
Abstract
Abstract
Purpose:
Published results from mesh placement in the preperitoneal space between the posterior fascia and peritoneum for ventral hernia repair are limited. We describe our initial experience regarding the feasibility of a robotic-assisted transabdominal preperitoneal (rTAPP) ventral hernia repair.
Methods:
The study is a retrospective review and descriptive analysis of consecutive and prospectively collected data regarding rTAPP ventral hernia repair conducted by a single surgeon between 2014 and 2016.
Results:
Fifty-four consecutive rTAPP ventral hernia repairs were performed, and all but two cases were elective. Indications were: 41 primary ventral, 5 incisional, 3 lumbar, 2 Spigelian, 1 recurrent incisional, 1 combined flank and inguinal, and 1 combined primary ventral and inguinal. The mean operative time was 73 minutes (range 25–217 minutes). The average hernia defect was 9.7 cm2, whereas the average size of synthetic mesh was 178 cm2. Forty-six cases were completed through an rTAPP approach, and 8 were via partial rTAPP due to multiple peritoneal defects. Estimated blood loss was 5–10 mL. Forty-nine patients were treated on an outpatient basis. Two complications occurred: symptomatic seroma requiring aspiration in the office and rectus sheath hematoma requiring hospital readmission and blood transfusion.
Conclusions:
Our study results support the safe and effective placement of mesh in the preperitoneal space via the use of robotic technology, and they represent the largest single-surgeon series of robotic-assisted TAPP ventral hernia repair. Large, multicenter prospective trials could further elucidate the potential benefits and the long-term outcomes from this approach.
Introduction
L
Laparoscopic repair can be performed with the use of an intraperitoneal onlay mesh (IPOM) or by a transabdominal preperitoneal (TAPP) approach. In the IPOM approach, the direct contact of the composite mesh with the abdominal contents could potentially result in an inflammatory response and subsequent intestinal obstruction, chronic pain, and enterocutaneous fistulas.8–10 New composite meshes have an inert, adhesion-resistant substance on the visceral side and can potentially reduce the occurrence rate of these complications. 11
The TAPP approach confers the possible advantage of minimal adhesion formation, even with the use of a non-coated mesh, since there is no direct contact between the mesh and the intra-abdominal structures. 11 A recent study demonstrated the efficacy of the TAPP approach in ventral hernia repair. However, the approach has been associated with longer operative times, as development of the appropriate preperitoneal plane requires advanced laparoscopic skills. 11
The robotic-assisted approach has been proposed as an alternative method for ventral hernia repairs that involve mesh placement. 12 We describe the technical aspects and early outcomes from a single surgeon's experience with robotic-assisted TAPP (rTAPP) ventral hernia repair.
Materials and Methods
All patients who underwent rTAPP ventral hernia repair utilizing the da Vinci® Si robotic platform (Intuitive Surgical, Inc., Sunnyvale, CA) between January 2014 and September 2016 were included in this single-institution retrospective study. Institutional Review Board approval was obtained, and the first (consecutive) 54 cases were reviewed. Although the majority of the cases involved primary elective ventral hernia repairs, our study also included incisional hernias, flank hernia, lumbar hernia, combined ventral/inguinal hernias, and emergent cases. rTAPP ventral hernia was the approach of intent in our study.
Patient demographics and details related to the surgical procedure were collected and reported on predefined data collection forms by the surgeon or his designee. Surgical data included the dimension of the hernia defect, mesh type and size, and suture type used for fixation. The ability of the surgeon to close the fascial hernia defect (yes/no), the technique used, and the length of stay were also recorded. Conversion rate, perioperative outcomes, and complications (utilizing the Clavien-Dindo classification system) were collected as well. Hernia recurrence was defined as the absence of hernia on clinical exam and associated symptoms from a patient's standpoint during their clinic visits in the first month and after 3 months. In addition, a follow-up phone call was made 1-year post-procedure to ascertain whether the patients had any recurrence of the hernia or any associated symptoms.
