
Abstract
Abstract
Introduction:
Different methods and devices have been developed to regulate cerebrospinal fluid flow for the treatment of congenital hydrocephalus (HC). In addition, progress in shape and materials of catheters and also valves has been achieved. Although many studies in literature have evaluated the benefits of a laparoscopic approach, few researches have compared the two techniques used for the insertion of the ventriculoperitoneal shunt (VPS).
Aim:
The aim of this study was to compare laparoscopically assisted VPS (LVPS) with open VPS and to evaluate the benefits of LVPS.
Patients and Methods:
This cross-sectional analytic study was conducted on 192 children undergoing either laparoscopic or open placement of VPSs for congenital HC over 1-year period. Insertion of the proximal tube and reservoir were performed and the distal tube was then passed into the peritoneal cavity, either conventionally or laparoscopically assisted.
Results:
Mean operative time was 50.1 minutes (28.0–121.8 minutes) in the laparoscopic group versus 74.0 minutes (39.0–162.0 minutes) in the open group (P < .05). Duration of hospital stay was the same (P = .938). The percentage of shunt failure during the follow-up period was 10% in the laparoscopic group and 17% in the open group (P = .623). Shunts were working in 85% at 6 months and 78.5% at 1 year.
Conclusion:
The laparoscopically assisted placement of VPS in children is safe, effective, associated with lower rates of abdominal malposition of the distal catheter, and a technically easy approach. It is an alternative method that may improve and simplify the safety of VPS surgery.
Introduction
C
Despite its frequent use in the treatment of HC, complications are common and most of them unavoidable. The definition of clinical shunt failure is that the patient needs surgery for treatment of a shunt-related problem. Complications were categorized as proximal to the reservoir, at the level of the reservoir, and distally. Causes include proximal catheter malposition, distal catheter malposition, obstruction or infection of the shunt, valve malfunction, and overdrainage. 2
Shunt infection was defined as an increase in white blood cell count proved by a positive cerebrospinal fluid (CSF) culture from the shunt tap in a symptomatic patient associated with a positive wound culture taken during the shunt revision surgery. 2
Shunt dysfunction caused by malpositioning and mechanical failure is common after 1 year; the failure rates can be as high as 40%. 3 The distal tube failure rate represents 30% of all failures that need revisions. 4
The innovation of laparoscopic procedures in neurosurgery was first described for the removal of a disconnected distal shunt in children.5,6
Eventually, Armbruster et al., Basauri et al. and Schievink et al. evolved the use of laparoscopically assisted procedures allowing the insertion of the distal catheter under vision as an alternative to the conventional laparotomy techniques.7–9
The laparoscopic technique provides a lot of advantages including visualization of the abdominal cavity, visual confirmation of catheter position, and function of shunt (by observing the CSF outflow from the distal catheter end), and the advantage to perform adhesiolysis in patients with a history of abdominal surgery. In addition, it is supposed that it can reduce the operative time, reduce the incidence of postoperative adhesions, and its smaller incision may reduce the incidence of complications like postoperative herniation and infection. Also, it improves the postoperative convalescence by reducing the postoperative pain, the need for medications used, and allows for early mobilization resulting in a shorter length of hospital stay that decreases the risk of chest infection especially in children.10–13
Almost all neurosurgeons are experts in conventional VPS operation, but laparoscopically assisted procedure is a new technique to them. Laparoscopically assisted surgery is considered as an alternative procedure that may improve and simplify the safety of VPS surgery. 14 Although there are many researches reporting the benefits of a minimally invasive approach, few have directly compared the two techniques used in VPS surgery. 14
Patients and Methods
This cross-sectional analytic study included 192 children undergoing either laparoscopic or open placement of VPSs for congenital HC at Assiut University Hospital over 1-year period, between September 2015 and September 2016.
Inclusion criteria
The inclusion criterion was children requiring new VPS for treatment of congenital HC. The selection for either the laparoscopy or laparotomy group was random.
Exclusion criteria
The exclusion criteria were all shunt revisions and patients who underwent previous shunt extraction, history of previous abdominal surgery, or parent refusal to participate in the study.
Operative technique
After induction of general anesthesia, the patient was placed in the supine position, with the patient's head turned to the other side of the shunt. A semicircular scalp flap was raised, and then a burr hole created in the skull. The ventricle was accessed, and the shunt tubing inserted. The catheter was connected by a one-way reservoir to the distal catheter that was inserted into the peritoneal cavity.
