
Abstract
Abstract
Background:
Laparoscopic abdominoperineal resection (LAPR) for rectal cancer (RC) treatment is still controversial, so we conducted this meta-analysis comparing LAPR with conventional open abdominoperineal resection (OAPR) to explore the safety and feasibility of LAPR for RC treatment.
Methods:
A systematic literature search with no limits was performed in PubMed, and Ovid. The last search was performed on June 6, 2017. The outcomes of interests included intraoperative outcomes, pathological outcomes, postoperative outcomes, and survival outcomes.
Results:
Twenty-one articles published between 1997 and 2016 with a total of 20,343 patients were enrolled in this meta-analysis. Compared with OAPR, LAPR showed comparable operative time, less blood loss and intraoperative blood transfusion, smaller length of hospital day and postoperative hospital day, faster recovery of bowel functions, and less postoperative complications, especially less abdominal wound infection. As for pathological outcomes, LAPR was not inferior to OAPR. Besides, LAPR was comparable to OAPR in recurrence rate, 3-year survivals and 5-year survivals.
Conclusions:
LAPR can reduce postoperative complications, lead faster postoperative recovery. In addition, LAPR is not inferior to OAPR in terms of oncological clearance, recurrence rate, and long-time survivals. So LAPR is safe and feasible for RC treatment. Further, more perspective randomized trials can be conducted to compare LAPR and OAPR in the future.
Introduction
R
In 1982, Heald et al. first described total mesorectal excision (TME) for RC surgery. 3 It means the resection of the entire mesorectum and micro-metastasis of lymph nodes.4,5 Then, several studies demonstrated that TME could reduce the incidence of local recurrence and improve prognosis for patients with RC.6,7 Nowadays, TME has been widely accepted as standard surgical procedure in RC treatment.8,9 However, there are several surgical approaches that can perform TME, including inter-sphincter resection, low anterior resection (LAR), and abdominoperineal resection (APR).10–13
APR was first reported by Miles in 1908, so it also called Miles' surgery in which specimen can get from perineal incision directly.14,15 Once in a long time, APR was also widely used for RC. 16 However, in recent years, APR decreased because of the development of sphincter-preserving procedures such as LAR. 15 Although some studies pointed that APR lead more circumferential resection margin (CRM) involvement than LAR, 17 we cannot deny that APR is still the optimal choice for some patients with RC especially these with lower location, perianal muscle invasion, and cannot be radically resected via sphincter-saving techniques.15,16,18,19 Nevertheless, conventional open APR (OAPR) surgery also has disadvantages including long abdominal incision and high risk of infection. Laparoscopic techniques may make up these limitations.
In 1993, laparoscopic surgery (LAS) for colorectal cancer (CRC) was first reported. 20 Since then, LAS has been widely applied for CRC surgery. 21 Many studies have demonstrated that LAS is safe and feasible for colon cancer, but it is still controversial for RC.22–25 Recently, some literatures have reported that laparoscopic is not inferior to open surgery in long time outcomes for TME. But they did not present the data of APR independently.26–28
Several studies have compared laparoscopic APR (LAPR) and OAPR for RC, but the results may differ from each other. 29 In 2013, a meta-analysis reported this issue, but it included only eight articles and the sample size was small. 30 After that, other published studies also investigated LAPR and OAPR. We conducted an updated meta-analysis that included far more articles and patients to compare LAPR and OAPR for RC.
Materials and Methods
Study selection
We performed a literature search in PubMed and Ovid for studies comparing LAPR with OAPR for RC surgery. The key terms included “abdominoperineal resection or abdominoperineal excision or APR” and “colorectal cancer or colorectal carcinoma or rectal cancer or rectal carcinoma” and “laparoscopic or laparoscopic-assisted or laparoscopy.” The final search was performed on June 6, 2017. We also performed a manual search of references of articles and reviews for additional potentially eligible studies.
Inclusion and exclusion criteria
The inclusion criteria for this meta-analysis were as follows: (1) case–control study (LAPR versus OAPR); (2) RC; (3) studies with total sample size more than 20; (4) intraoperative and/or postoperative outcomes and/or survival outcomes were reported. The exclusion criteria studies were as follows: (1) review articles; (2) correspondences or editorial; (3) conference abstract without detail data; (4) studies including benign diseases; (5) animal studies; (6) single-arm studies.
Data extraction
Two authors (X.Z. and Q.W.) reviewed all the identified articles independently. They solved the discrepancies by discussion; if needed, a third reviewer (Z.W.) was necessary. We extracted the following items from each study: first author's name, year of publication, country, publication type, study type, bowel preparation, location of disease, number of total patients and male in gender in each study, age, body mass index (BMI), previous abdominal surgery (PAS), tumor stage, and outcomes of interests.
