
Abstract
Abstract
Background:
Adjustable gastric banding and vertical banded gastroplasty are associated with the worst postoperative food tolerance of all bariatric techniques. However, food tolerance tends to improve over time. The aim of this study was to assess food tolerance and diet quality in patients undergoing a sleeve gastrectomy, 1 and 5 years after surgery.
Patients and Methods:
A prospective observational study of all the morbidly obese patients undergoing laparoscopic sleeve gastrectomy was performed. Food tolerance was assessed using the Quality of Alimentation questionnaire validated in bariatric patients.
Results:
Ninety-three patients were analyzed. One year after surgery, mean excess weight loss (EWL) was 81.1% ± 8.3%, and 5 years after surgery, mean EWL was 79.9% ± 6.4%. Preoperatively, 39.8% of patients perceived their eating patterns as good or excellent, 1 year after surgery, 79.6% and 5 years postoperatively, 86%. One year after surgery, the patients reported some difficulty in tolerance of rice, pasta, and red meat. Five years after surgery, these difficulties disappeared and very few patients just refer some tolerance difficulties with red meat. One year after surgery, 10% of the patients reported that they suffered postprandial vomiting often and 22% rarely. Five years postoperatively, only 8% of subjects describe rarely vomiting.
Conclusion:
After sleeve gastrectomy, the patients recognize an improvement in the quality of alimentation. During the first postoperative year, they present tolerance problems with rice, pasta, and red meat, and that disappeared 5 years after surgery.
Introduction
B
Food tolerance and diet quality may influence weight loss, improvement of comorbidities, and quality of life after bariatric surgery. Suter et al. defined good food tolerance as the ability to consume a variety of foods without difficulty and with minimal regurgitation or vomiting. 5 Poor tolerance is expected early after surgery, mainly secondary to tissue edema, but if persistent it may lead to food avoidance or maladaptive eating behaviors. This may result in eating habits, affecting overall diet quality, increasing the risk of nutritional deficiencies and compromising an adequate weight loss.6,7
Bad postoperative food tolerance has been reported for adjustable gastric banding and vertical banded gastroplasty. 6 Although sleeve gastrectomy is also a mostly restrictive procedure, several studies have reported that food tolerance is significantly better after sleeve gastrectomy than after gastric banding, and similar to Roux-en-Y gastric bypass 4 and a recently published article demonstrated similar food tolerance after gastric bypass and malabsorptive procedures. 8 Although food tolerance is obviously lower for patients after sleeve gastrectomy than for nonobese patients who had no surgery, 95% of them described food tolerance as acceptable to excellent. 9 Moreover, food tolerance tends to improve over time. The most restrictive effect with lower caloric intake and difficulties in tolerance of several foods is maintained during the first 2 years, but later on a significant improvement in food tolerance can be observed.4,10
The aim of this study was to assess food tolerance and diet quality in patients undergoing a sleeve gastrectomy, 1 and 5 years after surgery in a population following a Mediterranean diet postoperatively.
Patients and Methods
A prospective observational study of all the morbidly obese patients undergoing laparoscopic sleeve gastrectomy as bariatric procedure between October 2007 and June 2012 at University Hospital Miguel Hernandez, Elche, Alicante, Spain, was performed. Exclusion criteria were pregnancy at the moment of fulfilling each of the three questionnaires, diagnosis of cancer during the follow-up, and subjects undergoing a subsequent bariatric procedure for gastroesophageal reflux, failure of the initial bariatric approach, or complications derived from the technique. Deceased patients were also excluded. The study was conducted according to the Declaration of Helsinki and approved by the local Ethics Committee. All the patients signed an informed consent form to undergo the surgery and for the inclusion in the study.
Preoperative evaluation
A multidisciplinary team, including surgeons, endocrinologists, dieticians, endoscopists, radiologists, cardiologists, pneumologists, anesthesiologists, psychiatrists and psychologists, and specialized nurses, performed a combined medical, nutritional, and endocrinological workup to evaluate potential surgical candidates. Preoperative assessment included abdominal ultrasound, upper gastrointestinal endoscopy, cardiac ultrasonography, functional respiratory tests, and analytical evaluation of the nutritional status (vitamin and protein deficiencies). Psychiatrists and psychologists assessed additional interviews to evaluate the implication of the patient in following a strict diet in the postoperative course. The psychiatric evaluation is a selective filter to identify patients with a psychological background of mild to moderate alimentary disorders, and these subjects are required to undergo individual psychotherapy, trying to improve the psychological basis of the alimentary behavior. If this improvement is not achieved, they are discarded to undergo a sleeve gastrectomy and reevaluated by the multidisciplinary team to decide if they would be suitable for undergoing a Roux-en-Y gastric bypass or if even any kind of bariatric procedure would be appropriate for them.