Surgical technique
The patient was placed supine under general anesthesia. Three ports were used: An initial port (8.5 mm) was placed in the left upper quadrant. Two 8.5-mm ports were placed at least 8 cm from each other in the mid axillary line in the left lower quadrant and, importantly, at ∼8 cm from the edge of the planned flap or mesh. The robot was then docked on the right side of the patient. The ventral hernia was identified (Fig. 1), lysis of adhesions was performed (if necessary), and any intra-abdominal hernia contents were reduced into the abdominal cavity (Fig. 2). A measuring tape was used inside the peritoneal cavity to measure the dimensions of the hernia defect before closure. With the use of monopolar scissors and a bipolar grasper, the peritoneum was grasped at ∼5 cm from the hernia defect, the preperitoneal space was entered, and the peritoneal flaps were created in a 5-cm radius around the hernia defect (Fig. 3). Primary closure of the hernia defect was accomplished by running a long-lasting absorbable barbed suture (Stratafix 0™ on CT-1 needle, Ethicon, Somerville, NJ). Next, the assistant placed the folded mesh in the abdominal cavity via one of the ports. The robotic arms were used to unfold the mesh in the preperitoneal space; the mesh was secured to the posterior fascia by using barbed absorbable sutures (2–0 V-lock™; Medtronic, New Haven, CT), which ensured a mesh overlap of ∼5 cm in all directions. The peritoneal flaps were closed with running absorbable barbed sutures (2–0 V-lock; Medtronic) (Fig. 4). At the end of the procedure, the entire mesh was covered with the peritoneal flap.
