to its deep location beneath the confluence of the left and middle hepatic veins and its close proximity to the Arantius ligament, hepatic hilum, and the inferior vena cava (IVC). 12 Therefore, a fully visual operative field and an adequate working space are the vital prerequisite to perform laparoscopic hepatic caudate lobectomy safely.
In this study, we describe a novel technique to help obtaining a clear exposure and a sufficient surgical space in laparoscopic hepatic caudate lobectomy.
Materials and Methods
Patients
From January 2013 to December 2016, there were 572 laparoscopic hepatectomy for benign and malignant liver tumors carried out in our center. In this series, laparoscopic isolated caudate lobectomy using the Arantius ligament suspension was carried out in 6 patients from April 2014 to October 2016. All patients received preoperative examinations and were diagnosed with a solitary hepatic tumor in the caudate lobe, including 2 symptomatic hepatic cavernous hemangioma and 4 hepatocellular carcinoma (HCC) with varying degrees of liver cirrhosis. They all had normal preoperative hepatic and thromboplastic functions. The operative time, conversion to laparotomy, blood loss, hospital stay after surgery, and postoperative complications were reviewed. All HCC patients were followed up.
Operative technique
The patients were in the supine position with both legs close together. A 12 mm camera port was placed though a subumbilical incision. Two 10 mm ports were placed 5–6 cm above the umbilicus at the outer border of the rectus muscle. Two 5 mm ports were placed in the left and right subcostal anterior axillary line (Fig. 1). The surgeon was on the right side of the patient, while the assistant and camera operator were on the opposite side.
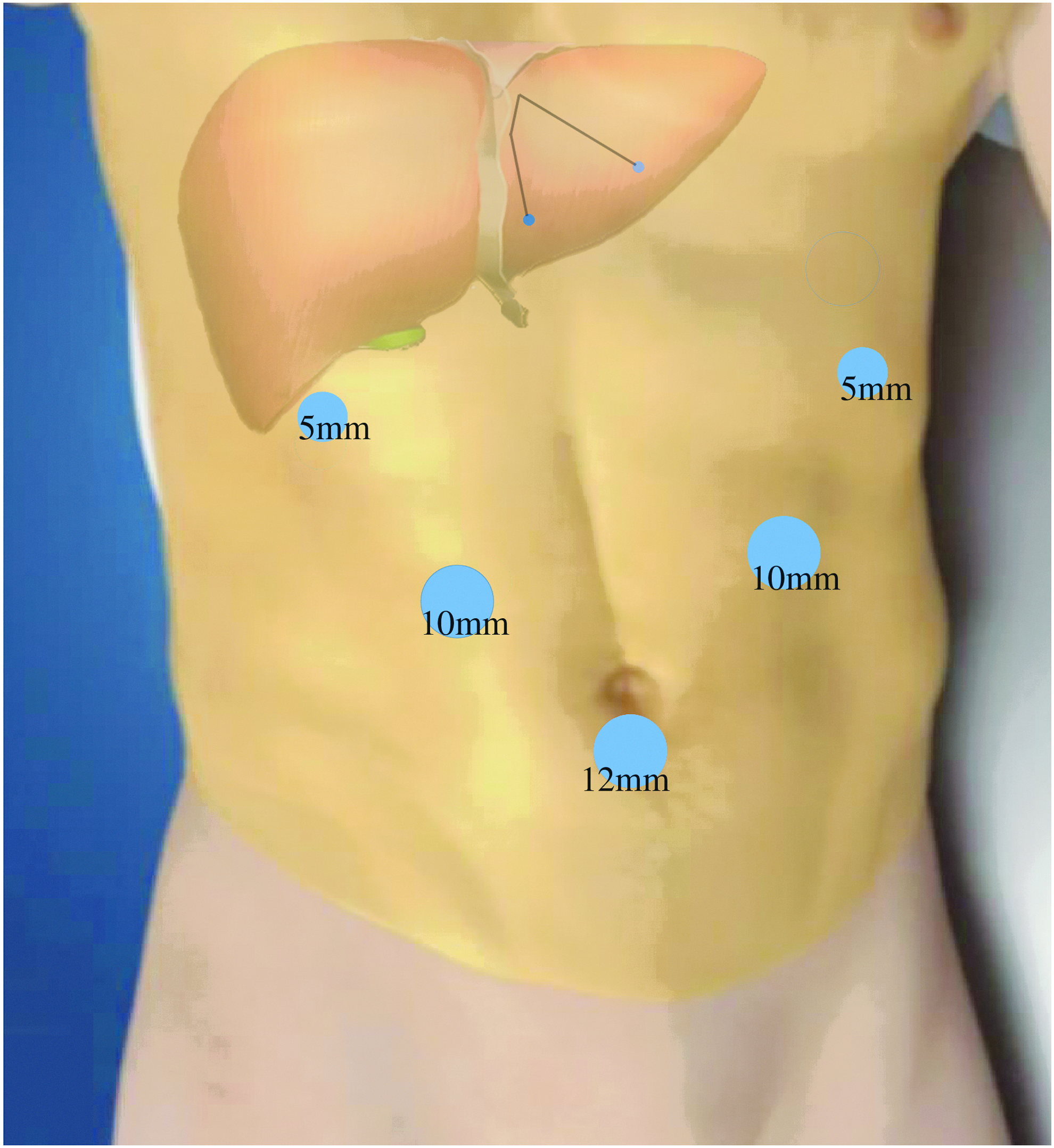
Details of the port placement and skin puncture sites for Arantius ligament suspension technique.