A dietician established a diet consisting in a total daily energy intake of 1200 kcal, similar to that they have to follow after the operation and based on Mediterranean diet patterns. An excess weight loss (EWL) of at least 10% was considered an indispensable condition to be selected as candidate for laparoscopic sleeve gastrectomy, which is a standard eligibility criterion to undergo a sleeve gastrectomy at our institution. The patients who did not achieve this preoperative weight loss were rejected for undergoing a sleeve gastrectomy and reevaluated by the multidisciplinary team to decide if they could be candidates for a Roux-en-Y gastric bypass or if they should be discarded from the bariatric surgery program, given the absence of implication with a diet compliance.
Surgical technique
A longitudinal resection from the angle of His to ∼3–4 cm above the pylorus was performed using a 50-Fr bougie inserted along the lesser curvature. A staple line inversion was performed with a continuous oversewing of Polypropilene 3/0, before extracting the bougie.
The patients were discharged on a liquid diet for 2 weeks, then pureed diet for the following 2 postoperative weeks, and then advanced to regular meals under specific dietary instructions.
Follow-up
All the patients were followed up by the surgeon, the endocrinologist, and the registered dietitian 1, 3, 6, 12, 24, 36, and 60 months after surgery. Nutritional assessment and dietary counseling began 4–6 weeks before surgery, in individual and group sessions. After the first months postoperatively, patients were counseled to follow a balanced diet, that included adequate servings from all food groups, and in particular protein needs. The prescribed diet was based on Mediterranean diet patterns, with olive oil as the main source of lipids.
Medical treatment, such as antidiabetic and antihypertensive drugs, was adjusted according to the current needs of the patient. Postoperatively, daily proton pump inhibitor (Omeprazol 20 mg/day) and multivitamin supplements (Supradyn; Bayer®, Germany) were uniformly prescribed.
Variables
Body mass index (BMI) was obtained before operation and in postoperative determinations at 1 and 5 years after surgery. EWL was determined at 1 and 5 years after surgery, based on an ideal weight established by a BMI of 25 kg/m2. Food tolerance was assessed using the Questionnaire for quick assessment of food tolerance after bariatric surgery, validated by Suter in bariatric patients, 5 and modified by Ramon et al. for Spanish-speaking population. 11 The questionnaire is divided into four sections. Section 1 assesses satisfaction with the ability to consume food, with a score ranging from 1 (very poor) to 5 (excellent). Section 2 determines the time between meals and food intake between them. Section 3 evaluates the tolerance of eight types of food; a score of 2 indicates no difficulty with consumption, 1 indicates some difficulty, and 0 indicates that this food is not at all tolerated. Section 4 quantifies vomiting and regurgitation frequency, with the score ranging from 0 to 6, where 0 indicates daily, 2 indicates often, 4 indicates rarely, and 6 indicates never (Table 1). Mean final score of the questionnaire was obtained from the addition of the individual scores of sections 1, 3, and 4.
The patients must fill the questionnaire in the Outpatient Clinic before surgery, 1 and 5 years after the intervention.
Statistical analyses
All statistical analyses were performed using SPSS version 22.0 (SPSS, Inc., Chicago, IL). Results are expressed as mean ± standard deviation or number and percentages. Univariate analysis was performed with Chi-square test for categorical data and with Wilcoxon matched-pairs nonparametric test for continuous data.
The association between quality of alimentation and weight loss was analyzed with multiple Student's t-tests, evaluating the relationship between certain alimentation characteristics included in the Questionnaire for quick assessment of food tolerance after bariatric surgery and weight loss as a continuous variable.
A P value <.05 was considered statistically significant.
Results
A total of 100 patients were assessed for eligibility to be included in the study. Seven patients were excluded, 3 females were pregnant during one of the periods of questionnaire fulfillment, 3 patients required conversion to Roux-en-Y gastric bypass (2 due to uncontrolled gastroesophageal reflux disease and 1 for long-term weight regain), and 1 patient died in the postoperative course. Finally, 93 patients were included for analysis, 73 females (78.5%) and 20 males (21.5%), with a mean age of 45.7 years (range 19–68 years) and a preoperative BMI of 46.4 ± 7.9 kg/m2. Postoperative complications rate was 3%, including two staple line leaks, satisfactorily solved with an endoscopic stent, and one esophageal perforation in the middle third of the esophagus during the introduction of the bougie, that was also managed with an endoscopic stent placement, but the patient died in the postoperative course because of a massive pulmonary embolism, despite a correct thromboembolic prophylaxis.