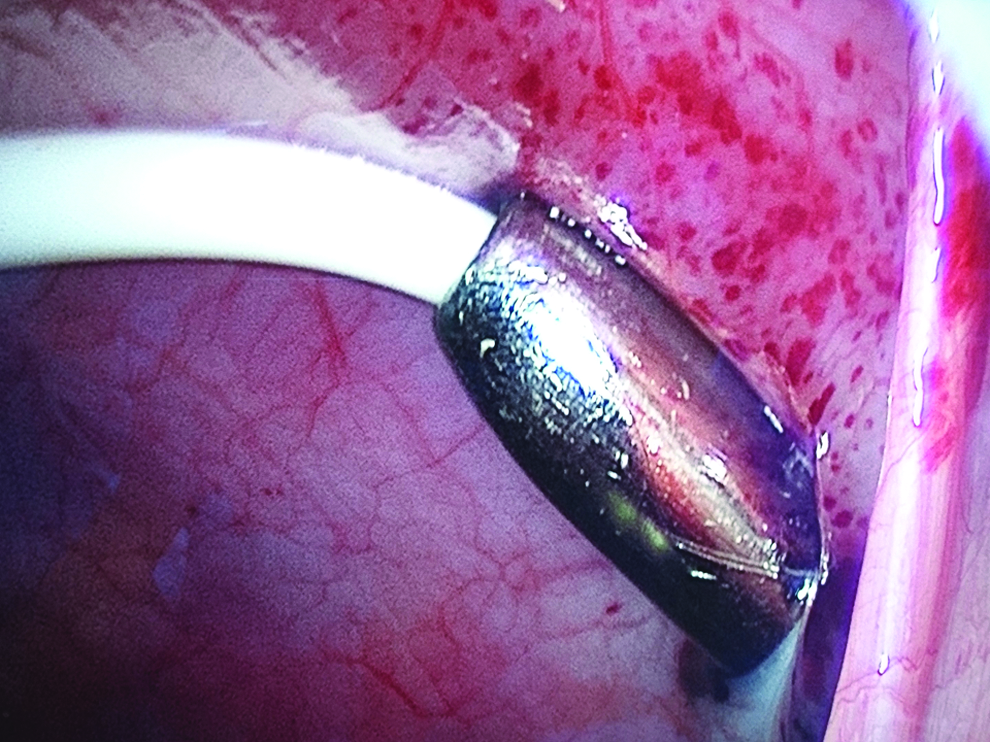
Insertion of the distal catheter was done either through the standard technique, from a small incision on the abdominal wall 1 inch above and lateral to the umbilicus (Group A), or laparoscopically (Group B); pneumoperitoneum was established to a pressure of 10 to 12 mm Hg using a Veress needle. After insufflation, a 5-mm optical trocar was placed through a subumbilical incision, and another 5 mm trocar was placed ∼10 cm away from the tunnel site (Fig. 1). A 10-French introducer sheath (Hickman peel away) was used for placement of the distal catheter in the peritoneal cavity (Figs. 2 and 3).

A 5-mm optical trocar and another 5-mm working trocar.

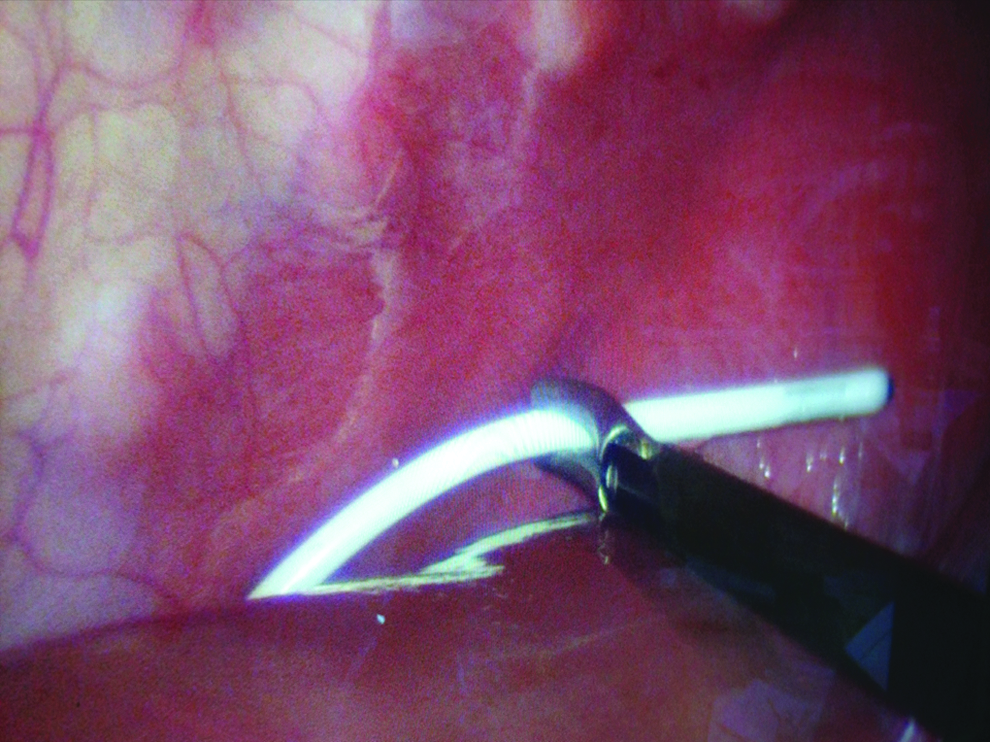
10-French introducer sheath (Hickman peel away).