Outcomes of interests
Intraoperative outcomes
Operative time, blood loss, intraoperative blood transfusion.
Pathological outcomes
Lymph node harvested, length of specimen, positive CRM.
Postoperative outcomes
Hospital day, postoperative hospital day, time to first flatus, time to first bowel movement, time to first fluid diet, time to first soft diet, time to first normal diet, reoperation, ileus, pelvic abscess, postoperative blood transfusion, bleeding, hernia, deep venous thrombosis, perineal wound infection, abdominal wound infection, wound dehiscence, other wound complication, pulmonary infection, urinary retention, urinary tract infection, urinary injury, postoperative complication, morbidity, mortality, and readmission.
Survival outcomes
Local recurrence, wound recurrence, 3-year overall survival (OS), 3-year disease-free survival (DFS), 5-year OS, and 5-year DFS.
Quality assessment
The methodological quality of the enrolled retrospective studies was assessed using the revised and modified grading system of the Scottish Intercollegiate Guidelines Network. 31 Articles achieving less than 8 scores, 8–14 scores, and more than 14 scores (total score, 20) were defined as poor quality, fair quality, and good quality, respectively. And the methodological quality of the randomized controlled trials was assessed by modified Jadad score system (total score, 5; 1–2, low quality; 3–5, high quality). 32
Statistical analysis
All data analyses were conducted using the Review Manager version 5.0 (The Cochrane Collaboration, Software Update, Oxford) and P < .05 was considered statistically significant. Weighted mean difference (WMD) or standard mean difference (SMD) was calculated for the continuous outcomes, and pooled odds ratios (ORs) or risk ratios (RR) were calculated for the dichotomous outcomes. For continuous outcomes, if the study only provided means and range values or median and range values, the means and standard deviations were calculated using methods described by Hozo et al. 33 Chi-squared test and Higgins I2-test were used for heterogeneity test. A value of P < .05 and I2 > 50% was regarded as existing heterogeneity. If I2 > 50% and P < .05, a random-effects model was applied. Correspondingly, if I2 < 50% and P > .05, a fixed-effects model was applied. Begg's funnel plot was used to evaluate publication bias. The survival curves in articles were obtained by Engauge Digitizer version 4.1.
Results
The process and result of literature searching were shown in Figure 1. The initial search algorithm retrieved a total of 1956 studies. After removing duplications, there still remained 1404 studies. After reviewing titles and abstracts, only 51 relevant studies were kept for further evaluation. Besides, no additional record was identified through manual search. Among the 51 studies, 30 literatures were excluded due to following reasons: 1 study was review article, 1 was correspondence, 1 was editorial, 8 studies did not present independent data for APR, 14 studies were conference abstract without detail data, 3 were single-arm studies, and 2 with a small sample size. Finally, 21 articles15,17,19,34–51 published between 1997 and 2016 were included in our meta-analysis. Three studies were randomized controlled trial.34,39,41 The characteristics of the included studies were summarized in Table 1. A total of 20,343 patients (5548 by LAPR and 14,795 by OAPR) were enrolled.
