
Abstract
Abstract
Background:
Peroral endoscopic myotomy (POEM) has become an acceptable incisionless treatment for achalasia based on encouraging outcomes in multiple series worldwide. This report reflects our early experience.
Methods:
Data were collected prospectively on all patients undergoing POEM between June 2011 and April 2016 under IRB approval. Diagnosis of achalasia was confirmed by standard preoperative work-up. Primary outcome was symptom relief, measured by Eckardt score. Secondary outcomes were operative time, length of stay (LOS), adverse events, failure, and recurrence.
Results:
Fifty patients were included; 30 were female. Mean age was 55.7 ± 17.7 years. Mean BMI was 29.5 ± 9.2. Median OR time was 133.5 minutes (range 70–462); average myotomy was 13.1 ± 2.3 cm. One early case was converted to a laparoscopic Heller myotomy due to extensive submucosal fibrosis from a recent Botox injection. Two cases were aborted; one due to extensive submucosal fibrosis and the other to intraoperative capnopericardium. Median LOS was 1 day (range 0.8–8). Two major complications occurred: intraoperative cardiac arrest due to capnopericardium and postoperative submucosal hemorrhage. There were no deaths. Mean postoperative Eckardt score was 1.0 ± 1.9 (range 0–8) at 2–6 weeks (vs. preoperative score 7.7 ± 2.8; P < .0001); mean dysphagia component 0.35 ± 0.28 (vs. preoperative score 2.6 ± 0.7; P < .0001). Two recurrences were identified, both at 6 months.
Conclusions:
POEM is a safe and durable treatment for achalasia in the short term. We demonstrated marked improvement of symptoms in all completed cases. There was an acceptable serious adverse event rate of 4%, failure of 6% due to patient selection, and recurrences occurring in only 4% of cases.
Introduction
A
Natural orifice translumenal endoscopic surgery™ (NOTES) is a developing field of surgery in which target organ access is gained across the lumen of a hollow viscus such as the esophagus, stomach, rectum, bladder, or vagina. The early human experience of NOTES procedures focused mainly on cholecystectomy, performed through either a transgastric or transvaginal approach, using either a flexible endoscope or standard laparoscopic instrumentation. Per-oral endoscopic myotomy (POEM), initially described by Ortega et al. 9 and popularized by Inoue et al., 10 represents an approach to the circular muscle layer of the esophagus via the mouth utilizing a flexible endoscope. Based on principles learned from endoscopic submucosal dissection (ESD), and congruent with the development of endoscopic surgical techniques in NOTES procedures, POEM allows direct access to the circular layer of the esophagus without extraluminal dissection. Compared to a LHM, POEM is incisionless, does not enter the abdominal cavity, and has been shown by many studies to have reduced postoperative hospital stay and recovery time. 11 We report our initial experience with fifty patients who underwent POEM.
Methods
The first POEM performed by our multidisciplinary team in a human patient was in June 2011. Our team consists of one minimally invasive surgery (MIS) general surgeon, and two gastroenterologists, specialty trained in advanced interventional gastroenterology. The general surgeon has been in practice for 16 years, with 12 of those years involved in the development and clinical practice of developing less invasive operations, including NOTES procedures, single-port laparoscopic surgery, and endoscopic surgery in porcine models and human patients. The senior gastroenterologist has been performing advanced therapeutic endoscopy for 17 years, with 11 years of NOTES research in swine. The junior gastroenterologist has been in advanced therapeutic endoscopy practice for 7 years and has been performing POEM procedures with our team for over 2 years.
Our team had begun animal research in 2005 in NOTES procedures and physiology. By 2011, we had performed over 50 animal experiments, including work on NOTES techniques, including five porcine POEMs based on the description of the technique by Inoue et al. 10 Our human NOTES experience began with pancreatic pseudocystgastrostomy in 200712 and with transvaginal cholecystectomy in 2009. We then visited Professor Inoue at Showa University Northern Yokohama Hospital in Yokohama, Japan in January 2011, where our team observed five human POEM cases. We continued performing animal experiments while awaiting Institutional Review Board (IRB) approval of a human protocol for our first 25 procedures, which was subsequently modified to an ongoing data repository for POEM cases.
Patient selection
All patients over 18 years of age offered a POEM for achalasia at our institution between June 2011 and April 2016 agreed to undergo informed consent and to enroll in our IRB-approved protocol. All patients underwent preoperative upper gastrointestinal contrast study, upper endoscopy, and esophageal manometry to confirm their diagnosis.
Operative technique
Patients were placed under general anesthesia with endotracheal intubation. A standard gastroscope was inserted (Olympus GIF 180 or 190) and CO2 insufflation was initiated (Olympus America, Center Valley, PA). Many patients had undigested food particles and pooled secretions present in the esophagus, which were suctioned away or pushed into the stomach with the tip of the endoscope until the esophageal lumen was cleared of debris. The endoscope was passed into the stomach through the gastroesophageal junction (GEJ) in all patients and the location of the GEJ was noted. A minimum of a 10-cm myotomy was the goal in all patients, with at least a 2-cm portion distal to the GEJ, although in later cases the high-resolution esophageal manometry (HREM) results dictated the length of the myotomy. The mucosal tunnel was planned proximal to the start of the myotomy, running at least 5 cm in length.
The preferred site for mucosal incision was on the anterior esophageal wall, except in patients with prior Heller myotomy, in which case a posterior approach was chosen. A submucosal cushion was created by injecting saline mixed with indigo carmine dye as described by Inoue. 1 A sclerotherapy needle (Boston Scientific, Natick, MA) or with the injecting mechanism of the Erbe Hybrid Knife® (Erbe USA, Marietta, GA) was used for this purpose (Fig. 1a). Using either the triangle-tip (TT) knife (Olympus America), or the Hybrid Knife, the mucosa over the saline cushion was opened with monopolar cautery (Erbe Electrosurgical Generator, Marietta, GA, set on 50 watts) (Fig. 1b). The tip of the endoscope was fitted with an endoscopic cap, beveled to 30 degrees (Olympus America), with the elongated end positioned toward the mucosa. The TT Knife (or Hybrid knife) was extended beyond the end of the cap, and “spray coag,” “endo cut,” or “dry cut” mode (50–70 watts), was used to dissect through the submucosa to the level of the easily visualized circular muscle fibers, which are typically very prominent in achalasia. The submucosal tunnel was extended distally, continuing the dissection as close to the muscle fibers as possible so as to leave the maximum amount of submucosa adherent to the mucosa (Fig. 1c). The cap-fitted endoscope tip was bluntly maneuvered into the submucosal tunnel with the long edge of the angled cap abutting the mucosa, so as to protect it from thermal injury. The space was continually distended with repeated injections of blue-dyed saline and the submucosal tunnel was dissected with “spray coag” or “dry cut” to the level of the GEJ. At this point, the dissection often became difficult, with narrowing or disappearance of the submucosal plane, and with disorder of the previously uniform circular smooth muscle (Fig. 1d). The tunnel was extended another 2–3 cm onto the anterior surface of the stomach. Hot biopsy forceps were used to cauterize the larger crossing vessels, especially near the GEJ, where there is increased vascularity and greater potential for bleeding during dissection. The disordered appearance of these palisading vessels also serves as an important anatomic landmark. The endoscope was then withdrawn from the tunnel and returned to the true lumen (Fig. 1e). We entered the stomach and retroflexed the endoscope to examine the hiatus, specifically to confirm that blue dye was visible through the mucosa of the stomach, indicating the dissection proceeded sufficiently distal to the GEJ (Fig. 1f).