Follow-up rate was 100% at 1 and 5 years postoperatively. One year after surgery, mean BMI was 28.5 ± 5.1 kg/m2 with a mean EWL of 81.1% ± 8.3% and 5 years after surgery, mean BMI was 28.9 ± 5.6 kg/m2 with a mean EWL of 79.9% ± 6.4%.
Quality of alimentation questionnaire
One hundred percent of the patients included for the analysis filled out the questionnaire at the preoperative, 1 and 5 years postoperative points.
Preoperatively, only 39.8% of patients perceived their eating patterns as good or excellent. One year after surgery, 79.6% of patients had a perception of having good or excellent eating patterns and 5 year postoperatively, this perception increases up to 86% (Fig. 1).
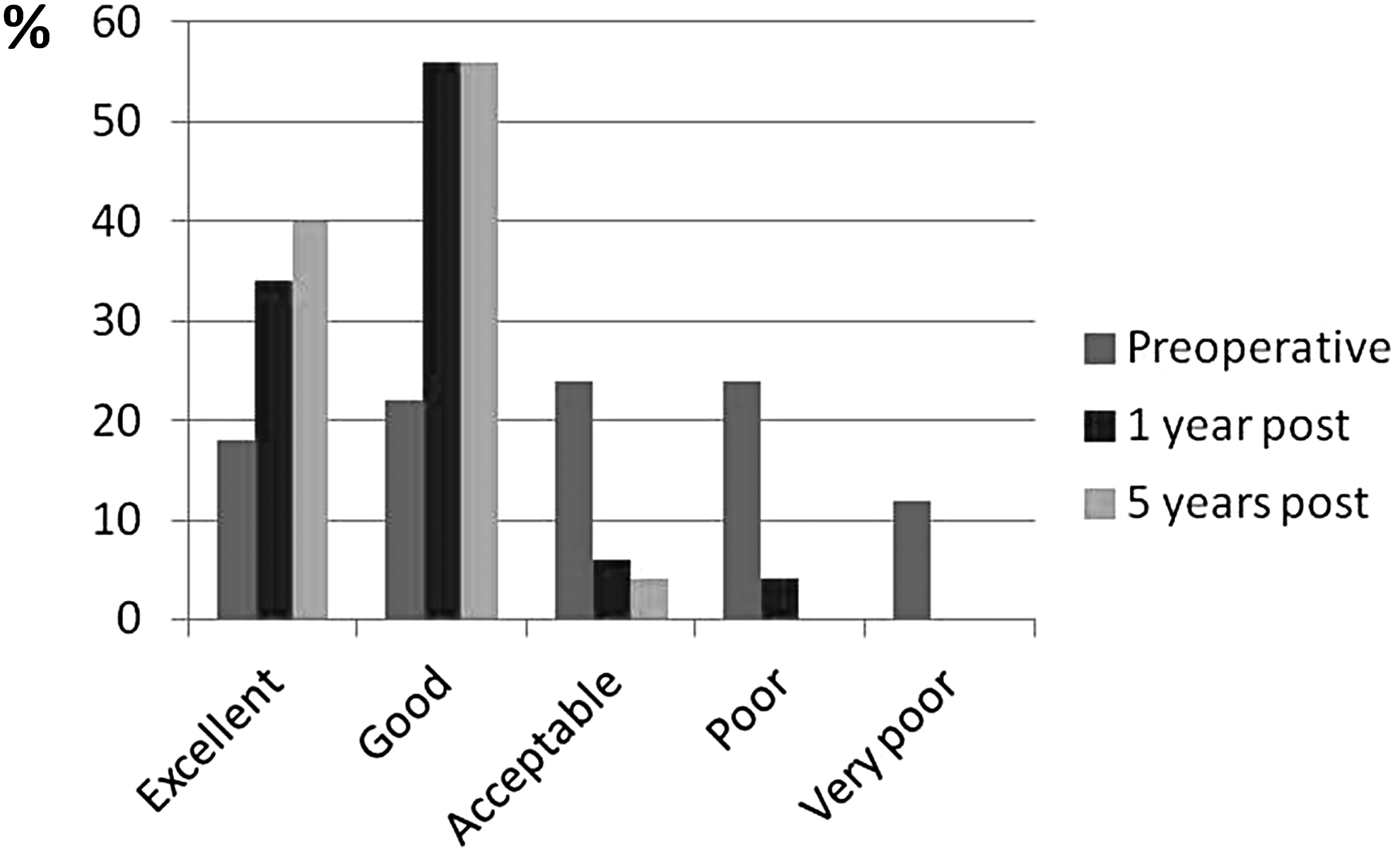
Overall satisfaction regarding how the patients can eat before surgery and 1 and 5 years postoperatively.