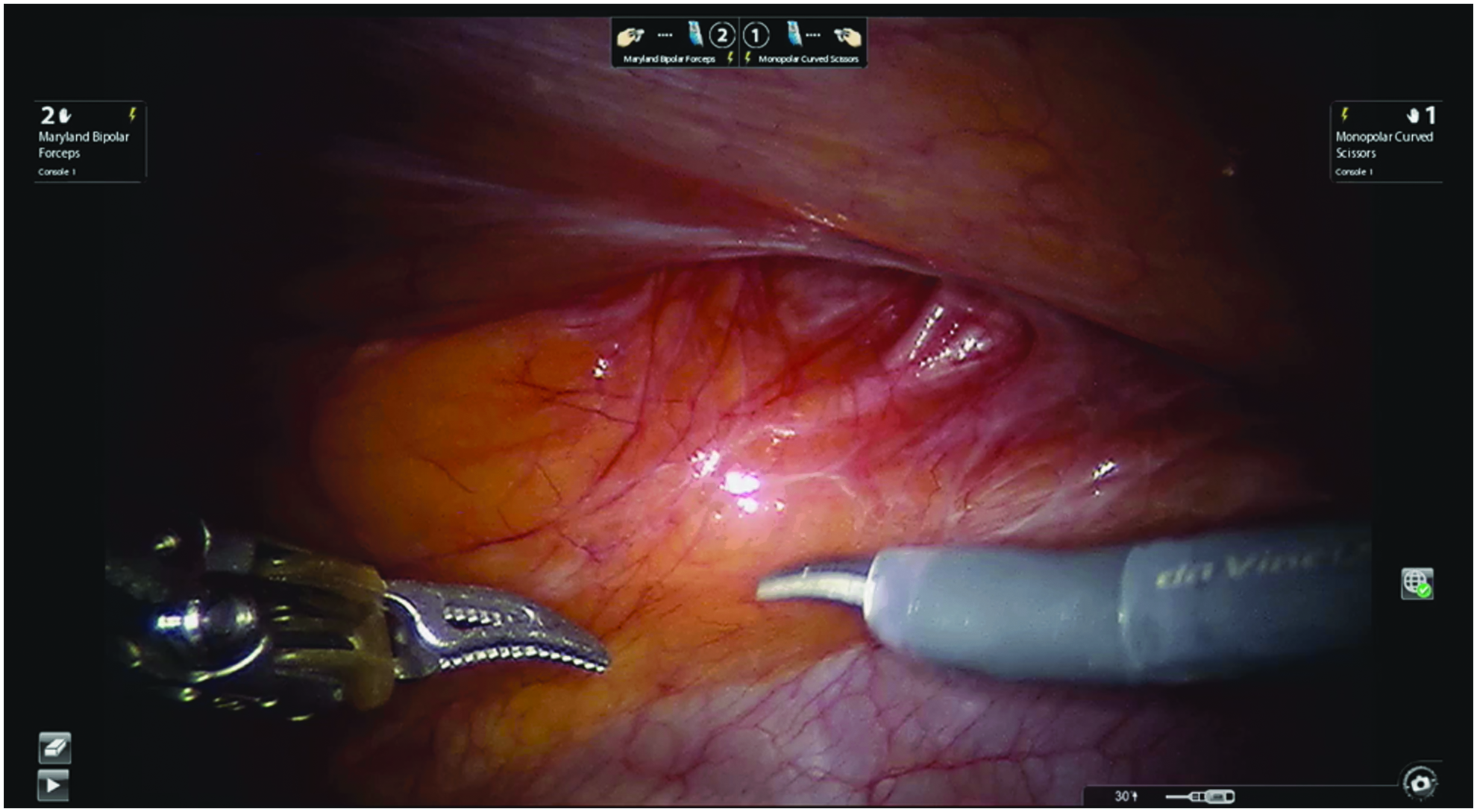
Identification of ventral hernia.
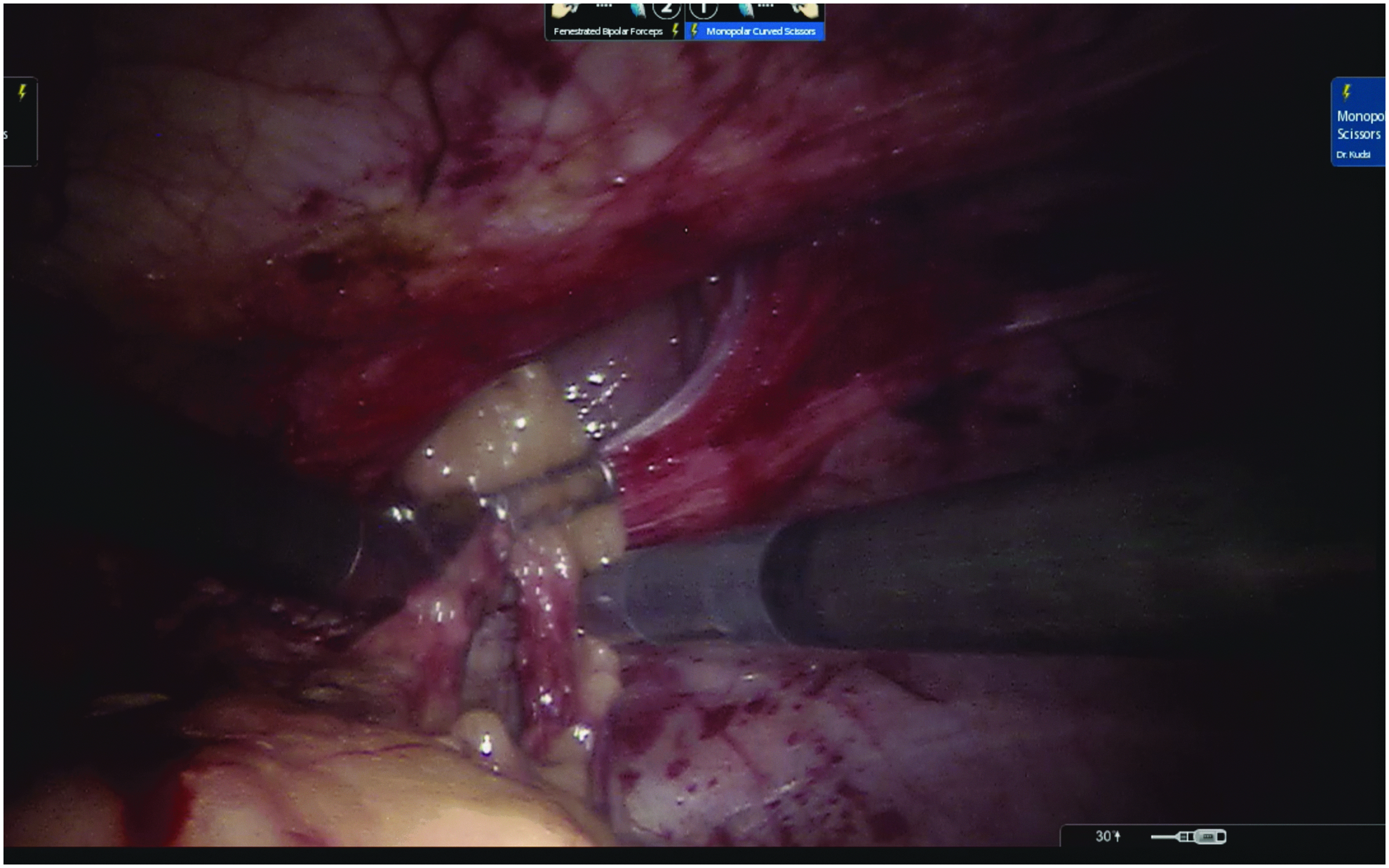
Reduction of hernia contents.
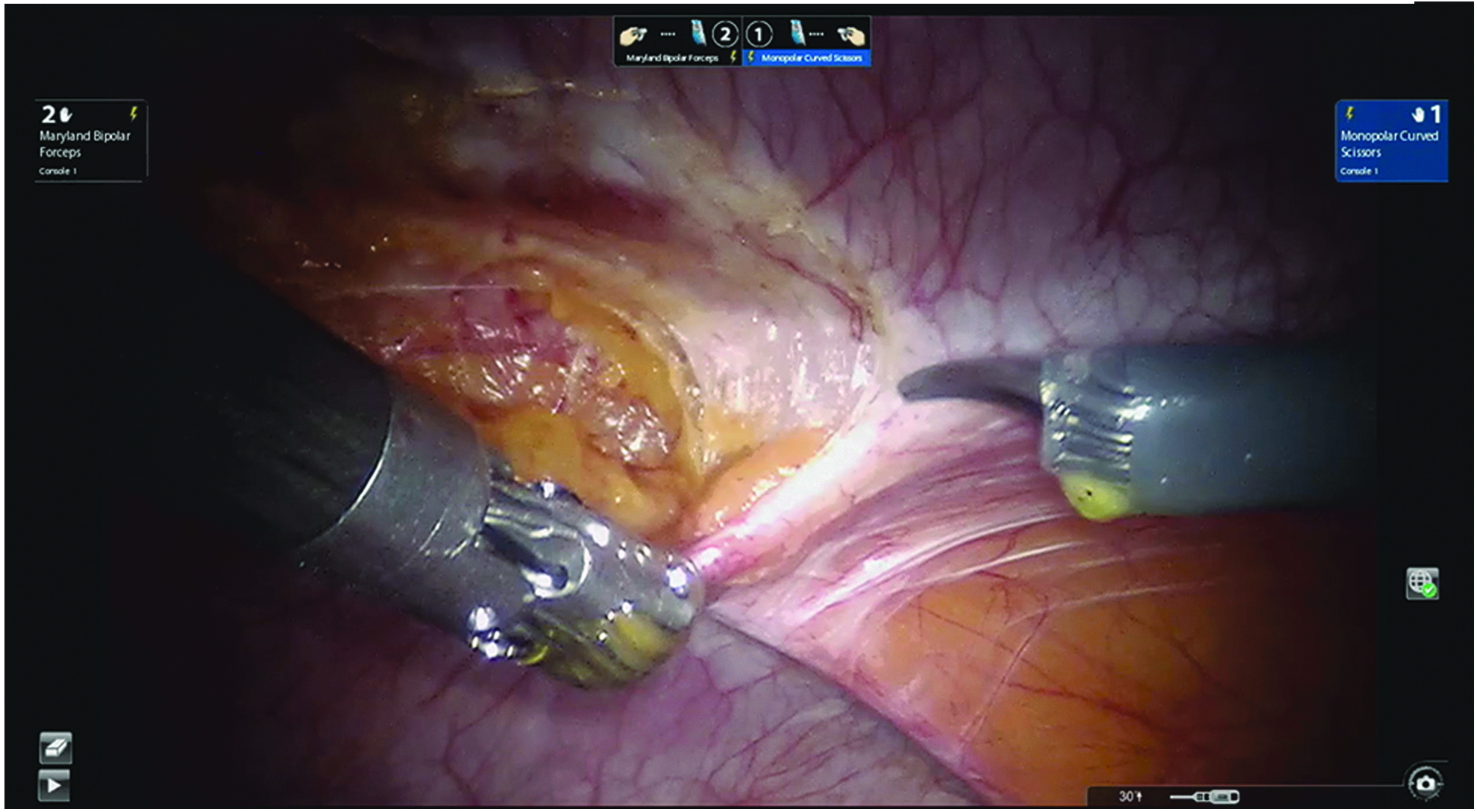
Creation of peritoneal flap.
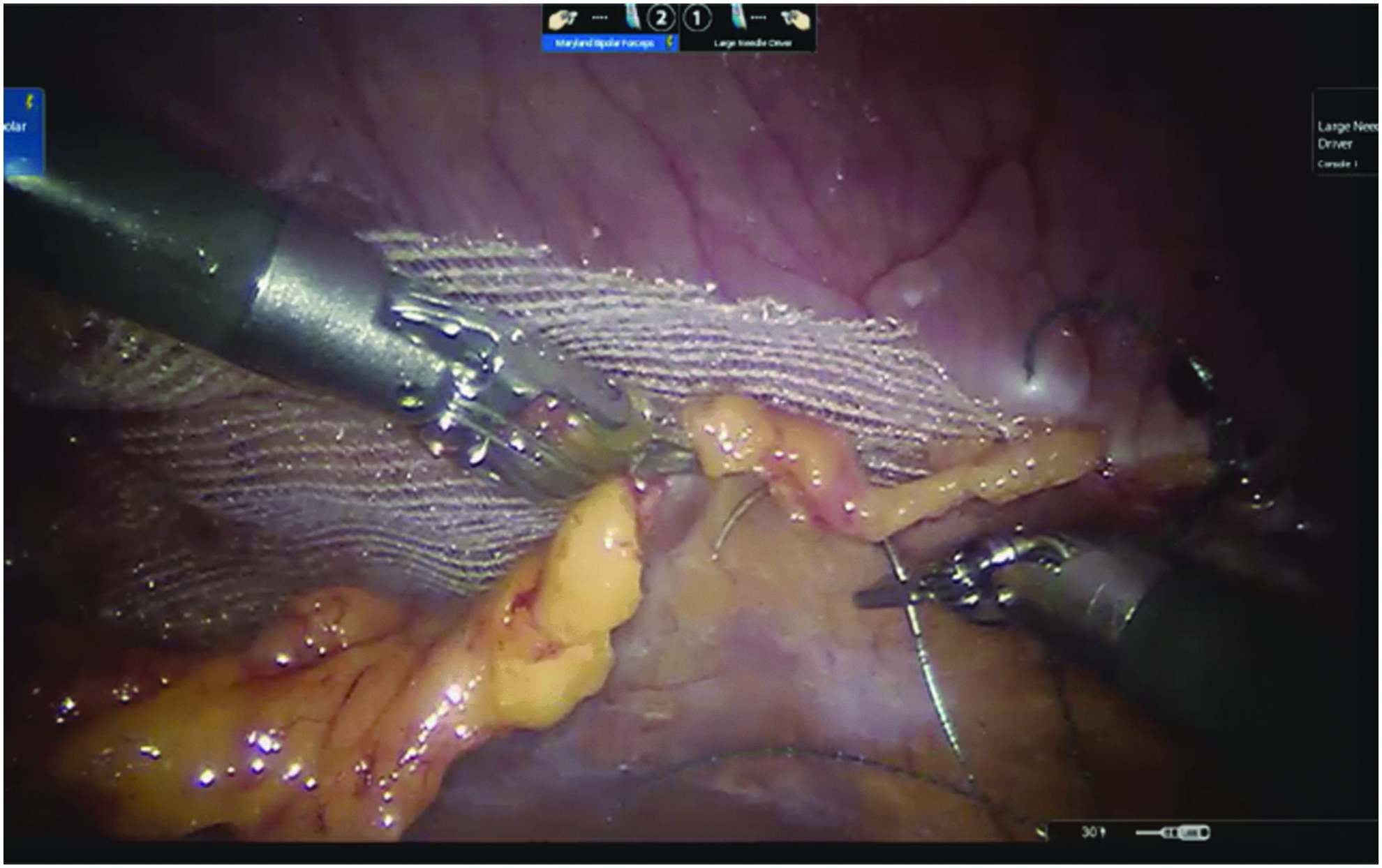
Closure of peritoneal flaps after mesh placement.
Statistical analysis
Descriptive statistics were applied throughout. Analyses were based on all reported data. Any unavailable or missing data were described as unknown and not included in the calculations. Analyses were made by using Microsoft Excel 2016 for the Mac.
Results