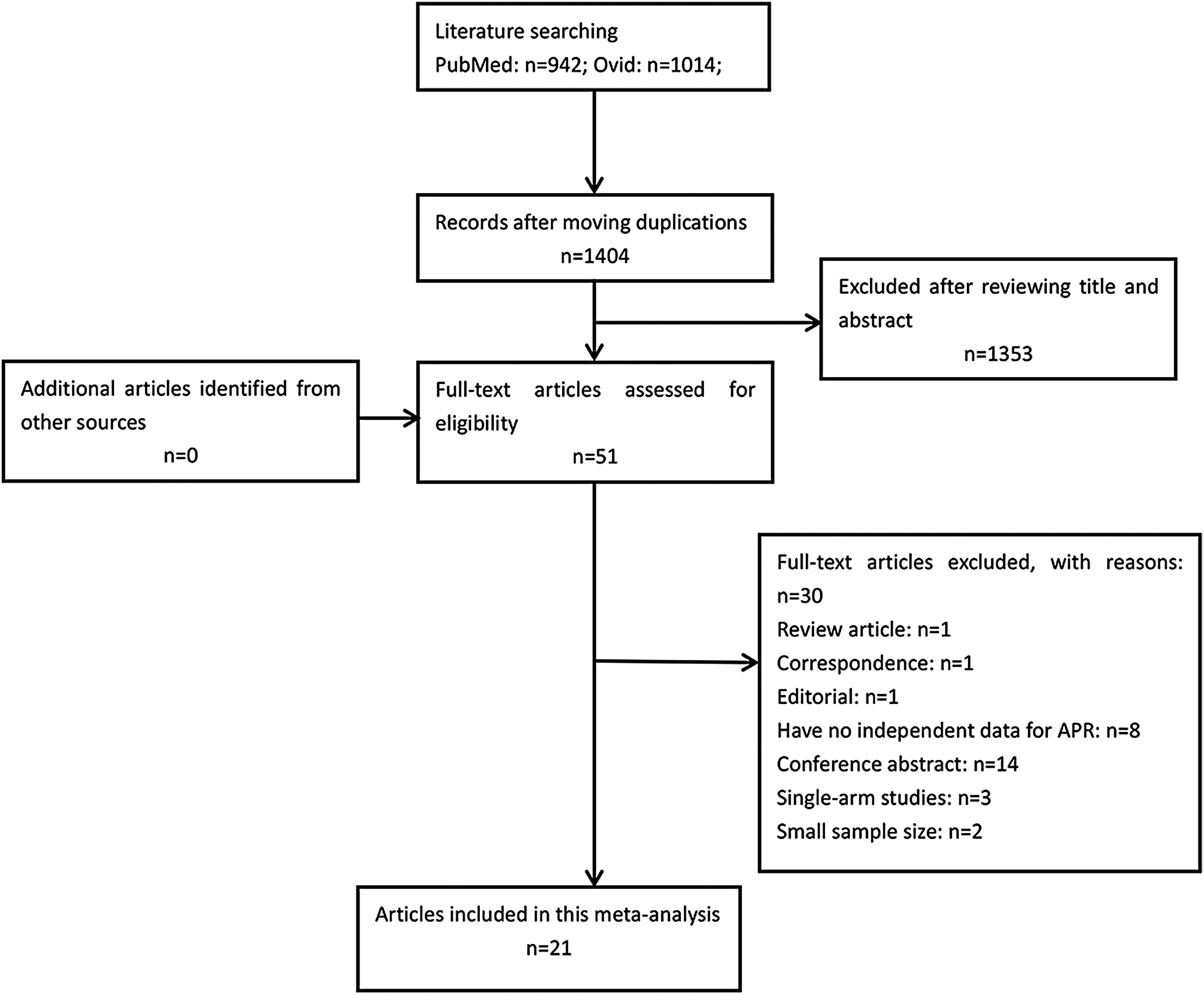
PRISMA diagram. APR, abdominoperineal resection.
Distance to dentate line.
BMI, body mass index; LAPR, laparoscopic abdominoperineal resection; NR, not reported; OAPR, open abdominoperineal resection; PAS, previous abdominal surgery; PNCT, prospective nonrandomized controlled trials; PRCT, prospective randomized controlled trials; RCCS, retrospective case–control study.
Patient demographics
There was no significant difference between the two groups in terms of age (P = .14, WMD = 1.36, 95% CI [−0.43, 3.15], I2 = 64%), male gender (P = .42, OR = 0.97, 95% CI [0.91, 1.04], I2 = 19%), BMI (P = .35, WMD = 0.52, 95% CI [−0.57, 1.61], I2 = 65%), tumor stage (P = .57, OR = 0.92, 95% CI [0.71, 1.21], I2 = 17%), distance to anal verge (P = .09, WMD = −0.33, 95% CI [−0.72, 0.05], I2 = 78%), or PAS (P = .21, OR = 0.72, 95% CI [0.43, 1.21], I2 = 0%).
Quality of included studies
The scores of methodological quality assessment of the enrolled retrospective studies and randomized controlled trial were shown in Tables 2 and 3. Among the 21 articles, 15 retrospective studies15,35–38,40,42–49,51 were with fair quality (8–14 scores), other 2 retrospective studies17,19 had high quality (16 scores). Three prospective randomized studies34,39,41 were with low quality (1–2 scores). Besides, one study 50 was prospective but nonrandomized so we did not assess the quality.
Total scores: 20; <8, poor quality; 8–14, fair quality; >14, good quality.
LAPR, laparoscopic abdominoperineal resection.
1, reported; 0, not reported. A total modified Jadad score of 1–2, low quality trial; 3–5, high quality trial.