The lesser omentum near the Arantius groove was divided to expose Arantius ligament and the left portion of the caudate lobe (Spiegel's lobe). A long straight needle with a 2-0 polypropylene suture (Prolen2-0®; Ethicon, Somerville, NJ) was brought into the abdominal cavity percutaneously from the left subcostal area, and then pierced the anterior abdominal wall at the left side of the falciform ligament to become exteriorized with certain length of suture remained in the peritoneal cavity (Fig. 2A, B). The remained suture was fixed to the Arantius ligament at the position near the left hepatic pedicle with one or two 5 mm hemolok clips (Fig. 2C). Finally, the left lateral lobe of the liver could be lifted up by the tensioned suture when the both ends of the suture were pulled externally (Fig. 1, Fig. 2D). Without pressure of left lateral lobe, the Spiegel lobe could easily be lifted up with a 5 mm laparoscopic liver retractor and the short hepatic veins were dissected and divided under direct vision (Fig. 2E).

Procedure of the Arantius ligament suspension technique and laparoscopic hepatic caudate lobectomy.
Additionally, we applied a modified laparoscopic Pringle's vascular control technique: a cotton tape encircling the hepatoduodenal ligament was exteriorized through a self-made tube with rubber joints and hepatic blood inflow could be occluded if the ends of the cotton tape were pulled outward while the tube was pushed inward via an operation trocar (Fig. 2G). Under intermittent Pringle's vascular control, liver parenchyma transection using a harmonic scalpel was initiated at the right border of the caudate process and subsequently proceeded in the cranial and left direction until the caudate lobe was completely divided from the posterior surface of the second porta hepatis (Fig. 2F). Finally, the retrohepatic IVC was fully exposed after complete resection of the caudate lobe (Fig. 2I). The liver cut surface was checked carefully in case of bile leakage (Fig. 2H). The suspension suture was removed easily after the hemolok clips were destroyed, which had been fixed to the Arantius ligament. The specimen in a retrieval bag was extracted through the extensive subumbilical port. A small suction drain was placed close to the transection margin through the right 10 mm trocar.
Results
All procedures for these 6 patients were completed as planned without conversion to open surgery or requiring additional ports. Although the peritoneal attachments of the left lateral lobe liver were preserved in some cases, the left lateral lobe liver still could be adequately retracted by the Arantius ligament suspension technique and providing a good visual operative field and working space. The clinical characteristics and perioperative parameters were showed in Table 1. This technique cost a mean time of 2 minutes 5 seconds (range, 1 minutes 36 seconds–2 minutes 44 seconds) and the mean duration of entire surgery was 249 minutes (range, 173–300 minutes).
F, female; HCC, hepatocellular carcinoma; M, male.
The average blood loss was 260 mL and no patients required blood transfusion during the operation. The mean tumor size was 5.4 cm (range, 2.2–7.8 cm). All tumors were located in the Spiegel lobe and the paracaval portion. Pathological examination was consistent with the preoperative diagnosis and all resected HCC specimens had negative surgical margins. Perioperative complications were seen in 2 patients including slight wound infection and left pleural effusion. However, no complication related to the suspension procedure was recorded. The average postoperative hospital stay was 7 days (range, 5–9 days). Preoperative uncomfortable symptoms of both patients with hepatic hemangioma disappeared at the time of hospital discharge. The mean follow-up time of HCC patients was 19 months (range, 6–31 months) and no dead or tumor recurrence occurred during the follow-up.
Discussion
Primary hepatic tumors originating in the caudate lobe or a single caudate lobe metastasis is not common and these patients are easily to lose the chance of radical resection for tumor invasion of the IVC. Besides, isolated caudate lobectomy requires profound anatomic understanding of the caudate lobe and exquisite skill of operation even in open approaches. Therefore, laparoscopic isolated caudate lobectomy remains unfamiliar to many surgeons and there are few reports in the literature on this subject. In our series, all procedures were completed without conversion to open surgery or requiring additional ports. All materials used for constructing the Arantius ligament suspension are easily obtained and the entire procedure takes only about 2 minutes. The average blood loss was 260 mL and no patients required blood transfusion during the operation. The postoperative complications were few and slight, and the length of postoperative hospital stay was short (7 days, 5–9 days). All surgical margins were pathologically negative and 4 HCC patients were all alive with no sign of recurrence during the follow-up.