We performed a total of 54 consecutive robotic TAPP ventral hernia repairs by utilizing the da Vinci Si robotic platform. The mean age of our patient population was 49.9 ± 15.4 years, and 61.1% were men (Table 1). The average body mass index (BMI) was 32.1 kg/m2: 31 patients (57.4%) were obese (BMI ≥30 to <40 kg/m2), and 4 patients (7.4%) were morbidly obese (BMI ≥40 kg/m2). The majority of the study group (90.4%) was classified as the American Society of Anesthesiologists (ASA) 2 (Table 1).
ASA, American Society of Anesthesiologists; BMI, body mass index.
All cases were elective, with the exception of 2 (3.7%), which were emergent. These two patients presented to the emergency department with incarcerated ventral hernias, which required intervention within 24 hours. Both cases were completed via the TAPP approach: one with noncoated mesh and the second one with absorbable noncoated mesh because of bowel incarceration. Forty-six patients (85.2%) underwent primary ventral and incisional hernia repair with a mean operative time (skin-to-skin) of 66.0 ± 30.2 minutes. The remaining 8 patients had the following repairs: recurrent incisional hernia (n = 1), flank hernia combined with inguinal (n = 1), primary ventral hernia combined with inguinal (n = 1), lumbar hernia (n = 3), and Spigelian hernia (n = 2); the mean operative time (time from skin incision to skin closure) for these 8 repairs was 103.9 ± 64.4 minutes. The mean operative time for all 54 procedures was 73.0 ± 40.4 minutes, whereas the mean console time (time utilizing the robotic console) was 54.4 ± 31.1 minutes (Table 2).
TAPP, transabdominal preperitoneal.