Meta-analysis of intraoperative outcomes
The results demonstrated that there was no significant difference between the two groups in operative time (P = .07, WMD = 18.40, 95% CI [−1.16, 37.97], I2 = 93%). However, the LAPR group had a significantly less blood loss (P < .001, WMD = −136.22, 95% CI [−195.00, −77.45], I2 = 92%) though there existed a high heterogeneity. Besides, we also observed a less intraoperative blood transfusion in the LAPR group (P = .002, OR = 0.39, 95% CI [0.08, 0.55], I2 = 0%) (Fig. 2).
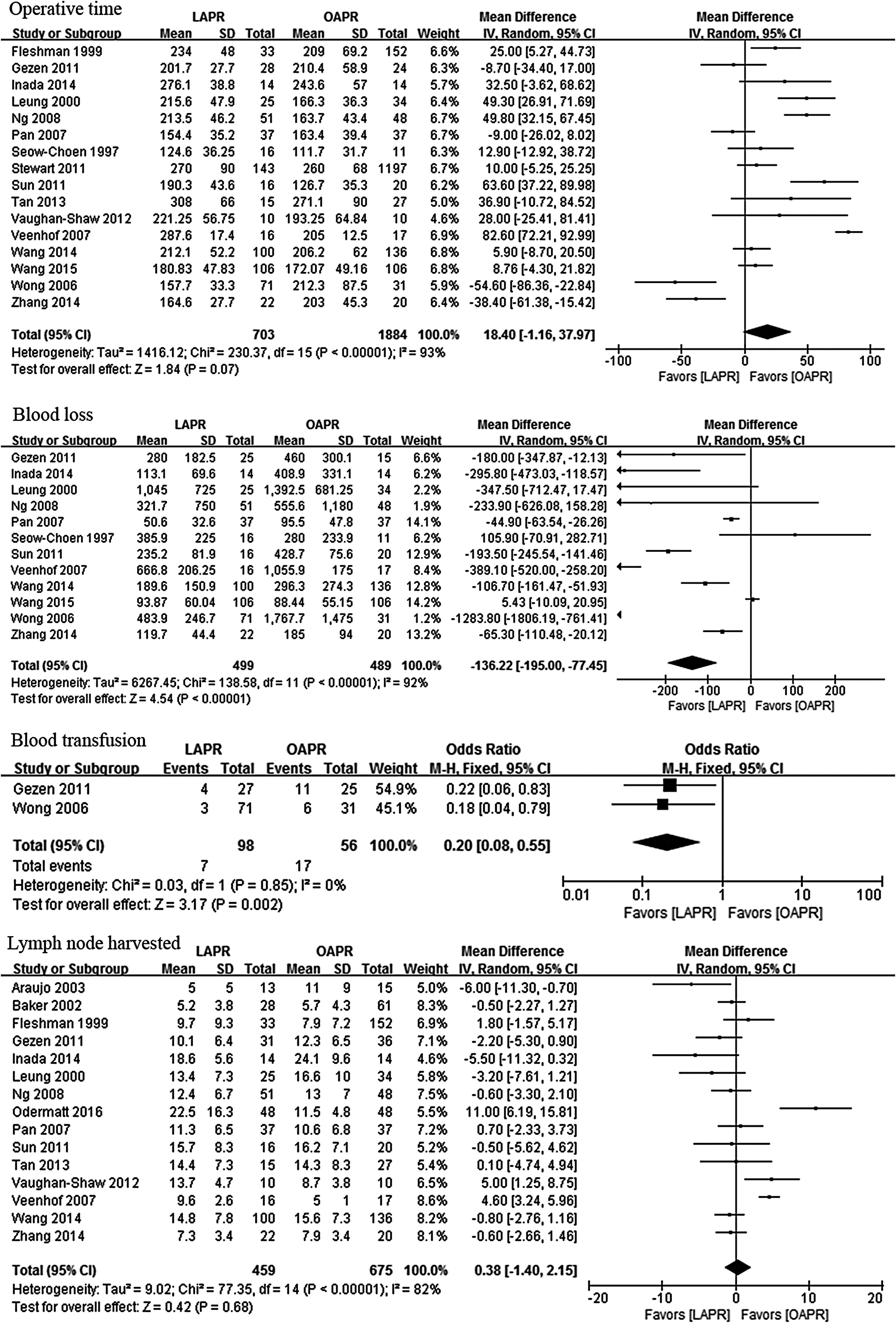
Meta-analysis of intraoperative outcomes, pathological outcomes and recurrence rate. CRM, circumferential resection margin; LAPR, laparoscopic abdominoperineal resection; OAPR, open abdominoperineal resection.