Anatomically, the caudate lobe is generally divided into three subsegments: the Spiegel lobe, paracaval portion, and caudate process. Since these subsegments are supplied by separate vasculobiliary branch, theoretically each subsegment could be removed independently, which is the theoretical foundation of partial caudate lobectomy. 13 However, concerning tumor residue, complete caudate lobectomy appears more appropriate for tumors originating in the caudate lobe.
In practice, because of its deep anatomical location and complicated surroundings, caudate lobectomy is usually performed in combination with resection of adjacent lobe or transection of the liver parenchyma overlying the caudate lobe to obtain a clear exposure and a sufficient surgical margin. But for patients with chronic hepatitis and cirrhosis, the functional reserve and regenerative capacity of the remnant liver after hepatectomy are impaired compared with normal liver parenchyma. The combined resection may sacrifice overmuch innocent liver parenchyma and, therefore, put these patients at risk of postoperative liver failure. Thus, a good exposure of the operative area is considered as an essential step in the success of isolated caudate lobectomy.
The Arantius ligament, a fibrous remnant of the fetal ductus venosus, is located within the fossa between the left lateral lobe and the caudate lobe, travelling from the left portal vein to the IVC. 14 The tight connection between this ligament and the sheaths of the left portal pedicle provides conditions for using the Arantius ligament suspension to achieve good exposure of the left portal pedicle or even its left posterior surface. By this means, all the small branches of the left portal pedicle supplying the caudate lobe were more easily identified when the liver parenchyma was sectioned progressively.
Compared with open method, the laparoscopic approach could offer a unique viewing angle from below and the superior magnification and illumination could further increase visibility of this visually restricted area, which make laparoscopic isolated complete caudate lobectomy the most ideal oncological resection for tumors confined to the caudate lobe. Nevertheless, the operative area exposure is still unsatisfactory in laparoscopic isolated caudate lobectomy mainly because the laparoscopic fixed retractor couldn't raise the left lateral lobe liver sufficiently, especially a hypertrophic one. The drooping left lateral lobe could obscure the field of vision or repeatedly contaminate the lens. The Arantius ligament suspension technique described in this study could solve this problem very well without an additional port or an assisting hand, thus minimizing wounding and reducing the assistant's workload.
Additionally, to avoid slippage of the left lateral lobe, the left triangular ligament is usually preserved in this technique, which would benefit patients with liver cirrhosis because the dilated thin-walled collateral vessels in the peritoneal attachments are potential sources of intraoperative bleeding and causes of postoperative subphrenic fluid collection and ascites. During the operation, the short hepatic veins and IVC injury is a thorny problem, and it may cause massive hemorrhage and gas embolism, which are pretty difficult to handle even with the conversion to open surgery. Using our technique, the Spiegel lobe could be easily retracted upward and cranially to fully expose the short hepatic veins without the cover of left lateral lobe. Thus, we could dissect precisely and effectively control them from the left anterior of IVC to the right part. In practice, we usually prioritize dealing with these vessels in the surgical procedure, which effectively avoid the metastasis of tumor cells via them when we resected the hepatic malignancy of caudate lobe.
There are a few laparoscopic liver retraction techniques reported in the previous literature, but they all are designed for laparoscopic gastric surgery to obtain a good visualization of the gastrohepatic ligament and the stomach.15–20 Two of them are involved in liver puncture, which may increase risk of hemorrhage and additional hepatic injury in the present of underlying liver disease.15,16 One of them require the retraction device to be fixed on the pars condensa of the lesser omentum, 17 but to full expose the caudate lobe, the lesser omentum often need be divided in proximity to the Arantius ligament and the hepatoduodenal ligament firstly during laparoscopic caudate lobectomy. Shibao et al., 18 to retract left liver lobe for laparoscopic gastrectomy, proposed a system consisting of a leaf-shaped silicon disk placed under the lateral segment of the liver and elevated with a snake retractor under the disk. Compared with the Arantius ligament suspension technique in this study, the disk suspension technique needs an additional port placement, and the fixed retractor and disk may interfere with the operation of other surgical instruments when applied to laparoscopic caudate lobectomy. The Arantius ligament suspension technique allows us to rationally utilize the anatomical features of the liver, and avoids the shortcomings of the above techniques when used in laparoscopic caudate lobectomy. It should not only be suitable for laparoscopic caudate lobectomy, but also for other laparoscopic upper abdominal surgery needing left lateral lobe liver retraction.
In conclusion, laparoscopic isolated caudate lobectomy is a worthy alternative treatment method for the caudate lobe tumors. From our preliminary experience, the Arantius ligament suspension technique is quite simple and safe, and it could provide a satisfactory surgical field exposure without substantial mobilization or parenchymal transection of other liver lobes. Due to the small sample size and absence of case of tumor located in the caudate process in this study, more cases are required to further assess the feasibility and advantages of this technique.
Footnotes
Acknowledgments
The authors would like to thank the patients who participated in this study, and the medical staff involved in their care.
Disclosure Statement
No competing financial interests exist.