
Abstract
Abstract
Background:
Intercostal pleural drainage is standard practice after transthoracic esophagectomy but has some drawbacks. We hypothesized that a transhiatal pleural drain introduced through the subxyphoid port site incision at laparoscopy can be as effective as the intercostal drainage and may enhance patient recovery.
Patients and Methods:
A proof of concept study was designed to assess a new method of pleural drainage in patients undergoing hybrid Ivor Lewis esophagectomy (laparoscopy and right thoracotomy). The main study aims were safety and efficacy of transhiatal pleural drainage with a 15 Fr Blake tube connected to a portable vacuum system. Pre- and postoperative data, mean duration, and total and daily output of drainage were recorded in an electronic database. Postoperative complications were scored according to the Dindo-Clavien classification.
Results:
Between June 2015 and December 2016, 50 of 63 consecutive patients met the criteria for inclusion in the study. No conversions from the portable vacuum system to underwater seal and suction occurred. There was no mortality. The overall morbidity rate was 40%. Two patients (4%) required reoperation for hemothorax and chylothorax, respectively. Percutaneous catheter drainage for residual pneumothorax was necessary in 2 patients (4%) on postoperative day 2. The mean duration of drainage was 7 days (interquartile range [IQR] = 2), and the total volume of drain output was 1580 mL (IQR = 880). No pleural effusion on chest X-ray was detected at the 3-month follow-up visit.
Conclusions:
Transhiatal pleural drainage is safe and effective after hybrid Ivor Lewis esophagectomy and could replace the intercostal drain in selected patients.
Introduction
T
More than 10 years ago, we replaced the conventional 28 Fr Argyle tube with a 24 Fr Blake drain after transthoracic esophagectomy. Next, we switched to a 19 Fr Blake drain still connected to underwater seal and suction. 11 More recently, we hypothesized that transhiatal drainage of the pleural cavity may be as safe and effective as the traditional drainage.
Patients and Methods
We designed a proof of concept study to test the hypothesis that transhiatal pleural drainage is safe and effective after hybrid Ivor Lewis esophagectomy. Secondary study outcome was the efficacy of a portable vacuum system connected to the transhiatal drain. The study was deemed exempt by the IRCCS Policlinico San Donato Internal Review Board. The transhiatal drain consisted of a 15 Fr Blake® (Ethicon, Somerville, NJ) connected to a portable vacuum drainage system (J-Vac®; Ethicon). Criteria of exclusion from the study were preoperatively known bleeding disorders, perceived suboptimal intraoperative hemosthasis or difficult surgical dissection, the presence of extensive pleural adhesions, and/or air leakage at closure of thoracotomy. Routine antibiotic prophylaxis with cefazolin was given, and in most patients a thoracic epidural catheter was inserted before operation. Pneumoperitoneum was induced with a Veress needle and a five-port laparoscopic access was used to perform gastric mobilization, D2 supramesocolic lymphadenectomy, and lower mediastinal dissection. A 4 cm large gastric tube was formed by sequential firings of a linear stapler (Endo-GIA; Medtronic, Minneapolis, MA) starting with a 45 mm cartridge above the third branch of the right gastric vessels. The upper part of the stomach was left undivided. A 15 Fr Blake drain was advanced through the 5 mm subxyphoid port into the right pleural cavity until the multichannel segment of the tube was completely inside the chest cavity (Fig. 1).

Intraoperative image showing the Blake drain inserted through the subxyphoid port (arrow) at the end of the laparoscopic phase of the Ivor Lewis esophagectomy.