Meta-analysis of pathological outcomes
No significant difference was observed in terms of lymph node harvested (P = .68, WMD = 0.38, 95% CI [−1.40, 2.15], I2 = 82%), length of specimen (P = .48, WMD = −0.27, 95% CI [−1.02, 0.48], I2 = 0%), or positive CRM (P = .35, OR = 0.69, 95% CI [0.32, 1.50], I2 = 0%) (Fig. 2).
Meta-analysis of postoperative outcomes
When compared with the OAPR group, the LAPR group showed a significantly smaller length of hospital day (P < .001, WMD = −3.13, 95% CI [−4.55, −1.71], I2 = 87%) and postoperative hospital day (P < .001, WMD = −2.54, 95% CI [−3.29, −1.79], I2 = 63%). As for recovery of bowel function, the LAPR group had a significantly less time to first flatus (P = .003, SMD = −0.75, 95% CI [−1.26, −0.25], I2 = 89%), time to first bowel movement (P = .01, WMD = −0.90, 95% CI [−1.62, −0.18], I2 = 70%), time to first fluid diet (P = .004, WMD = −2.53, 95% CI [−4.25, −0.81], I2 = 93%), time to first soft diet (P < .001, WMD = −3.26, 95% CI [−4.23, −2.29], I2 = 0%), and time to first normal diet (P < .001, WMD = −1.18, 95% CI [−1.46, −0.90], I2 = 0%) (Fig. 3).
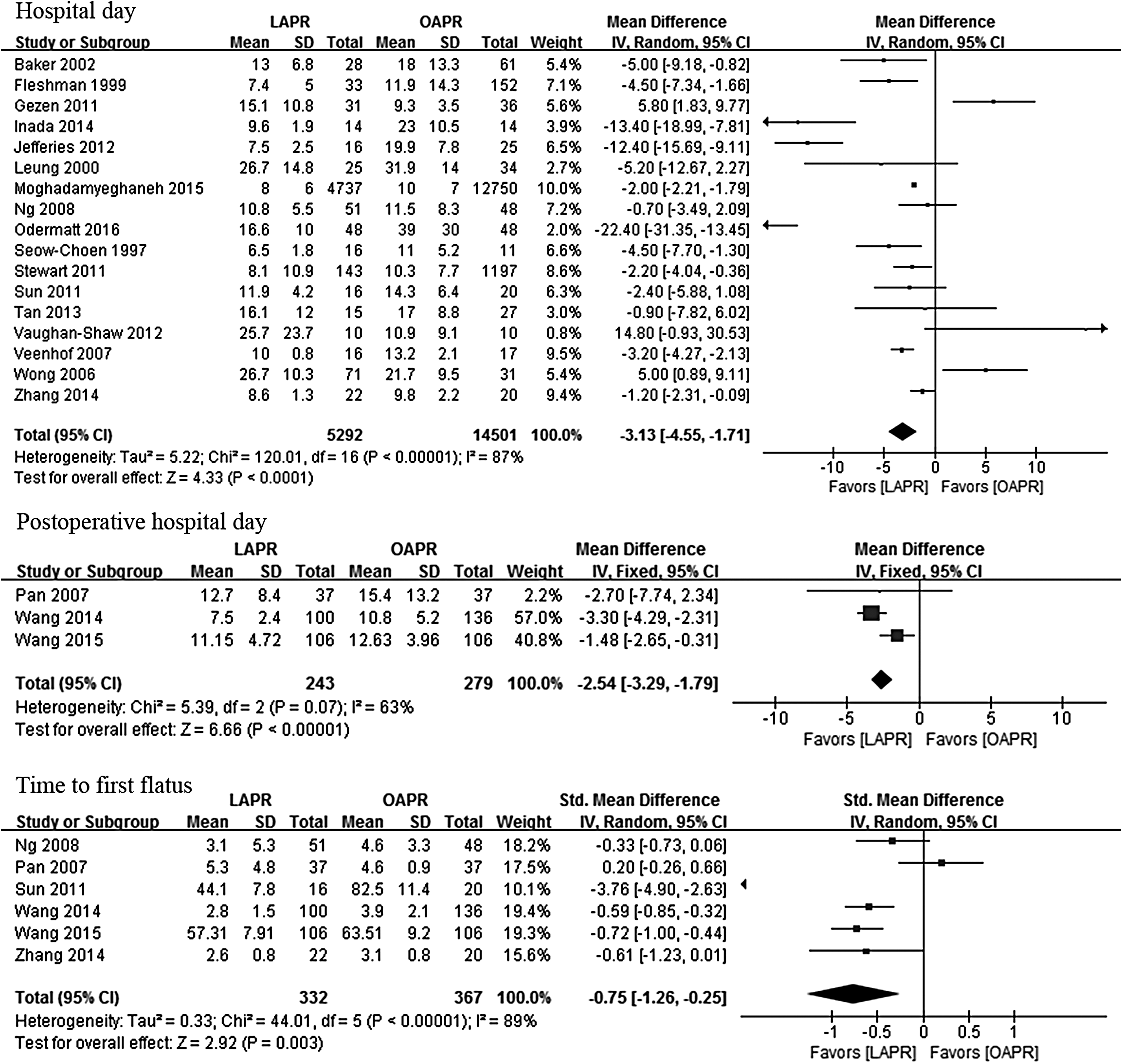
Meta-analysis of postoperative outcomes. LAPR, laparoscopic abdominoperineal resection; OAPR, open abdominoperineal resection.