The fascial defect was closed in all cases, and the average hernia defect was 9.7 cm2 (range 4–80 cm2). Synthetic mesh was used predominantly, with the exception of one case where an absorbable mesh was placed because of an incarcerated bowel within the hernia defect and concern for bacterial translocation. The most commonly used mesh was permanent synthetic (Progrip™; Medtronic), and the mean mesh size was 178 cm2 (range 81–450 cm2). Forty-six cases (85.2%) were completed entirely with the TAPP approach. The remaining 8 repairs (14.8%) were completed by using the IPOM approach given the numerous peritoneal tears and the need for composite mesh (Symbotex™; Medtronic).
No intraoperative complications—including bowel injury or blood transfusion—occurred. All the procedures were completed with robotic assistance without any conversion to open (Table 2). Most patients (n = 50) were discharged home on the procedure day. Four patients required hospitalization for 1–2 days: 2 cases were emergent and were watched for return of bowel function, 1 elective case involving combined flank hernia and bilateral inguinal hernia repair required an overnight stay as the patient lived alone, and 1 case required blood transfusion postoperatively. During the immediate 30-day follow-up period, 2 patients (3.7%) experienced complications. The first developed a seroma at the surgical site that was successfully aspirated at the office (Grade I in the Clavien-Dindo classification system), and the second patient suffered a rectus sheath hematoma that required hospital readmission and two units of blood transfusion. The hematoma spontaneously resolved and did not require surgical evacuation (Grade II in the Clavien-Dindo classification system). No surgical site infection was noted in any patient. All the patients (100%) reached their 1-year follow-up and, when contacted, reported no hernia recurrence.
Discussion
The long-term morbidity associated with open surgical ventral hernia repair has resulted in the development of different surgical techniques for the repair. Early reported primary closure of the fascial defect with an open approach resulted in high recurrence rates of up to 54%,13–15 whereas subsequent use of mesh in a tension-free repair resulted in significant decreases in hernia recurrence rates.13,14 One technique for mesh placement was the preperitoneal approach, and its use for ventral hernia repair was first described by Rives et al. 16 and Stoppa. 17 The preperitoneal approach has the benefit of no direct contact between the mesh and the abdominal contents; however, the drawback of high wound-associated complications has been significant and attributed most probably to the wide fascial dissection during the flap creation. 10
Laparoscopic approaches of mesh placement were developed to prevent open extensive fascial dissection. Prasad et al. 11 compared laparoscopic IPOM and TAPP mesh placement at their institution and concluded that TAPP is associated with longer operating times, possibly because it requires creation of peritoneal flaps and resuturing of the flap after mesh fixation. It was also reported that 2.3% of patients who underwent the IPOM procedure had prolonged pain compared with 1.4% of the patients who underwent the TAPP procedure; the difference was possibly due to the use of transfascial sutures rather than tacks. 11 Numerous other studies demonstrated an association between postoperative pain and transfascial suture use.18,19
The robotic approach imparts dexterity from the wristed instrumentation and three-dimensional optics. Compared with laparoscopic ventral hernia repair, these robotic features could facilitate the creation of peritoneal flaps and mesh fixation by suturing, making unnecessary the use of tacks or percutaneous transfascial sutures and decreasing the incidence of postoperative pain. An added benefit of the robotic approach is the ease of the fascial defect's closure, which traditionally has been the challenging component of a fully laparoscopic TAPP technique. Gonzalez et al. 12 demonstrated closure of the fascial defect in 69.3% of their cases via robotic primary ventral hernia repair, even during the surgeon's initial experience.
The decreased rate of surgical site infections after a minimally invasive approach to ventral hernia repair is a proven benefit compared with open interventions. Kaoutzanis et al. 4 reviewed 26,766 patients who underwent ventral and incisional hernia repair and reported that, after laparoscopic repair, the surgical site infection rate was 1.2% for reducible and 2.3% for incarcerated hernias. In a multicenter retrospective review of 368 patients who underwent robotic-assisted ventral hernia repair, Gonzalez et al. 12 reported that 1.4% of their study population developed surgical site infection. In our study, we identified no patients with surgical site infection; however, 2 (3.6%) surgical site complications (seroma and rectus sheath hematoma) were noted.