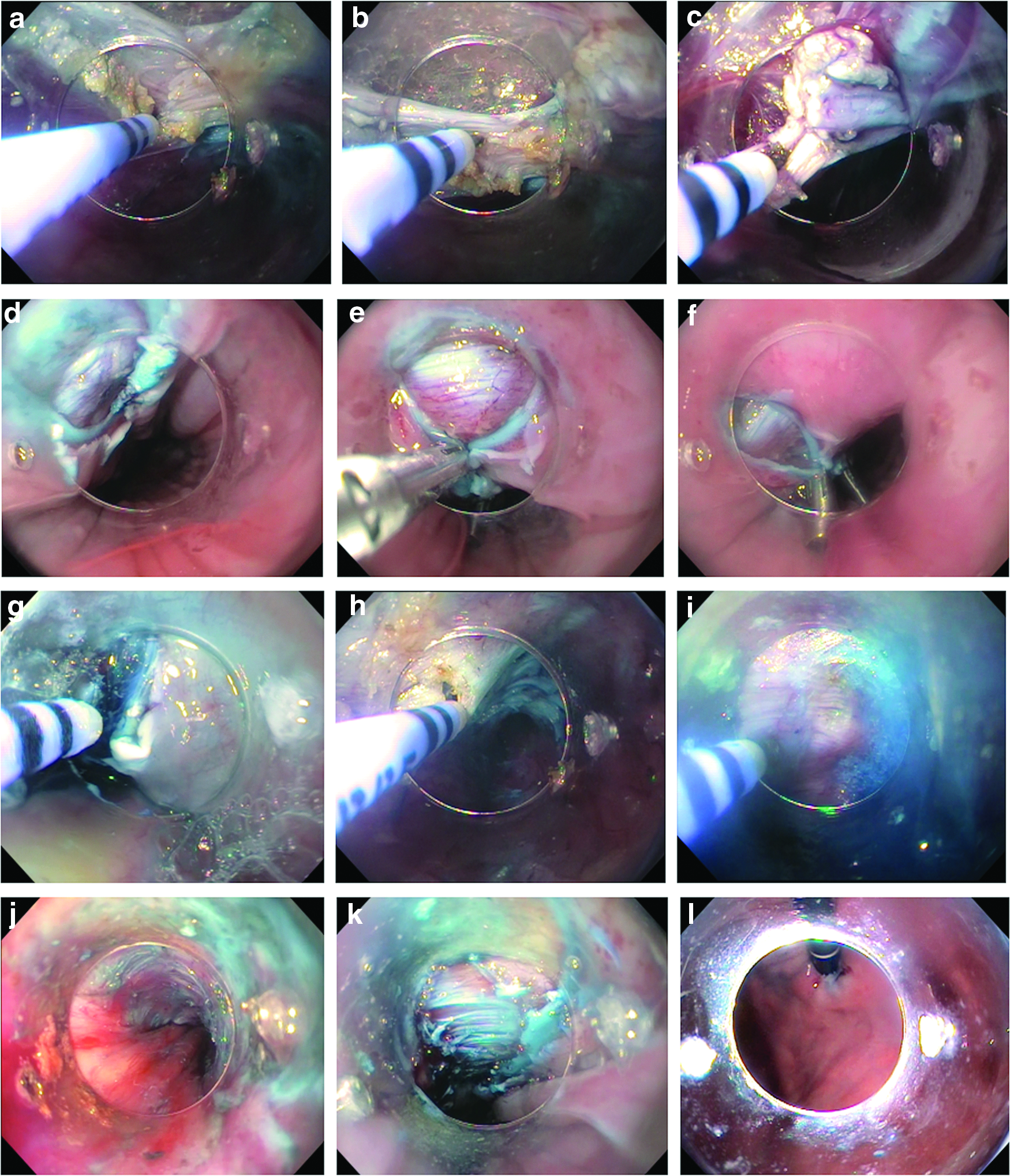
Once confirmed that the submucosal tunnel was extended adequately onto the stomach, the myotomy was initiated. Typically, the myotomy was performed using either the TT Knife or the Hybrid Knife in the proximal-to-distal direction (Fig. 1g). However, in some cases, we performed the myotomy in the distal-to-proximal direction (Fig. 1h). We found this approach more difficult to remain in the proper anatomic plane. We have also started the myotomy in an antegrade-fashion, starting with the GEJ, and then have performed a second antegrade myotomy from the desired start point to the GEJ. Though the longitudinal muscle fibers were not intentionally divided, the advancement of the scope has a tendency to disrupt them, and the circular fibers retract when cut, also pulling the longitudinal fibers apart. At times, the plane between the circular and longitudinal layers becomes hard to distinguish, and both layers must be divided together, producing a full-thickness dissection (Fig. 1i). When this occurs, patients may develop pneumoperitoneum, and a portion of these cases may require Veress needle placement for decompression. Although the esophagus does not have a serosal layer per se, adherent mediastinal tissues prevent gross capnomediastinum when this space is entered.
At this point, gentamicin 80 mg in 60 cc saline was injected through the working channel of the endoscope to fill the submucosal tunnel. The esophageal mucosa was closed using either Olympus QuickClip™ (Olympus America), Resolution™ clips (Boston Scientific, Natick, MA) or Cook Instinct™ clips (Cook Medical, Winston-Salem, NC) (Fig. 1j–l).
Data collection
Data were collected prospectively in a surgeon-maintained registry. Some follow-up data were obtained by retrospective chart review to ensure that the reported outcomes were up to date at the time of article submission. Demographic data, including achalasia type, imaging for diagnosis, previous endoscopic or surgical achalasia treatment, and preoperative symptoms, were collected for all patients. Eckardt scores were available from the initial clinic visit for all patients, except for the first two patients in the series who had been seen before our implementation of the Eckardt score. Primary outcome was symptom resolution, as measured by pre- to postoperative Eckardt score. Other outcomes included location of the GEJ, location of the mucosotomy, locations of the start and end of the myotomy (giving total myotomy length), whether the myotomy was performed on the anterior versus posterior or lateral esophageal wall, number of clips used for closure, whether a patient experienced pneumoperitoneum and required Veress needle decompression, operative times, conversion rate, complications, length of stay (LOS), length of follow-up, recurrence, and treatment failure.