When it came to postoperative complications, we observed that LAPR could reduce ileus (P = .01, OR = 0.90, 95% CI [0.83, 0.98], I2 = 0%), deep venous thrombosis (P = .01, OR = 0.16, 95% CI [0.04, 0.66], I2 = 0%), and total postoperative complications (P = .009, OR = 0.69, 95% CI [0.52, 0.91], I2 = 0%). Besides, LAPR is comparable to OAPR in reoperation (P = .15, OR = 0.46, 95% CI [0.16, 1.31], I2 = 0%), postoperative blood transfusion (P = .06, OR = 0.36, 95% CI [0.13, 1.03], I2 = 0%), bleeding (P = .42, OR = 0.92, 95% CI [0.75, 1.13], I2 = 0%), hernia (P = .27, OR = 2.17, 95% CI [0.55, 8.56], I2 = 0%), morbidity (P = .12, OR = 0.42, 95% CI [0.14, 1.27], I2 = 84%), mortality (P = .05, RR = 0.67, 95% CI [0.45, 1.00], I2 = 0%), and readmission (P = .19, OR = 0.62, 95% CI [0.30, 1.26], I2 = 0%) (Table 4).
Bold values signify when P value <.05.
RR.
LAPR, laparoscopic abdominoperineal resection; OAPR, open abdominoperineal resection; OR, odds ratio; RR, risk ratio; CI, confidence interval.
In addition, we also compared some other complications associated with infections. The results revealed that the LAPR group had significantly less abdominal wound infection (P = .01, OR = 0.27, [0.10, 0.75], I2 = 0%), and urinary tract infection (P = .01, OR = 0.83, [0.72, 0.96], I2 = 0%). Nevertheless, no significant difference was observed in pelvic abscess (P = .68, OR = 1.33, 95% CI [0.35, 5.04], I2 = 0%), perineal wound infection (P = .29, OR = 1.29, 95% CI [0.81, 2.06], I2 = 50%), or pulmonary infection (P = .05, OR = 0.45, 95% CI [0.20, 1.01], I2 = 0%). Particularly, there was no significant difference between the two groups in wound dehiscence (P = .58, OR = 1.25, 95% CI [0.57, 2.73], I2 = 0%), other wound complication (P = .66, OR = 0.60, 95% CI [0.07, 5.60], I2 = 68%), urinary retention (P = .37, OR = 0.81, 95% CI [0.52, 1.28], I2 = 0%), or urinary injury (P = .44, OR = 1.65, 95% CI [0.47, 5.76], I2 = 0%) (Table 4).
Meta-analysis of survival outcomes
We found that LAPR was not inferior to OAPR in terms of local recurrence (P = .45, OR = 0.81, 95% CI [0.47, 1.39], I2 = 0%), wound recurrence (P = .70, OR = 0.70, 95% CI [0.11, 4.39], I2 = 0%) (Fig. 2), 3-year OS (P = .87, HR = 1.03, 95% CI [0.71, 1.50], I2 = 0%), 3-year DFS (P = .94, HR = 0.98, 95% CI [0.54, 1.77], I2 = 0%), 5-year OS (P = .82, HR = 0.95, 95% CI [0.58, 1.54], I2 = 0%), or 5-year DFS (P = .80, HR = 0.87, 95% CI [0.30, 2.49], I2 = 0%) (Table 5).
CI, confidence interval; DFS, disease-free survival; HR, hazard ratio; LAPR, laparoscopic abdominoperineal resection; OAPR, open abdominoperineal resection; OS, overall survival.
Publication bias
A funnel plot of the studies reporting on urinary retention shows that there was no obvious publication bias among the studies (Fig. 4).