Preoperatively, median number of meals per day was 3 (range 1–7), while 1 and 5 years after surgery, the median number of meals was 5 (range 4–6).
Before surgery the daily main meal was dinner for 46% of the patients, while after surgery, dinner was the main meal in 18% of the cases (Fig. 2). Preoperatively, 92% of the patients recognize that they eat between meals, but 1 year after surgery, only 26% do this, and 30% do this 5 years postoperatively.

Daily main meal before surgery and 1 and 5 years postoperatively.
Referring to the tolerance of different types of foods, before surgery the patients did not refer tolerance problems with any of the analyzed foods. One year after surgery, the patients reported some difficulty in tolerance of rice, pasta, and red meat. Notwithstanding, 5 years after surgery, these difficulties mainly disappeared and very few patients just refer some tolerance difficulties with red meat (Fig. 3).
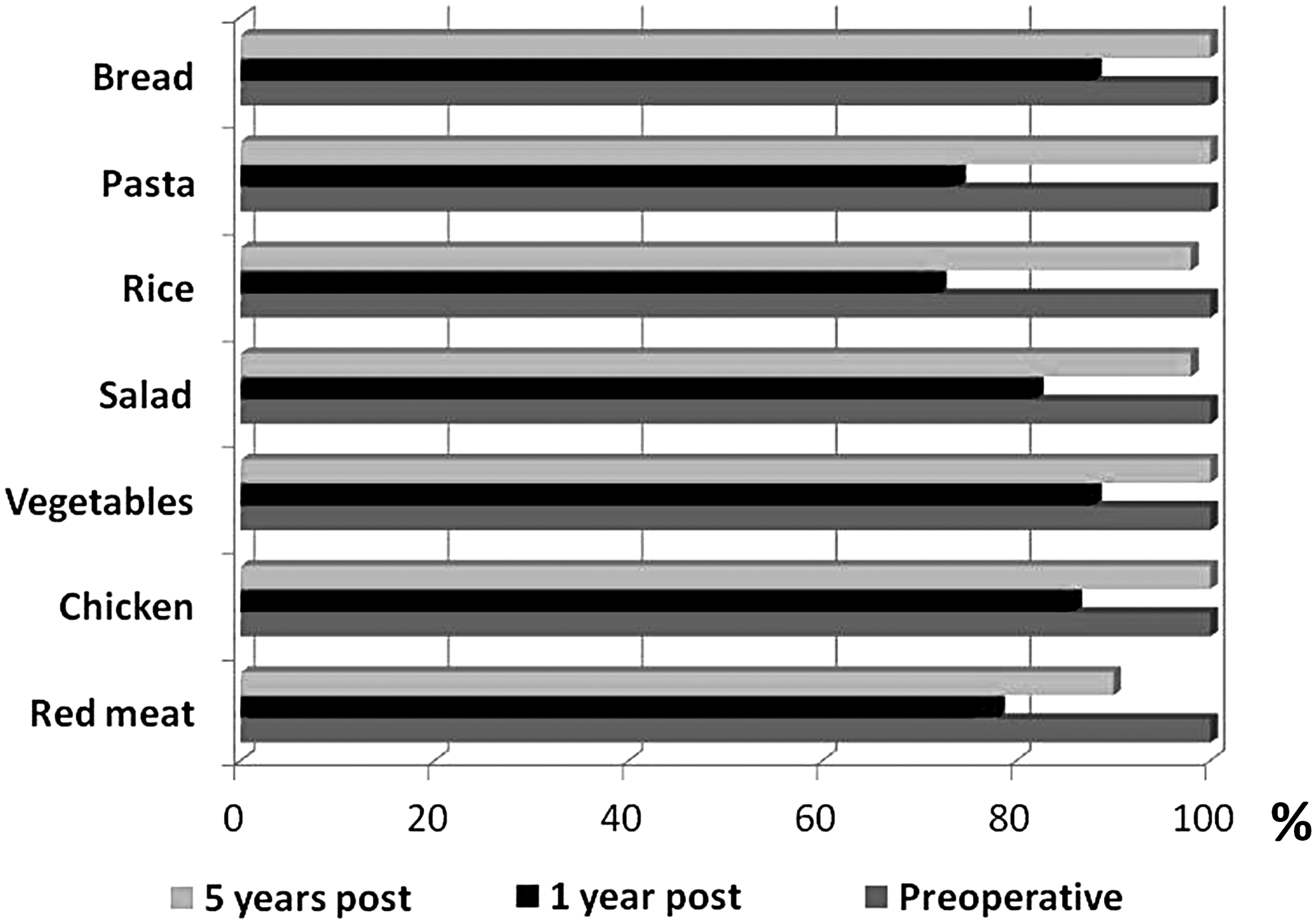
Tolerance of eight different foods before surgery and 1 and 5 years postoperatively.