Statistical analysis
Descriptive analyses were reported as percentages for categorical variables and as mean ± standard deviation or median with range for quantitative variables. Univariate comparisons for pre- to postoperative Eckardt score were performed using Wilcoxon signed-rank tests and comparison of operative times between early and late cases with Wilcoxon rank-sum tests. These analyses were executed on Graphpad Prism 6.0 (Graphpad Software, Inc., La Jolla, CA). Operative time learning curve was investigated using regression models and cumulative sum analysis. Both piecewise and simple linear regression were utilized to determine the overall trend and any potential inflection point(s) in the OR time learning curve over the life of the study. A cumulative sum (CUSUM) chart was then produced to better identify subtle changes in OR time trends as surgeon experience increased, with a downward slope indicating better than target OR time performance. Target OR time was set to 140 minutes, a value slightly less than the mean OR time following an operative device change early in the study. Analysis of variance, with Tukey's Studentized Range Test, was used to compare mean operative times at different stages of the learning curve identified by the CUSUM chart. Learning curve analysis was performed using SAS v9.4 and R v3.2.3.
Results
Between and June 2011 and April 2016, 50 patients underwent POEM, with 47 completed successfully. Thirty (60%) were female. All but three patients carried the diagnosis of achalasia (10 with type I, 29 with type II, 6 with type III, and 2 who did not fit into a specific classification); one patient had nutcracker esophagus, one had diffuse esophageal spasm, and one was diagnosed retrospectively with scleroderma. The mean age was 55.79 ± 17.7 years and the mean BMI was 29.7 ± 9.2. The mean preoperative Eckardt score was 7.8 ± 2.8 (range 1–12), with mean dysphagia component of 2.6 ± 0.72 (range 0–3). Forty-nine patients presented with dysphagia, 30 with regurgitation, 24 with chest pain, 19 with weight loss, and 1 with aerophagia. Of the 50 patients, 7 (14%) patients had intramuscular botulinum toxin injection preoperatively, ranging from 10 days to 4 years before presentation, and 22 (44%) had previous endoscopic dilations. Eight patients had undergone previous surgical treatment for achalasia; all of these had been a Heller myotomy with either Toupet or Dor fundoplication (Table 1).
BMI, body mass index; IM, intramuscular.
The average myotomy length was 13.1 ± 2.3 cm. The mucosal incision was made on the anterior esophageal wall in 45 patients, 5 were made on the posterior esophageal wall, and 1 was made laterally. Both an anterior and a posterior myotomy was created for one patient who had undergone a previous failed Heller myotomy, resulting in fibrosis and thus, a submucosal plane was unable to be identified. Posterior wall myotomy was the preferred approach in patients who had undergone previous Heller myotomy to avoid encountering previously disrupted surgical planes. The patient who underwent reoperation with a POEM had a posterior tunnel creation and myotomy. The average number of clips for mucosal closure was 4.3 ± 2.1. In the first seven cases, between 7 and 12 clips were needed to close the mucosal opening. In more recent cases, this number decreased to three or four clips (Table 2).
Of 29 full-thickness dissections noted through muscular layers, 17 patients developed intraoperative pneumoperitoneum, 12 were decompressed by Veress needle, and none suffered further sequelae. One case (#8) was converted to a LHM due to botulinum toxin injection at an outside institution 10 days before the procedure, concealed by the patient and not known to us at the time of her POEM. This caused an intense scarring reaction in the submucosal space such that the submucosa could not be expanded with saline injection, and so the tunnel could not be created without undue risk of mucosal injury. Two cases had to be aborted, one (#40) due to extensive submucosal fibrosis from a previous LHM. The other aborted case (#18) occurred due to inadvertent tension capnomediastinum, causing cardiac tamponade and cardiopulmonary arrest, requiring cardiopulmonary resuscitation. 13
Mean operative time, as measured from the beginning of the endoscopy to the withdrawal of the endoscope, was 150 minutes (median 133.5 minutes; range 70–462). The high outlier (462 minutes) was the one case that was converted to an open procedure due to extensive submucosal fibrosis. After the fifth case, we changed the operative device from the Olympus TT knife to the Erbe Hybrid Knife, which allowed for simultaneous injection and cautery without the need to change instruments. Our mean time in the first five cases was 225.4 ± 26.2 minutes, while the mean time of the subsequent five cases with the new instruments, excluding the case converted to open procedure, was 142.4 ± 15.7 minutes (P = .0003) and the last five cases was 130 ± 10.5 minutes (P < .0001).
Operative times were found to have a decreasing trend over the life of the study. Piecewise regression identified a potential inflection point in the operative times after October 2014 (case #15); as expected, shorter OR times were seen as procedures became more frequent. However, a simple linear regression model showed a better fit for the data (Fig. 2). Cumulative Sum (CUSUM) chart analysis provided a more detailed look at the operative time trend (Fig. 3). We observe an initial period that included a change in operative device (from a sclerotherapy needle to hybrid knife) and one procedure conversion (mean operative time 198 ± 88 minutes). A second period, corresponding with a sharp increase in the frequency of procedures, began at Case #15. This phase demonstrated an overall decreasing, yet still somewhat variable, trend in the operative time (mean 136 ± 37 minutes). Starting at Case #39, we observe a final stage where operative time shows much less variation (mean 121 ± 16 minutes). ANOVA results indicate a shift in mean operative times over these different stages (P = .001). Stages 2 and 3 both have significantly lower mean operative times than Stage 1 (Tukey's Studentized Range Test at the 0.05 level). Stages 2 and 3 do not have significantly different mean operative times compared with each other, but there is a notable decrease in variability in Stage 3 (with a much smaller standard deviation) compared to Stage 2 (Fig. 4).