10-French introducer sheath (Hickman peel away) with the distal catheter appears through it.
The flow of CSF through the catheter was then visually confirmed while pressing on the proximal valve (Fig. 4). The tip of the catheter was placed in the right subdiaphragmatic space to minimize the risk of omental adhesions (Fig. 5). The abdomen was then desufflated, and the trocar site and the tunnel site were closed with absorbable subcuticular sutures.

Cerebrospinal fluid flow was visually confirmed.
The tip of the distal catheter placed in the right subdiaphragmatic space.
The decision for laparoscopy or laparotomy was randomly selected.
Demographic, clinical, and operative data of all patients were collected by reviewing all medical records of each patient and included (1) chart review, (2) examination of operative notes, and (3) brain computed tomography (CT) scan examination.
Independent variables analyzed in this study included the following: demographic data (e.g., gender and age) and indications for VPS. We carefully saved the preoperative imaging (CT) data, the details of the operative technique (whether open or laparoscopic and intraoperative findings), the specifications of the used catheter, and also all clinical notes and reports of radiographic studies during the follow-up period for 1 year.
Dependent variables investigated included the following: operative time, length of hospital stay, findings on postoperative head CT scan (immediately postoperatively and 4–8 weeks after surgery, and monthly thereafter to assess early and delayed postoperative complications), the appearance of any shunt failure and its cause, and any other complications.
Shunt obstruction was evaluated. The intraventricular catheter was disconnected from the reservoir and checked for flow. The distal catheter was checked by a Marx needle and injected with saline. The ventricular and abdominal catheters malposition were radiographically evaluated and then confirmed during surgery. Overdrainage was diagnosed either by the presence of radiographically slit ventricles or the development of a recent and significant subdural fluid collected requiring surgical revision.
In this study, patients were routinely followed for a minimum of 1 year after the operation and then informed to return only for any signs of malfunctioning. We considered patients who did not return to this or any other hospital owing to problems related to the shunt had a functioning hardware for the entire period.
Ethical consideration
The study was approved by the Medical Ethical Committee of Assiut Faculty of Medicine. Parents of the children gave their written consent to participate in the study, to ensure the randomization.
Statistical analysis
SPSS software for Windows, version 23 (SPSS, Inc., Chicago, IL) was used for data analysis. Data were presented as mean or number and percentage. Statistical analysis for categorical variable was performed using chi-square tests. Continues variables were compared using t-test. A P value of <.05 was considered significant.
Results
Between September 2015 and September 2016, a total of 192 children with HC underwent new placement of a VPS. The mean age was 2.4 years (age range: 0.6 − 5 years) in Group A, and 2.5 years (age range: 0.9–5.3 years) in Group B. There were 59 boys and 41 girls in Group A and 56 boys and 36 girls in Group B. In 100 (50%) cases, the distal shunt was placed by open technique (Group A) and in another 92 (47.9%) cases, the placement of the distal catheter was performed laparoscopically (Group B).
None of the laparoscopic cases required conversion to open. Both groups were similar in term of gender, age, and indication for VPS surgery.
Operative time was considered as the time from skin incision to skin closure. The mean operative time in all cases was 60.0 minutes (range: 28.0–162.0 minutes), in the laparoscopic group the mean operative time was significantly shorter, 50.1 minutes (28.0–121.8 minutes) compared with the time spent in open cases, 74.0 minutes (39.0–162.0 minutes) (P < .05) (Table 1).
The overall number of postoperative complications was 27/192 (14.1%), and there was no significant difference between the open and the laparoscopic groups.