One year after surgery, 10% of the patients reported that they suffered postprandial vomiting often and 22% rarely. Five years postoperatively, only 8% of subjects describe rarely vomiting.
Mean final score of the questionnaire was 23.4 before surgery, 21.3 one year postoperatively, and 24.2 five years postoperatively (Table 2).
Association between quality of alimentation and weight loss
A significant association between the different parameters of alimentation or satisfaction with eating patterns and food tolerance, with EWL at 1 and 5 years postoperatively could not be established.
Discussion
Several authors have reported that dietetic counseling is important in bariatric patients to achieve optimal weight loss and weight loss maintenance. It is true that the biological changes after surgery enable the patient to accept the recommendations from the dietitian, helping the patient not only to choose the foods that they feel hungry for but also the foods that decrease gastrointestinal symptoms. The change in food choices can be an important factor that determines the success of postoperative caloric restriction and weight loss.12,13 There is general agreement that reduction of volume of food plays a principal role in postoperative weight loss, but changes in what patients eat may also contribute. Morbidly obese patients usually consume a great amount of high-calorie food. They know that the consumption of such foods is inadequate, and therefore, they experience a higher level of dissatisfaction, as confirmed in the preoperative alimentary patters of our patients. Ignorance is not the problem of these patients, but a willpower to follow a healthy diet, which is mainly caused by psychological problems. 4 Thus, an exhaustive psychological evaluation, as performed in this study, is essential to identify potential disorders and to establish a correct therapy to improve them preoperatively, to optimize the results after a sleeve gastrectomy.
It has been hypothesized that a poor food tolerance is associated with lower EWL, as these patients might have an excessive intake of extras, including processed foods or sweets. The refined nature of these products may offer an easier consumption for postsurgical patients experiencing poor food tolerance.5,14 The involvement of a multidisciplinary team in the postoperative course is essential to prevent these incorrect attitudes. Surgeons, endocrinologists, and, specially, dietitians must perform a close follow-up with a specific optimization for food tolerance, with better degree of adaptation after surgery with the recommendations and correct monitoring. 15
However, despite a close and correct follow-up and counseling, sleeve gastrectomy implies anatomic modifications of the stomach, hindering a correct digestion of several foods. Bread, cereals, and red meat are described as the foods with greater digestion difficulty, 16 similar to the patients of our sample 1 year after surgery. Notwithstanding, the literature has demonstrated that with the passage of time, the feeding tolerance improves, and not only in sleeve gastrectomy but also in all bariatric procedures.5,14,17,18 In our patients, 5 years after surgery, the food tolerance was nearly similar to that reported preoperatively, including infrequent episodes of vomiting or regurgitation. It has been published that in Roux-en-Y gastric bypass, late postoperative is possible to have the same food tolerance than patients without having undergone bariatric surgery. 5
The inclusion of only selected patients in the study and the calibration of the sleeve with a 50-Fr bougie, larger than many other centers use, limit the generalizability of these results to other populations. Future studies must be conducted, including unselected patients undergoing sleeve gastrectomy and with other calibration bougie sizes, to confirm if the presented long-term results are only feasible with the patients and surgical techniques presented in this article.
Conclusion
After sleeve gastrectomy, the patients recognize an improvement in the quality of alimentation. However, during the first postoperative year, they present tolerance problems with rice, pasta, and red meat. In the late postoperative course, these tolerance problems disappear and they describe having a satisfactory eating behavior, without regaining the weight lost.
Footnotes
Disclosure Statement
No competing financial interests exist.