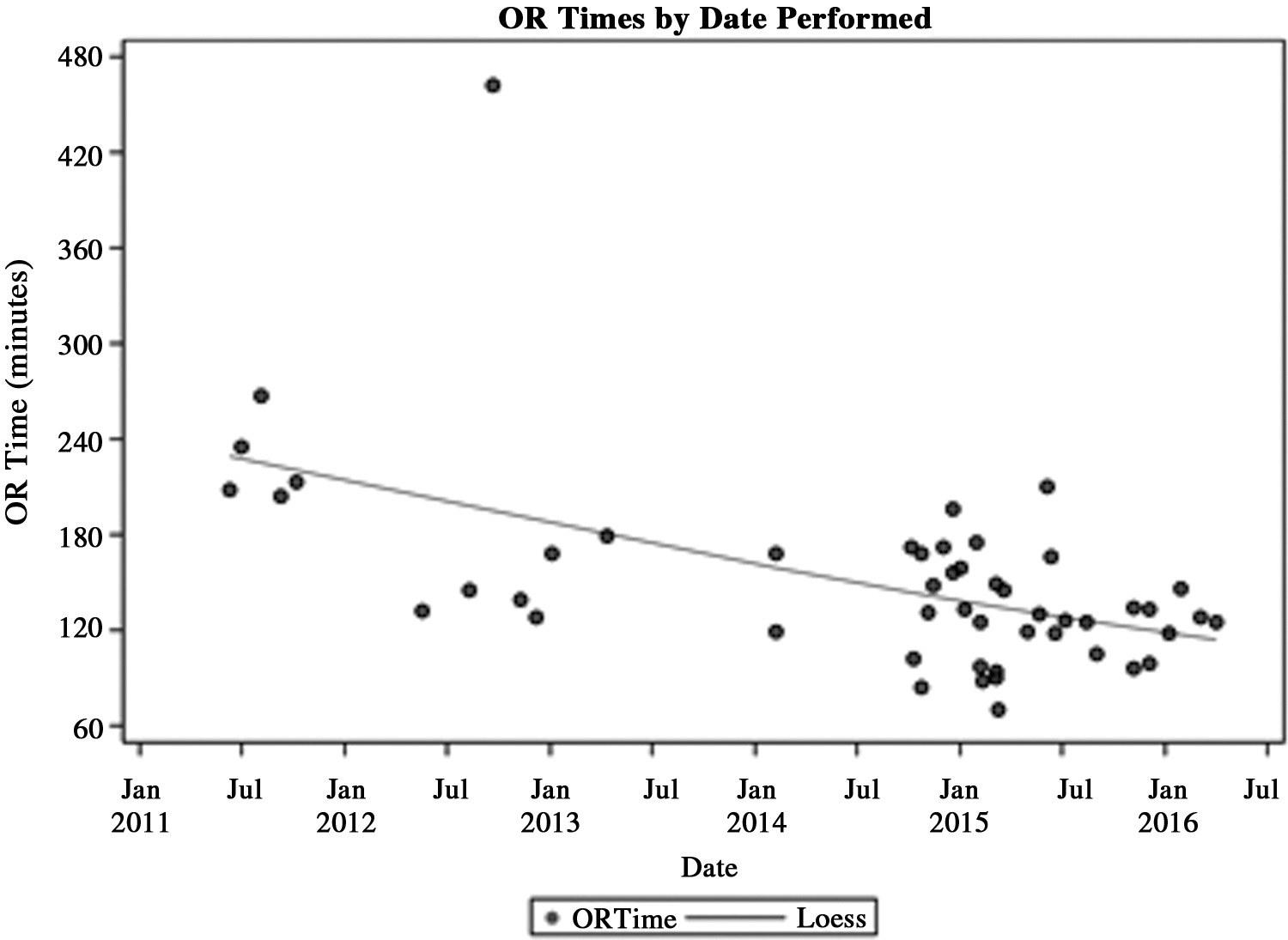
OR times by date. Piecewise regression identified a potential inflection point of shorter OR times as procedures became more frequent, after October 2014 at Case #15.
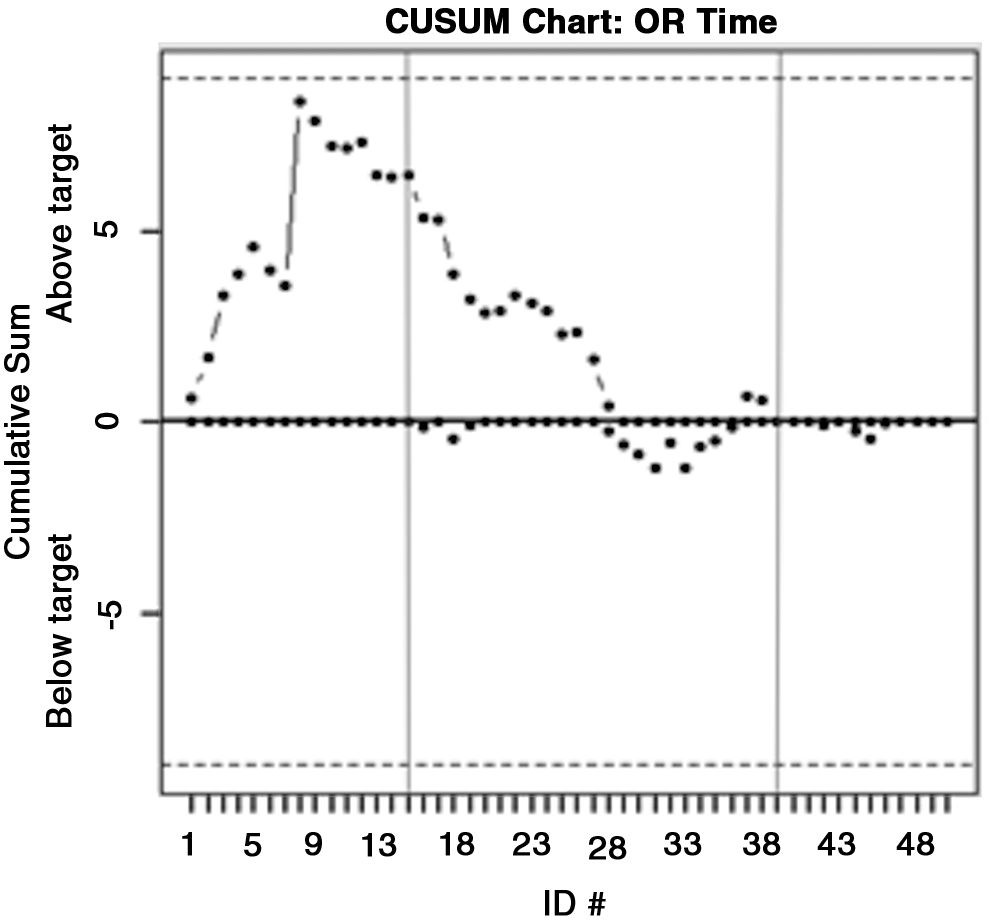
CUSUM chart. Displays the cumulative sums (CUSUMs) of the deviations of each patient's operative time from a target operative time of 140 minutes (point between the mean and median). Here, we see a rise over the first 8 cases then, leveling-off. Starting with Case #15, the procedures were performed more frequently and we observe a downward trend and eventual stabilization at Case #39. Each point is based on information from all cases, up to and including the current case.