The second step of the operation consisted of a right posterior–lateral thoracotomy in the fifth interspace with sparing of the anterior serratus muscle. The arch of azygos vein was divided, and the esophagus was mobilized en bloc with the mediastinal pleura and the periaortic lymphoadipose tissue up to the diaphragm. The thoracic duct was routinely ligated. Lymphadenectomy of the low paratracheal and tracheobronchial nodes was performed, and the vagal branches supplying the airways were preserved whenever possible. The gastroesophageal junction was retrieved in the chest along with the preformed gastric tube, and an end-to-side esophagogastric anastomosis was performed at the apex of the chest using a 25 mm circular EEA stapler (Medtronic). The gastric tubulization was completed using the endo-GIA stapler. The active part of the Blake drain crossing the hiatus was placed with the tip at the level of the third intercostal space. After complete lung recruitment, the drain was connected to the portable J-Vac. The system was checked every 3 hours for the first 24 hours to ensure that the bellow was fully charged to guarantee stable lung expansion. Postoperative pain management, in addition to thoracic epidural analgesia, consisted of remifentanil on postoperative day 1, and acetaminophen and ketorolac on the following days as needed.
Pre- and postoperative data were recorded in an electronic database. Postoperative complications were scored according to the Dindo-Clavien classification. 12 The efficiency of the drainage system was assessed by recording the presence of subcutaneous emphysema on the chest wall and/or neck, the frequency of vacuum loss in the J-Vac and/or switch to underwater seal with or without suction, the presence of residual pneumothorax on a standard chest radiography or CT scan, the daily and the total volume of fluid drainage, and the duration of drainage. The need to place additional pleural drains was also recorded. A chest X-ray was performed immediately after operation and on days 1, 3, and 6 (Fig. 2 and Fig. 3). In eligible patients, the nasogastric tube was removed on postoperative day 3 and clear liquids per os were allowed according to our fasttrack protocol. The epidural catheter was removed on postoperative day 4. A gastrographin swallow study was performed on postoperative day 5 and patients were then allowed a soft diet. A chest X-ray was obtained before hospital discharge. Patients were scheduled for a follow-up visit including a chest X-ray 3 months after the operation.

Chest X-ray on postoperative day 3. Arrows indicate the entry of the Blake drain in the right pleural cavity and the tip of the drain in the upper chest.

Portable pleural drainage system consisting of a 15 Fr transhiatal Blake drain connected to a J-Vac close circuit.
Results
The study was performed between June 2015 and December 2016. During the study period, 63 patients underwent a hybrid Ivor Lewis esophagectomy. In 50 patients, the right pleural cavity was drained with a single transhiatal Blake tube. Thirteen patients were excluded from the study due to air leakage from the lung at the time of thoracotomy closure (n = 6), perceived unsatisfactory hemostasis (n = 4), or both (n = 3). In these individuals, an additional intercostal drainage (19 or 24 Fr Blake) was placed at surgeon's discretion.
The demographics and clinicopathological data are shown in Table 1. No intraoperative complications occurred, and the median operative time was 300 minutes (interquartile range [IQR] 74). The transhiatal drain was connected to the J-Vac bag in all patients at the end of the surgical procedure after lung recruitment. There was no need to switch from J-Vac to underwater seal and suction in none of the patients, and no loss of vacuum occurred after a median of three (IQR = 1) recharges of the J-Vac. There was no hospital mortality, and the overall morbidity rate was 40%. Grades 3–4 complications occurred in 9 patients, and a reoperation was necessary in 2 (1 hemothorax requiring redo thoracotomy 8 hours after the primary procedure, and 1 chyle leakage requiring thoracoscopic duct ligation on postoperative day 4). Two patients with persistent pneumothorax required percutaneous catheter drainage on postoperative day 2. One patient had persistent gastric outlet obstruction possibly related to kinking of the Blake drain at the hiatus: drain removal at the time of the gastrographin swallow study resulted in immediate relief of obstruction (Table 2). The transhiatal drain was removed after a median time of 7 days (IQR = 2). The daily drainage output is shown in Figure 4. The median volume of drain output decreased <300 mL after postoperative day 2, and remained <200 mL after postoperative day 6. The median of total volume of fluid drained was 1580 mL (IQR = 880). The median hospital stay was 9 days (IQR = 3). One patient was readmitted 35 days after discharge due to severe nutritional impairment and minimal bilateral pleural effusion not requiring drainage. At the follow-up visit 3 months after discharge, no pleural effusions were detected on the chest X-ray. Fourteen patients (28%) reported occasional use of paracetamol or nonsteroidal antinflammatory drugs for residual pain at the thoracotomy site.