Causes of shunt failure had been categorized as proximal (infection, malposition, and obstruction), distal (infection, malposition, and obstruction), reservoir revision, and overdrainage. The overall number of shunt failures in this study was 27 (14.1%), and of those 14 (51.8%) shunts failed in the first 3 months of the follow-up period. The most common cause of shunt failure was an infection (proximal or distal), followed by proximal and distal tube malfunction, and finally reservoir malfunction. There was a no statistically significant difference between the open and the laparoscopic groups in terms of shunt failure rate (n = 17/or 17% versus n = 10/or 10.9%, P = .6).
In Group A, 9 patients developed an infection of the abdominal incision after surgery without signs of distal shunt obstruction or malposition, 4 of them improved before discharge and the other 5 required shunt extractions. Four patients had malposition of the distal catheter requiring revision. Three patients had a proximal catheter failure, and 1 patient had a valve failure and all required revisions.
In Group B, an infection of the proximal catheter occurred in 5 patients: in 2 patients, the shunt was removed because of the persistence of fever and proved by positive CSF cultures, the other 2 patients were treated successfully with vancomycin. One patient developed mild erythema of the abdominal incision and was treated successfully. Three patients required proximal catheter revision because of malposition, and 2 other patients had reservoir failure requiring revision. There was no further complication in these patients after their discharge. Significantly, there were no postoperative distal complications in the laparoscopic group of patients (Table 2).
The mean length of hospital stay in all shunt patients was 2 days (range: 1–3 days). Most patients were usually discharged within 2 days after surgery with no statistically significant difference between the open and the laparoscopic groups (2 days versus 2 days, P = .945).
Discussion
VPS is a common procedure in neurosurgery, although its complication rate is high. The two main complications in children are mechanical shunt failure (70%) and infection (10%). Distal mechanical malfunctions are more common and comprise 25% to 30% of all mechanical failures and include CSF malabsorption resulting in secondary ascites, preperitoneal placing of the distal catheter, and distal catheter obstruction secondary to intra-abdominal adhesions and pseudocysts. 12
Common techniques for placing the distal catheter include open mini-laparotomy and the laparoscopically assisted procedure. The main drawback of the open technique is the uncontrolled placement of the distal catheter, especially in patients with peritoneal adhesions, such as those with a history of abdominal surgery. Over the past two decades, laparoscopic surgery has gained popularity for treatment intra-abdominal pathologies. The main advantages of laparoscopic surgery include the following: smaller incisions and thus reduced peritoneal and fascial incisions, less surgical trauma, shorter postoperative recovery, and fewer secondary peritoneal adhesions. 12
Using laparoscopy in distal shunt insertion enables placement of the abdominal end of the shunt under vision, thereby lowering the risk of immediate injury to the abdominal viscera, and decreasing the incidence of preperitoneal placement of the distal catheter. Other advantages include visual verification of CSF flow, although the spontaneous CSF flow may not be visible when the abdomen is insufflated possibly because of the high abdominal pressure (10–15 mm Hg) that may preclude spontaneous flow. Thus, pumping of the reservoir may be needed to verify the CSF flow. 13
Our results for an operative time in the laparoscopic group are similar to those reported in other studies evaluating the laparoscopy-approach only. Although the laparoscopic method was associated with a statistically significant lower operation time, the functional implication of the difference is trivial.
Technically, the implementation of laparoscopic approach creates a greater visual control of the distal tube position, allowing placement with minimal failure. Our results support this finding with a statistically lower rate of abdominal malposition (0% versus 4%; P = .001) observed in comparison with the laparotomy group. Phan et al. reported a similar result of distal shunt failure (8.9% versus 15.4%; P = .03) and abdominal malposition (2.8% versus 7.1%; P = .001). 15
Finally, technique modifications are ongoing. Recent examples include the single-port laparoscopic surgery performed by Hong et al. and a percutaneous minimal access insertion technique by Ochalski et al. that does not utilize the aid of laparoscope.16,17
Conclusion
The laparoscopically assisted insertion of a distal VP catheter is a safe, effective, minimally invasive, and technically easy approach for VPS placement in children. It allows definite insertion of the distal catheter in the peritoneal cavity and provides visual confirmation of the patency of the shunt system, minimizes omental adhesions and viscus perforation.
There was no statistically significant difference between the open and laparoscopic techniques regarding the length of hospital stay or infection rate. However, the laparoscopic technique in VPS surgery is associated with significantly reduced rate of abdominal malposition of the distal catheter compared with the open laparotomy technique. This finding is of great value in our locality (Upper Egypt), with low socioeconomic level and high incidence of distal shunt failure. Laparoscopically assisted insertion of the distal catheter is an alternative technique that may simplify and improve the safety of shunt surgery.