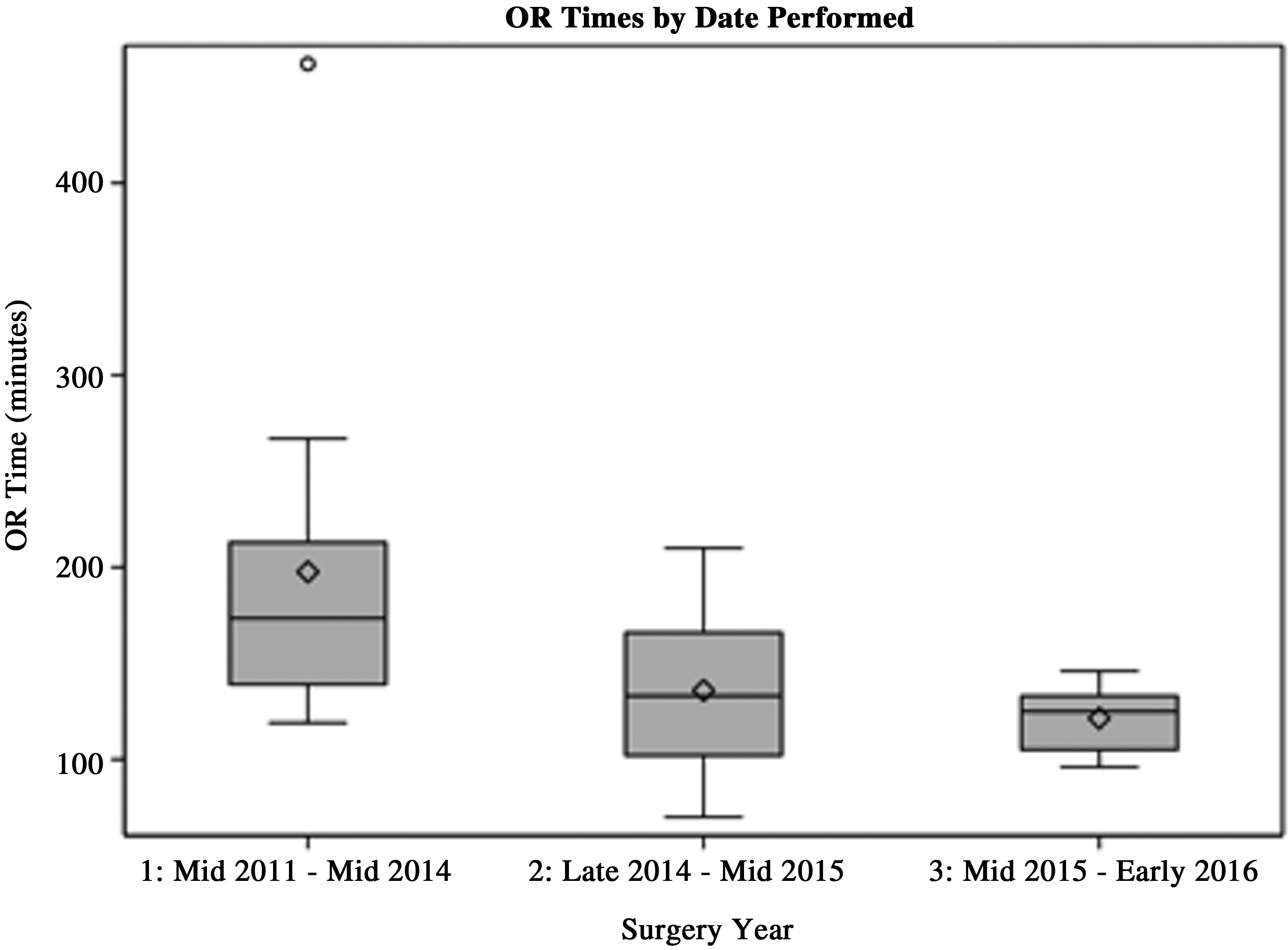
OR times by Stage. Stage 1 corresponded with a change in operative device, one procedure-conversion, and the first surgeries performed with the new knife (mean operative time 198 ± 88 minutes). A second stage, corresponding with a sharp increase in the frequency of procedures (Cases #15–38), demonstrated an overall decreasing trend in the operative time (mean 136 ± 37 minutes). The third stage demonstrated operative time with less variation (mean 121 ± 16 minutes). The difference in operative times between these stages are significant using ANOVA (P = .001). Stages 2 and 3 both have significantly lower mean operative times than Stage 1 at the 0.05 level (Tukey's Studentized Range Test). Stages 2 and 3 do not have significantly different mean operative times compared with each other, but there is a notable decrease in variability.
Mean LOS after POEM was 1.6 ± 0.7 days (median 1.0 day; range 0.8–8). Patient #8, who underwent conversion to a LHM, had a prolonged stay (5 days), as did the patient with capnopericardium (8 days). When these patients are excluded, mean LOS was 1.3 ± 0.7 days.
The first 10 patients underwent upper gastrointestinal contrast studies on postoperative day 1. None revealed a contrast leak. Notably, the radiology reports from some of the studies cited little change in the measurements of the GEJ narrowing length and/or diameter despite gross improvement in the patients' symptoms. As the results of these studies did not alter the team's management decisions for these patients, a postoperative esophagram was thereafter only obtained if there was a clinical suspicion of a leak or other concern.
Median follow-up was 8.14 weeks (range 11 days to 51 weeks), though mean follow-up was 28.3 weeks. All but 1 patient (#39) reported complete or near-complete resolution of symptoms. Patient #39 had disease that was also refractory to previous dilations and LHM. Mean postoperative Eckardt score was 1.0 ± 1.9 (range 0–8) at 2–66 weeks (P < .0001, compared with preoperative score of 7.7 ± 2.8), with mean dysphagia component 0.35 ± 0.63 (P < .0001, compared to preoperative score of 2.6 ± 0.7) (Table 3).
Paired t-test comparing pre- and postoperative results.
There were no deaths. There was one intraoperative complication: the development of capnopericardium with subsequent cardiac arrest that required CPR and prolonged intubation, which resulted in an overnight ICU stay for ventilation and a self-limited episode of atrial fibrillation. 13 A contrast esophagram performed on postoperative day 3 was negative for extravasation into the mediastinal tunnel or pericardial space and he was discharged on day 8 without any cognitive deficits. On short-term follow-up, he did report near complete resolution of his preoperative achalasia symptoms with only the mucosal tunnel and a short segment of the proximal myotomy completed. However, he later recurred with symptoms and went on to have an LHM 9 months later. One major postoperative adverse event, traumatic hemorrhage into the submucosal tunnel, occurred within 1 week of discharge due to the patient's choice of doughy ethnic food consumption swallowed whole, against medical advice.