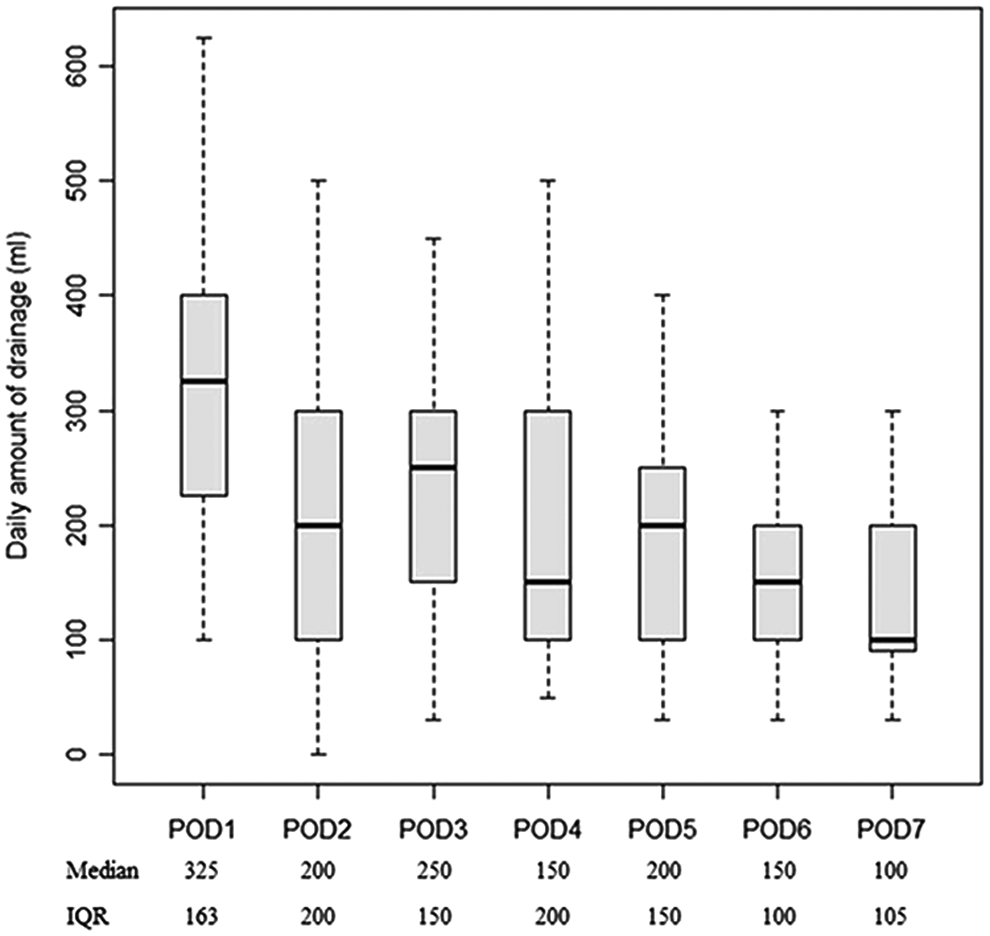
Median daily volume output of pleural fluid.
BMI, body mass index; IQR, interquartile range; pred, predictive.