Sugiyama et al. 20 demonstrated the feasibility of robotic-assisted TAPP ventral hernia repair. They evaluated 3 patients who underwent preperitoneal mesh placement, which was secured with absorbable tacks to the abdominal wall, and the flap was closed with running locking sutures entirely covering the mesh. They reported no intraoperative or postoperative complications within 30 days after the procedure and no recurrences during 3 months of follow-up. However, they reported a mean operative time of 163.7 minutes. We recorded a mean operative time of 73 minutes (skin-to-skin).
This study has several limitations. This was a single-institution, retrospective study of procedures performed by one surgeon. More heterogeneous surgeon experience could provide additional value. Patient selection bias may be considered a limitation; however, the surgeon initiated each procedure with the TAPP approach in selected ventral hernia (average hernia defect was 9.7 cm2). The ventral hernia TAPP approach is not feasible in all patients and was not successful in 14.8% of our study population. This could be attributed either to inadequate preperitoneal fat for the performance of an appropriate dissection or to inability of the surgeon to create adequate flaps for mesh placement. This study was not designed to analyze learning curve or cost nor powered to measure pain control. However, all of the patients were prescribed Percocet (5/325 mg, 30 tablets) and none required refills of their pain medication. We were unable, however, to quantify the number of pills each patient took during the first 30 postoperative days. Also, our study did not evaluate the potential benefit that the TAPP approach might have in preventing adhesion formation. Chelala et al. shared their findings in their IPOM series after a second-look follow-up of 126 patients (9.5%): 45.23% were adhesion free, 42.06% had minor adhesions classified as Müller I, and 12.69% had serosal adhesions classified as Müller II. 21 Different radiologic tools, including ultrasonograpy and magnetic resonance imaging, have been described and could have been used to detect abdominal wall adhesions. 22 Our goal is to apply these tools in future studies to address the long-term benefits of the robotic-assisted approach.
Finally, the findings of this study are not compared or controlled with the more established laparoscopic technique for ventral hernia repair with preperitoneal mesh placement. The purpose of this study is to describe a novel approach that could be utilized to overcome the technical difficulties encountered by the laparoscopic approach. Luque et al. 23 recently published their experience utilizing a self-adhesive mesh for the laparoscopic ventral hernia repair via the TAPP approach. They reported that this is a safe and effective technique that results in less morbidity than the open approach and also less post-operative pain and complications compared with other laparoscopic ventral hernia repairs that use tacks for mesh fixation. However, they noted that the main disadvantages of this technique were the technical complexity of unrolling the mesh in a short space and the creation of preperitoneal flap. Our intention was to further investigate the use of robotic technology to decrease the limitation of the laparoscopic approach and achieve better outcomes. Luque et al. report an operative time of 57.3 ± 18 minutes with a complication rate of 26%. In our study, the operative time was similar (54.4 ± 31.1 minutes) with a decreased complication rate (3.7%). Although there was no direct comparison between a laparoscopic and robotic group in our study, the robotic-assisted TAPP ventral hernia repair might be associated with better outcomes than the laparoscopic counterpart, possibly due to the ability to identify (due to 3D optics) and easily create (due to the dexterity of the wristed instrumentation) preperitoneal flaps with minimal disruption of the anatomic planes. Our future goal is to directly compare the two groups and conclude which technique has better outcomes in a prospective manner.
Conclusions
Our study presents the largest single-surgeon series of robotic-assisted trans-abdominal preperitoneal ventral hernia repairs, with a follow-up reaching 1-year post-operatively. Our data support the safe and effective placement of mesh in the preperitoneal space via the use of robotic technology. Further multicenter prospective trials could further elucidate the potential benefits and the long-term outcomes.
Footnotes
Disclosure Statement
G.O. declares no conflict of interest. O.Y.K. declares conflict of interest not directly related to the submitted work. He has received personal fees from Gore, Intuitive, Medtronic, and Medrobotics outside the submitted work.