Two patients had delayed failure (#1 and #3) with modest improvement for a short time, but required further surgery and/or dilatation for symptom relief. Patient #3 required a percutaneous gastrostomy tube for nutrition, which was removed after subjective improvement from a series of dilatations. Two recurrences were identified, both at 6 months. Patient #2 was found to have a GEJ stricture on esophagram; however, this is likely due to a peptic stricture. Patient #22 suffered upper esophageal spasm and was treated medically. Ten patients reported either ongoing or new reflux symptoms at the time of follow-up; all of which were controlled with medication.
Discussion
While endoscopic myotomy was reported in 1980, 9 the procedure became popularized by the animal work performed by Pasricha et al., 14 Sumiyama et al., 15 and Perretta et al., 16 in addition to the early human reports of Inoue starting in 2008.2,10,11 After Inoue initially reported his series of 17 patients, 9 subsequent reports have included 43 patients 17 to 500 patients 18 with excellent short- and long-term results, and minimal morbidity. Inoue and colleagues recently published technical recommendations after completing their thousandth patient. 19 Their series of 500 patients, the largest to date, demonstrated 91.3% efficacy at 2 months (mean reduction in Eckardt score from six preoperatively to one postoperatively), 91.0% at 1–2 years (mean Eckardt 1), and 88.5% at 3 years (mean Eckardt 1). 18 Another study, which describes outcomes up to 2 years postoperatively, 20 reported high efficacy in a series of 205 patients across 10 tertiary care centers. Efficacy was 98% at 6 months, 98% at 1 year, and 91% at 2 years, with overall decrease in Eckardt from 6.6 to 1.4. Their overall failure rate (or Eckardt >3) was 8.8%, with prior pneumatic dilation as a significant predictor of treatment failure. The recurrence rate was 6%, without any significant predictors.
A comprehensive meta-analysis by Talukdar, published in 2015, evaluated 29 studies with a total of 1045 patients (series ranged from 3 to 243 patients) between the years of 2007 and 2013. 12 This meta-analysis confirmed the efficacy of POEM in achalasia treatment and demonstrated similar outcomes to LHM using symptom reduction by Eckardt score, LES pressure, postoperative pain score, analgesia use, LOS, and adverse events as indicators. Effect size was −5.99 for Eckardt score and −5.39 for LES pressure. As expected, they demonstrated significantly shorter operative time for POEM compared to LHM.
Compared to the previously published series, our outcomes are comparable for operative time, myotomy length, symptomatic improvement (Eckardt score), LOS, length of follow-up, and postoperative reflux symptoms (Fig. 5). Attempting to compare complication rates across series is problematic given that the definitions of what constitutes a complication has evolved with further experience performing POEM. Initially, full-thickness dissections with pneumoperitoneum or pneumomediastinum and cervical emphysema not requiring intervention were categorized as minor complications. 21 More recently, these adverse events have been reclassified as important considerations during the procedure given that intervention may be needed if they occur, but do not necessarily add morbidity. 22 Furthermore, we initially considered inadvertent distal mucosotomy repaired by clip placement as a minor complication. These injuries have not resulted in any adverse events at our center, and are reported as common occurrences by other studies, with some centers reporting that it is not necessary to close them. 22 Incidence of mucosal injury is reported to be 48.7% across studies. 23 Reported complication rates range from 0% to 60% due to the variability of inclusion of pneumoperitoneum and mucosotomy as complications.23–30 For example, Zhou et al. 25 initially described their experience after 42 patients in Shanghai with no major complications through short-term follow-up. They later published a series of 119 patients who underwent POEM over a span of 9 months 26 with much higher complication rates; 25% of patients experienced a pneumothorax and 23% experienced cutaneous emphysema.
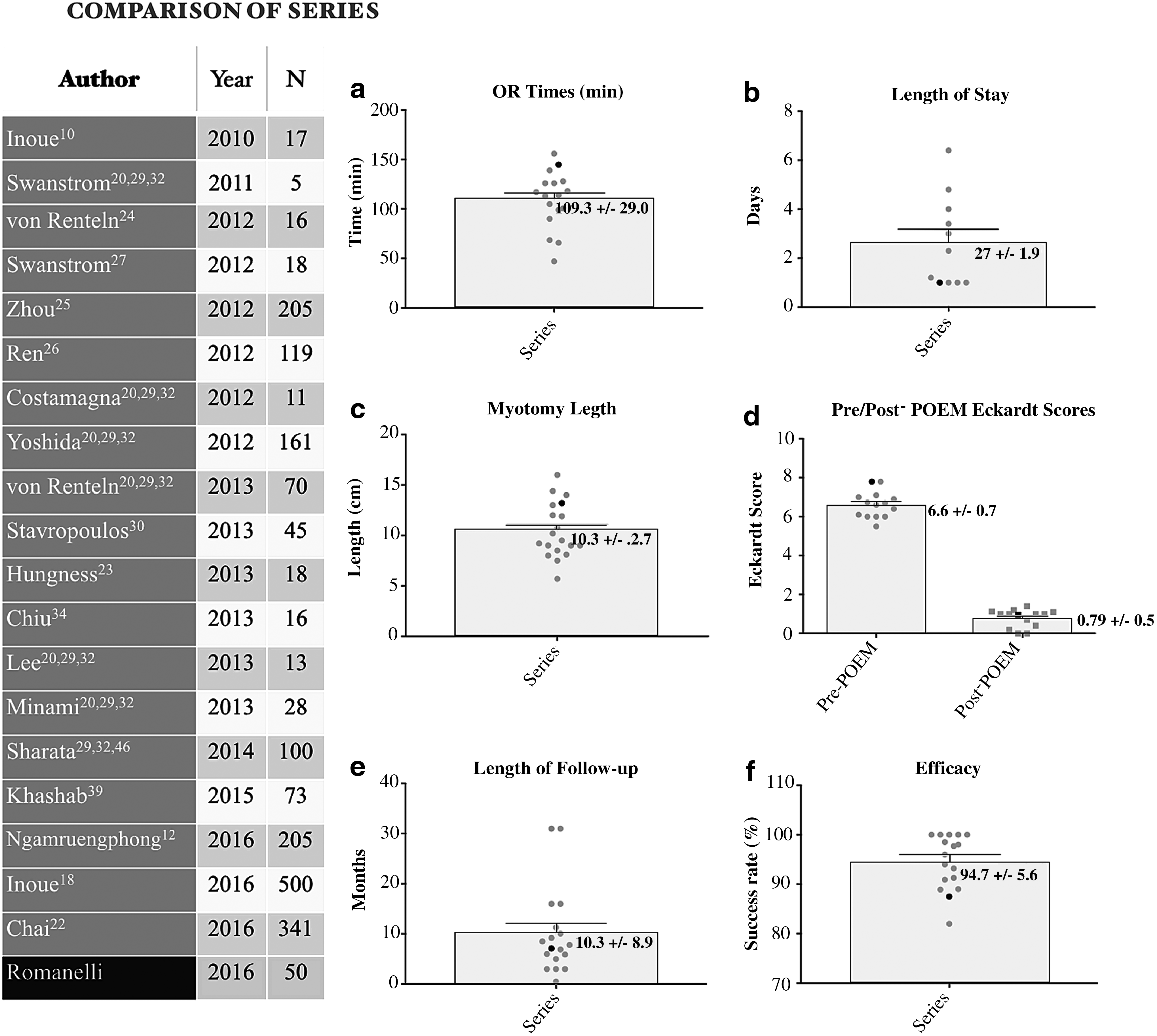
Comparison of outcome means across series. Mean outcomes from previous series were plotted individually on scatter plots (gray), the averages of those outcomes are represented by the boxes with associated standard deviation bars. The individual data point for each outcome from our series is represented in black.