Discussion
The main finding of this study is that a transhiatal pleural drain may safely replace the conventional intercostal drain after hybrid Ivor Lewis esophagectomy. The transhiatal pleural drainage has a number of potential advantages over the intercostal drain: (1) it consists of a smaller size and shorter Blake tube independent from underwater seal; (2) it is connected to a portable 450 mL J-Vac bag that is easily carried by the patient and fits into a jacket pocket; (3) it allows earlier ambulation and facilitates physiotherapy and nursing care; (4) no purse-string suture nor Valsalva maneuver is required at the time of drain removal. Although the one-way flutter valve prevents intrapleural reflux of air or fluid, the efficiency of the aspiration and the level of fluid drained should be checked at regular intervals, especially during the first 24 hours, to ensure optimal lung re-expansion by repeat charging of the bellow. If necessary, the J-Vac should be emptied more than once a day because of its limited capacity. This study also confirms that routine underwater seal drainage is not necessary after transthoracic esophagectomy. 13
A decade ago, the use of a large (28 Fr) transhiatal chest drain was reported in a series of 32 patients undergoing open transthoracic esophagectomy. 14 Pleural effusion requiring percutaneous drainage under ultrasound guidance occurred in 12.5% of cases, and drain displacement in 3.1%. In our study, transhiatal drainage was performed through the same port site incision used for the laparoscopic phase of the Ivor Lewis esophagectomy. The 15 Fr Blake drain was safe and adequate. A specific, although mild, complication of this method of pleural drainage was gastric outlet obstruction due to possible kinking of the Blake drain around the gastric tube across the hiatus. Since then, we have learned to keep the drain a little loose around the left liver lobe and to avoid excessive pulling up in the chest cavity.
The role of chest drainage after transthoracic esophagectomy has been mainly discussed with regard to the occurrence of anastomotic complications or chylothorax, and little information is available about the expected volume of fluid and duration of pleural drainage. Lagarde et al. 15 found that the median total output was about 2.5 L, and 43% of their patients needed chest drainage for >7 days. Prolonged chest drainage was associated with a transthoracic approach, a greater blood loss, a higher number of resected lymph nodes, and a radical dissection, perhaps indicating that prolonged drainage is a sign of adequate surgical dissection. In contrast, it has been shown that prolonging the duration of pleural drainage may not be necessary in most patients since using the 300 mL threshold for drain removal does not increase the necessity of repeat drainage or hospital readmission. 16 In contrast to pulmonary surgery, wherein the presence of a residual space requires evacuation of fluid and air without resistance, the impairment of lymphatic drainage in esophageal surgery is self-limiting and is compensated by the absorptive capacity of the pleura. Excess fluid evacuation should probably be avoided because pleural fluid drains, primarily through parietal pleura lymphatics, at a rate of 500 mL/day for each hemithorax. 17 In our patients, the median total fluid output was 1580 mL; the median drain output decreased <300 mL after postoperative day 2, indicating that early drain removal is safe after hybrid Ivor Lewis esophagectomy.
Our method of pleural drainage differs from other studies since we used a 15 Fr transhiatal drain connected to a portable vacuum apparatus. Niwa et al. 18 described an original method of bilateral intercostal pleural drainage using a single 15 Fr Blake tube inserted into the right chest and advanced to the left pleural cavity across the posterior mediastinum. The drain was managed underwater seal, the total output was higher than the conventional 19 Fr tube, and none of the patients developed a left pleural effusion.
Use of a mobile vacuum system connected to an intercostal drain after esophagectomy was first described by Law et al., 19 as a viable alternative to underwater seal. The overall success rate was 94%, and outcomes were no different from that of an historical cohort of patients treated with conventional underwater drainage. We found the J-Vac system very efficient, since a few bellow recharges were needed to obtain full lung expansion and there were no instances of conversion to underwater seal. The fact that we limited this approach to patients with no coagulation disorders, no intraoperative technical difficulties, no pleural adhesions, and/or air leakage at closure of thoracotomy may explain the low rate of complications in this series.
Conclusions
A pleural drain placed through the upper abdominal port site after hybrid Ivor Lewis esophagectomy can safely replace the traditional intercostal tube and provide a similar daily fluid output. However, we recommend to place an additional intercostal Blake drain in patients with bleeding disorders, perceived difficult surgical dissection or suboptimal hemostasis, and/or air leakage at closure of thoracotomy. The transhiatal drainage connected to a J-Vac system has also the potential to cause less postoperative discomfort, reduce analgesic requirements, and promote early ambulation and hospital discharge.
Footnotes
Acknowledgment
This work was supported by Associazione Italiana Ricerca Esofago (AIRES).
Disclosure Statement
No competing financial interests exist.