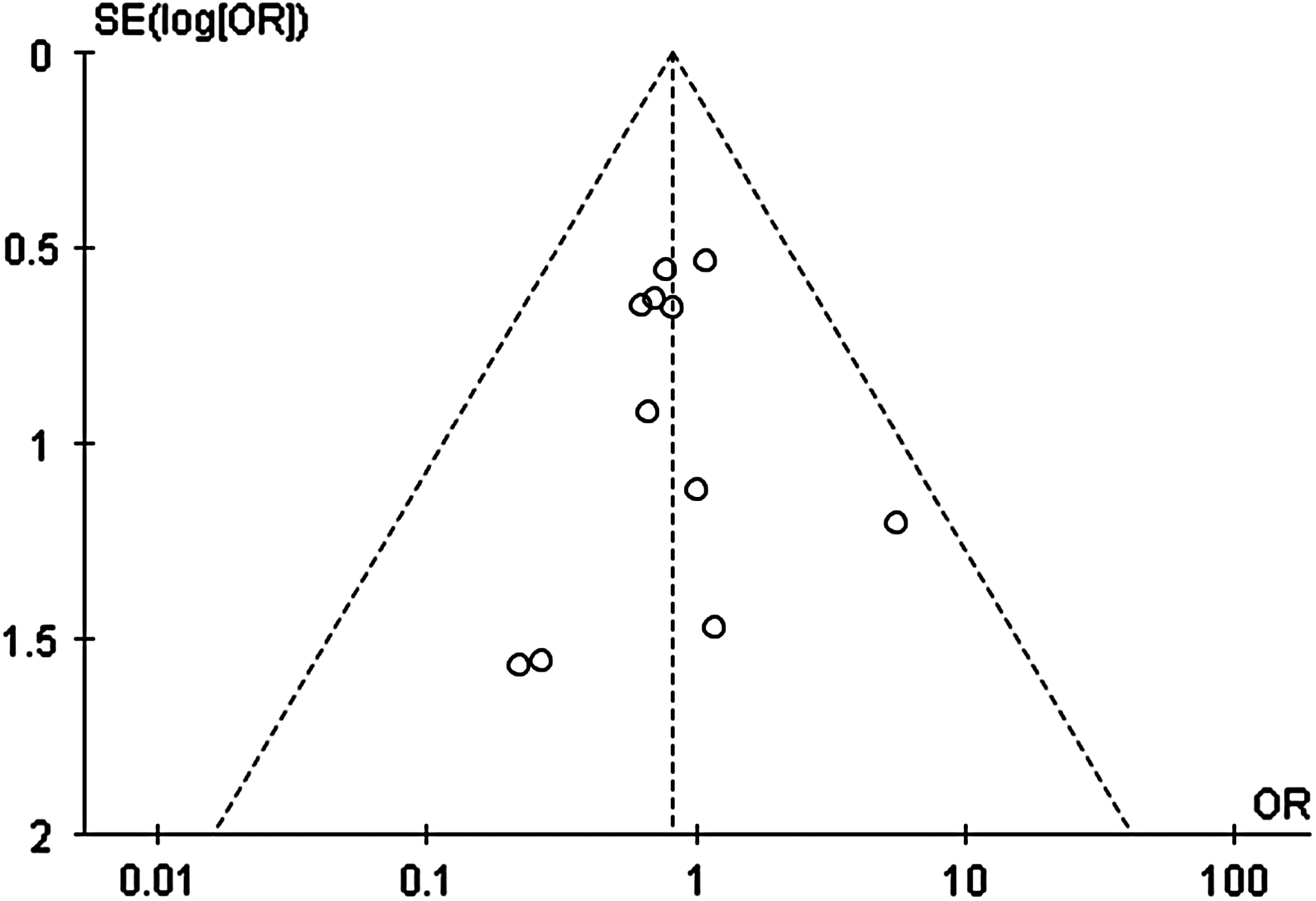
Funnel plots of the studies reporting on urinary retention.
Discussion
More than 100 years ago, Miles first reported APR as surgical treatment for RC. 52 In the past decades, the developments of TME and other surgical equipment have made APR more efficient in RC treatment though laparoscopic technique is still debatable.19,35 In recent years, many studies compared LAPR with OAPR for RC and the outcomes were conflicting. Up to this day, APR had walked a long way with controversy and challenges. So we performed this meta-analysis including 21 articles and 20,343 patients to compare LAPR with OAPR for RC treatment.