We report an overall complication rate of 4%, with one major and one minor complication. However, if we were to include capnoperitoneum as a complication in our study, our complication rate would increase to 34%. Nevertheless, none of the patients who experienced a peritoneal carbon dioxide leak developed any morbid sequelae. While we are unaware of other cases of capnopericardium, capnomediastinum is a common event, occurring in 10%–22% of POEM cases. 27 Other less common complications published have included submucosal bleeding, submucosal infection, dehiscence of the mucosotomy, pleural effusion, pneumothorax, and mediastinitis. 28
Our average operative time falls in the middle of the mean times reported in previously published series; their operative times range from 47 to 156 minutes (Fig. 5). Our team's learning stage transitioned to a mastery stage after case #15 (mean operative time 136 minutes) with an eventual stabilization at case #39 (mean operative time 121 minutes). Multiple studies have reported that an average of twenty cases are necessary to reach proficiency when the surgeon's learning curve was analyzed.23–30 Patel et al. reported reaching efficiency at 40 and mastery at 60, which is similar to our results thus far; however, this was the experience of a single operator who had completed 100 hours of training ESD in live animal laboratories and had performed 60 human ESD procedures before his first POEM. 31 El Zein et al.32,33 described a learning rate of thirteen cases with a plateau at 102 minutes for a single operator who had performed five nonsurvival and five survival POEM procedures in porcine models before his first human case. Furthermore, both individual operators in these series are gastroenterologists who have had many previous years of experience in therapeutic endoscopy.
Unlike many other previous studies, we report a short median LOS of 1 day, with patients tolerating a soft diet on the first postoperative day. Other case series describe patients staying anywhere from 1 to 6.4 days on average, and not have diets advanced until the second or third postoperative day, 28 potentially reflective of international differences in discharge criteria. The median LOS in the largest case series to date was 4 days. 18
Mean myotomy length across previous studies range from 5.7 cm to 16 cm. On average, our myotomies measured 13.2 cm, which was intentional, as we had a high number of Type II and Type III patients requiring long myotomies. Further study is needed to distinguish optimal myotomy length, as length alone does not necessarily appear to correlate with success rate. In the initial publication of their outcomes in 2011, Swanstrom et al. 27 reported a mean myotomy length of 7.5 cm on five patients with 100% efficacy, while Von Renteln et al. 24 reported only 82% efficacy with mean myotomy length at 13 cm the following year. At a median of 7.7 weeks (average 28.3 weeks), our efficacy is 87.5%, again falling into the average ranges of previous studies (Fig. 5).
Twenty percent of patients in our series reported symptoms of reflux on follow-up, which aligns reports that 8.2%–32% of patients had complaints associated with GERD in series that reported this outcome.17,20,23,24,27,33,34 A large multi-institutional study reported that over 57% of patients had a DeMeester score ≥14.72 at 12 months after POEM. 35 In series where patients underwent postoperative endoscopy, 18%–64.7% had findings of esophagitis, although authors reported that only about half of these were symptomatic.23–30 Furthermore, a recent meta-analysis demonstrated that post-POEM patients were more likely to experience GERD symptoms, erosive esophagitis, and lower pH on manometry than patients who had undergone LHM. 36
In reviewing our results, several learning points became evident. The first is the requisite extent of myotomy onto the gastric cardia. We believe the myotomy performed for patient #3 did not proceed distal enough due to our difficulty identifying the GEJ. Intraoperatively, we measured that the myotomy was made 2 cm onto the stomach by endoscope. This was likely a false measurement due to bowing of the shaft of the scope in the submucosal tunnel. While we debated converting to Heller myotomy in this case, our inexperience, combined with an endoscopic picture of a much more patulous GEJ, led us to falsely conclude that her myotomy was adequate. We do feel that this is a learning curve phenomenon, and we do not believe that we have not had an inadequate myotomy since this case.
Patient #8 was a failed endoscopic myotomy due to poor patient selection. The patient was self-referred from the nearest large metropolitan area, where POEM was at the time unavailable. It was only after the surgery that we completely understood that she underwent botulinum toxin administration 10 days before the operation. We now recognize that this is a contraindication to POEM, as she had an intense scarring reaction at the site of the injection, which would not allow us to distend the submucosa. We also incidentally note that this injection had been above the GE junction, which was likely falsely identified, making the dissection even more difficult. The combination of an endoscopic myotomy to the point of difficulty and an LHM up to that point in a retrograde fashion has led to significant improvement in her symptoms (self-reported “90% improvement” at 2 weeks postoperatively). Based on this experience we feel that patients should wait at least 3–6 months after botulinum toxin administration before POEM.
Another concept that became clear to us was that changing our instrumentation to a hybrid knife led to a drastic reduction in operative times. Our first five cases were performed using a sclerotherapy needle (Olympus America) for raising a saline cushion, and the Olympus TT knife (Olympus America) for mucosal incision, submucosal dissection, and transection of circular muscle fibers. A separate injection catheter (Ball-tip cannula; Cook Endoscopy, Winston-Salem, NC) was used to inject saline mixed with indigo carmine into the submucosa to facilitate the submucosal tunnel. This required continual switching of instrumentation, which delays progress. Our mean operative time in these cases was 225.4 minutes (range 204–267). After the fifth case we changed to the Hybrid Knife (Erbe USA), which allows injection and tissue division without the need for instrument change. Our mean time in the five successful cases following the change in instrumentation was significantly less at 142 minutes (range 128–168; P = .0001).