Interestingly, in line with previous meta-analysis, 30 the operative time was similar in the two groups. Several studies pointed that was because of the increasing experience in performing laparoscopic techniques.30,50 We also think it is the main reason. Besides, LAPR does not need the same laparotomy as OAPR and has advantages in dissecting adhesion. 36 The similar perineal phase in the two groups may also contribute to that result. 34 Besides, we think BMI and PAS can also have influence on operative time. 53 However, we did not find difference in BMI and PAS between the two groups. So with the balance of several factors, LAPR and OAPR were comparable on operative time.
Against previous meta-analysis, 30 we observed less hospital stay and faster recovery of bowel functions in the LAPR group. These results were supported by another study. 27 The possible reason is that the LAPR group had significantly less intraoperative and postoperative complications. In addition, LAPR may help reduce the bowel mobilization that can accelerate the recovery of bowel functions. This reason can also account for the less ileus in the LAPR group. Although electrocoagulation equipment was widely used in surgery, the LAPR group still had less blood loss and intraoperative blood transfusion than the OAPR group. We explain it that LAPR has a better magnified visualization, 34 so it can reduce the injury to blood vessels. 47 No significant difference was observed in perineal wound infection. The similar procedure of perineal phase may account for it. 34 However, as expectation, LAPR had less abdominal wound infection. We think it is because LAPR had a smaller length of abdominal incision that can decrease the risk of infection. Additionally, there existed no significant difference in terms of other wound complications such as dehiscence or hernia. We think it may be related with the nursing level of hospitals. Particularly, patients in APR group had less deep venous thrombosis formation. This may be because LAPR can lead smaller abdominal incision and less postoperative pain so patients can do off-bed activity earlier.
When performing surgery in deep pelvic cavity, it is easy to hurt urogenital system. Urethral disfunction is a common complication after rectal surgery.54–56 Our results revealed that LAPR was not superior to OAPR in this aspect though it has a better view. The possible reason is that pelvic cavity is narrow and pelvic organs have a too adjacent location. These will add difficulty for both LAPR and OAPR. Although LAPR showed a less urinary tract infection, we think this may associate with the care of catheter. Besides, no significant difference was observed in pelvic abscess. This may be because of the use of antibiotics and abdominal drainage.
As for oncological clearance, LAPR was not inferior to OAPR in lymph node harvested, length of specimen, and positive CRM, which was reported as important parameter for local recurrence. This result is consistent with previous meta-analysis and review.29,30 The possible reason is that both LAPR and OAPR need comply with the same surgical principles for tumor strictly such as TME. Although one previous meta-analysis 57 showed LAS had higher risk of noncomplete mesorectal excision, we did not have efficient data to prove it. In our opinion, all the surgeons want to clear tumor tissue as far as possible to avoid local recurrence. Before surgery, both surgeons and patients will make full preparation including computed tomography scan, magnetic resonance imaging, endoscopy, and preoperative tumor stage. Besides, we think the learning curve of pathologists 34 and preoperative chemoradiotherapy can have an important influence on these pathological outcomes.
For both surgeons and patients, the most concern for LAPR may be the long-time outcomes. Different from previous meta-analysis, 30 recurrence rate was similar in the two groups. This result was supported by previous review. 29 Nevertheless, consistent with pervious meta-analysis,26,30 LAPR was comparable to OAPR in survival outcomes in our study, including 3-year OS, DFS, and 5-year OS, DFS. This may be due to the similar oncological clearance in the two groups. However, we cannot deny that preoperative and neoadjuvant chemoradiotherapy can help improve the survivals.
Some limitations of this study have to be highlighted. Frist, there existed high heterogeneity in some analyses. Though the sensitivity analysis was conducted by removing one study each time, the outcomes remained unchanged. We thought it might be influenced by many factors, such as the learning curve of surgeon, bowel preparation, tumor stage, distances to anal verge, PAS, and preoperative chemoradiotherapy. Second, most of the enrolled articles were retrospective studies and this might induce patient selection bias though there were three randomized controlled trials that were in low quality. Third, when the survival outcomes were calculated by the survival curves some systematic errors might exist.
In conclusion, based on the results of our meta-analysis, we think LAPR can reduce postoperative complications and lead to faster postoperative recovery. In addition, LAPR is not inferior to OAPR in terms of oncological clearance, recurrence rate, and long-time survivals. So LAPR is safe and feasible for RC treatment. Further, more perspective randomized trials can be conducted to compare LAPR and OAPR in the future.
Footnotes
Acknowledgments
This work was supported by the Science and Technology Support Program of the Science & Technology Department of Sichuan Province (Grant No. 2016SZ0043).
Disclosure Statement
No competing financial interests exist.