One weakness in our series is that we did not prospectively measure outcomes utilizing the Eckardt scale 4 until our eleventh case; nevertheless, we were able to calculate the score retrospectively in nine of these based on comprehensive documentation of the patients' descriptions of their symptoms with accurate verbiage aligning directly with the Eckardt scoring system (i.e., “regurgitation after every meal” or “postprandial chest pain daily”). This gives us a data completion rate of 98%. The most recent report of 500 cases by Inoue and Kudo describes only 41.6% of preoperative Eckardt scores obtained, 18 and the meta-analysis by Talukdar et al. reports significant publication bias due to the reporting only of patients on whom both pre- and postoperative Eckardt scores have been obtained. 12 Furthermore, while the Eckardt score is an essential tool to follow the efficacy of POEM objectively, it does not always completely capture the patient's satisfaction. Two patients requiring postprocedure dilation have had some subjective improvement, which was not reflected in their Eckardt score. Performing pre- and postoperative quality of life surveys, like the Gastrointestinal Quality of Life Index or Short Form-36, would aid in depicting the true patient experience in future studies. A further weakness of our series is that despite having started performing POEMs 5 years ago, most patients only return for follow-up up to about 2 months. We did not routinely perform postoperative imaging or endoscopic surveillance unless a patient was experiencing concerning symptoms. As such, we acknowledge that we are not able to report true rates of postoperative esophagitis or to quantify objectively the patency of a patient's GEJ. Lastly, our measurements for OR time do not correspond to a single surgeon's learning curve, but to our surgical endoscopy team, which consisted of two surgeons, two MIS fellows, and two gastroenterologists over the study period. While the metric is imprecise for multiple operators, we feel it reflects the experience at many centers who work in multidisciplinary teams. Understanding OR utilization necessary for this procedure is critical to being able to incorporate POEMs into a clinical practice.
Our two major adverse events bear discussion. In considering the patient who experienced tension capnopericardium we felt that a pinhole perforation likely occurred during the myotomy due to adherence of the pericardium to the esophagus for unclear reasons. 13 There was unexplained lymphadenopathy in the mediastinum on CT scan before the POEM, possibly indicating some type of prior infection or inflammation. This adverse event suggests that it might be safer to divide only the circular muscle fibers during an anterior myotomy. Further, there is a need to prevent the current from penetrating too deeply beyond the muscle layer. We have modified our technique to prevent this error from reoccurring by retracting the muscle into the endoscopic cap whenever possible before applying electrocautery to divide the tissue.
The second adverse event occurred several days after discharge. This patient ate an ethnic food called “fufu,” which is a doughy substance typically not chewed but rather swallowed whole. This caused traumatic hemorrhage in the submucosal tunnel, leading to hospital readmission at an outside institution for acute upper GI bleeding. Fortunately his care providers were in contact with our team, as well as another American POEM expert, and nonoperative management was undertaken. The bleed was self-limited, his symptoms resolved, and he had an Eckardt score of zero at 4-month follow-up. He continues to do well at 3 years of follow-up.
As discussed by Kumta et al., 29 the establishment of a highly skilled multidisciplinary team with trained technical and nursing support is essential for safe performance of POEM. Currently, our team consists of two gastroenterologists, one surgeon, and one MIS fellow. Although the surgeon has advanced endoscopic skills we still believe that the skill level of an advanced therapeutic gastroenterologist provides additional benefit and safety in the performance of POEM. Therefore, we still recommend collaboration between gastroenterologists and surgeons. Similarly, given the potential need to surgically evacuate abdominal gaseous distention or convert to a laparoscopic procedure, we feel that POEM procedures should be performed in the operating room rather than in an endoscopy suite, with surgeons involved. We also believe that the cumulative training, laboratory practice, and clinical experience of each team member also contribute to the safety and successful outcomes of the procedure.
The last 5 years has seen a gradual increase in centers performing POEM in the United States. However, initial adoption of the technique, along with other NOTES procedures, was slow. This may have been due to a determined effort to avoid the rise in complication rates that was seen with early laparoscopic cholecystectomy. 37 It is also possible that this slow adoption was because adequate training in POEM and other NOTES procedures was not widely available. In addition, there is difficulty with reimbursement in this country, and this may also have contributed to the delay in adoption of POEM. Therefore, NOTES procedures have been confined to a few specialized centers with multidisciplinary teams who had obtained appropriate animal and human training. In the case of POEM the lack of widespread availability of instrumentation may have also retarded the popularity of the procedure. Initially, representatives from industry refrained from selling the required instruments to surgeons and gastroenterologists until they had observed the successful performance of the procedure in an animal laboratory. Since this time POEM has gained traction among surgeons and medical device companies alike. Novel techniques and procedural modifications have recently been described, including executing the myotomy along the greater curvature of the stomach, rather than the currently accepted myotomy location along the lesser curvature, for patients requiring reoperation, 38 the use of two endoscopes to confirm the extent of the submucosal tunnel,39–41 concurrent tunneling and myotomy, 42 and ex vivo models for training. 43
Despite these advances there is ample direction for future study and development. 44 At this time training opportunities are still limited, standardization of training has not been instituted, and there is still a need for standardizing the recommendations for credentialing. 45 Furthermore, there is no consensus regarding the risk of postoperative GERD. The rate of patients with reflux will likely become clear as more patients return for follow-up over the long term. Further study is needed to determine whether performing the myotomy on a different part of the esophageal wall would prevent distortion of the angle of His or the sling fibers, perhaps protecting the native antireflux mechanisms. Also, no guidelines have been established for surveillance of esophagitis, nor have guidelines been developed for the surveillance of esophageal carcinoma, even though patients with achalasia have a 50-fold increased risk of developing this cancer. 29
In conclusion, our series shows good results, with few major complications and effective symptom relief, in agreement with the trend of previously published reports. It should be noted, however, that this procedure is not without risk of serious adverse events. For example, we reported a case during which the patient developed capnopericardium and subsequent cardiac arrest. 13 As such, POEM should be performed with caution by operators who have acquired sufficient training and experience of advanced endosurgical techniques. As our community of surgeons and gastroenterologists accumulate experience we will continue to develop more sophisticated techniques to refine POEM with resultant improved outcomes. Questions about gastroesophageal reflux after POEM remain, but these are in the process of being studied. Additional work will involve the standardization of training protocols, further refinement of methods, and development of surveillance guidelines for esophagitis and carcinoma.
Footnotes
Acknowledgments
Special thanks to Drs. David B. Earle, Rebecca Kowalski, Amy Banks-Venegoni, and Mersadies Martin, who helped to take care of these patients during their clinical course.
Author Contributions
Erica Kane: Study design, data collection, data cleaning and statistical analysis, article writing and critical editing.
David Desilets: Patient care, procedure and technique development, article writing and critical editing.
Donna Wilson: Data cleaning and statistical analysis, critical editing.
Marc Leduc: article writing and critical editing.
John Romanelli: Patient care, procedure and technique development, study design, data collection, article writing and critical editing.
Disclosure Statement
Erica Kane, David Desilets, Donna Wilson, and Marc Leduc have no conflicts of interest to report. John Romanelli has consulted for Covidien, although not relevant to this work.