
Abstract
Abstract
Objective:
Short-term complications and long-term prognoses of three kinds of digestive tract reconstructions after radical gastrectomy for distal gastric cancer were compared.
Materials and Methods:
Patients who underwent radical gastrectomy for distal gastric cancer were divided into three groups according to the type of digestive tract reconstruction: Billroth I, Billroth II, and Roux-en-Y anastomosis. Clinicopathological characteristics, intraoperative conditions, short-term complications, and long-term prognoses were compared among the three groups.
Results:
There were no significant differences in the clinicopathological characteristics and postoperative complications among the three groups (P > .05). There was no significant difference in the operative times of the Billroth I and Billroth II anastomosis groups, but the operative times in both groups were shorter than the operative time in the Roux-en-Y anastomosis group (P < .05). The 5-year overall survival (OS) rate in the Billroth I, Billroth II, and Roux-en-Y anastomosis groups was 58.3%, 55.0%, and 62.2%, respectively, with no significant difference among the three groups. There was no significant difference in the OS rate according to the tumor node metastasis stage among the three groups (P > .05).
Conclusion:
The postoperative complications and prognoses were similar in the different digestive tract reconstruction groups. Billroth I anastomosis is a simple surgical method that can be used for gastrointestinal reconstruction after distal gastrectomy.
Introduction
G
Surgery is the main treatment for gastric cancer, but despite a combination of surgery, radiotherapy, and chemotherapy, the mortality rate continues to rise. 5 Although the incidence of proximal gastric cancer has risen in recent years, the gastric body and antrum remain the main sites of gastric cancer. 6 There are several methods of digestive tract reconstruction after distal gastrectomy for patients with cancer of the gastric body and gastric antrum. The most common methods are Billroth I, Billroth II, and Roux-en-Y anastomosis.7,8 There have been no studies of the prognosis for gastric cancer following digestive tract reconstruction.
In this study, short-term and long-term curative effects of three kinds of digestive tract reconstruction after distal gastrectomy for gastric cancer were retrospectively compared to obtain evidence for the selection of digestive tract reconstruction after distal gastrectomy.
Materials and Methods
Patients
From July 2012 to August 2014, clinical data on 328 patients who underwent distal gastrectomy at the Department of Gastrointestinal Surgery of the First Affiliated Hospital of Anhui Medical University were collected. There were 211 patients with gastric antrum cancer and 117 patients with gastric body cancer. The location of the tumor was determined by preoperative gastroscopy, computed tomography, or magnetic resonance imaging, in addition to the intraoperative diagnosis and postoperative pathological description (Table 1). All the patients were followed up by telephone or reexamination at the hospital. The clinical pathology and follow-up data were complete for all patients. Before surgery, none of the patients received anticancer therapy, such as chemotherapy. This study was performed in accordance with the requirements of the Declaration of Helsinki and was approved by the ethics committee of Anhui Medical University.
TNM, tumor node metastasis.
Digestive tract reconstruction
All patients underwent distal gastrectomy under general anesthesia. Some patients were anesthetized by general anesthesia combined with continuous epidural anesthesia. In accordance with surgical principles, R0 resection was performed in patients with stage I–III gastric cancer. R1 resection was confirmed by postoperative pathology in two patients. In 22 patients with stage IV gastric cancer, 18 patients underwent R0 resection for gastric lesions, 2 patients underwent R1 resection, and 2 patients underwent R2 resection. According to the digestive tract reconstruction methods, the patients were divided into three groups: Billroth I, Billroth II, and Roux-en-Y anastomosis.
Observation indices
The observation indices were as follows: (i) operative time and intraoperative blood loss; (ii) location and size of the tumor, depth of invasion, differentiation, and presence or absence of residual tumors in the margin; and (iii) retrieved lymph node number and tumor node metastasis (TNM) stage. Early postoperative complications included anastomotic leakage, anastomotic stricture, anastomotic bleeding, gastric paralysis, intraperitoneal hemorrhage, intraperitoneal infection, pulmonary infection, surgical-wound infection, incision dehiscence, intestinal mechanical obstruction, and inflammatory small bowel obstruction. Deaths in hospital and the causes of these deaths were recorded. In addition, OS from the date of surgery to death or the last follow-up was recorded. The last follow-up time was August 28, 2016.
Statistical analysis
SPSS 19.0 was used to analyze the data. All data were expressed as mean ± standard deviation. OS was analyzed by the Kaplan–Meier method. Comparisons among the groups were analyzed by the log rank test, t test, or χ2 test, with P < .05 considered statistically significant.
Results
Comparison of clinical data among the Billroth I, Billroth II, and Roux-en-Y anastomosis groups
There were 55 (16.77%), 131 (39.94%), 120 (36.59%), and 22 (6.71%) patients with stage I, II, III, and IV gastric cancer, respectively. Of these, 122, 98, and 108 patients underwent Billroth I, Billroth II, and Roux-en-Y anastomosis, respectively. There was no significant difference in the clinicopathological characteristics among the three anastomosis groups (P > .05). There were also no significant differences in intraoperative blood loss and retrieved lymph node number among the three groups (P > .05). Furthermore, there was no significant difference in the operative times of the Billroth I and Billroth II anastomosis groups, but the operative times in both groups were shorter than the operative time in the Roux-en-Y anastomosis group (P < .05) (Table 1).
Comparison of short-term complications among the Billroth I, Billroth II, and Roux-en-Y anastomosis groups
In the Billroth I, Billroth II, and Roux-en-Y anastomosis groups, 9, 12, and 11 patients, respectively, had complications, and there was no significant difference in complication rates among the three groups (P > .05). The complications mainly included anastomotic leakage, anastomotic bleeding, intraperitoneal hemorrhage, intraperitoneal infection, pulmonary infection, surgical-wound infection, gastric paralysis, and intestinal obstructions (Table 2).
Comparison of long-term prognoses among the Billroth I, Billroth II, and Roux-en-Y anastomosis groups
The 5-year OS rate in patients with TNM stage I, II, III, and IV was 90.9%, 70.8%, 41.7%, and 13.6%, respectively, and there was a significant difference in OS according to the different TNM stages (P < .05) (Fig. 1F). There was no significant difference in the prognosis of digestive tract reconstruction according to the disease stage (I–IV) (P > .05), as shown in Figure 1A–D. The OS rate in the Billroth I, Billroth II, and Roux-en-Y anastomosis groups was 58.3%, 55.0%, and 62.2%, respectively, with no significant difference among the three groups (P > .05) (Fig. 1E).
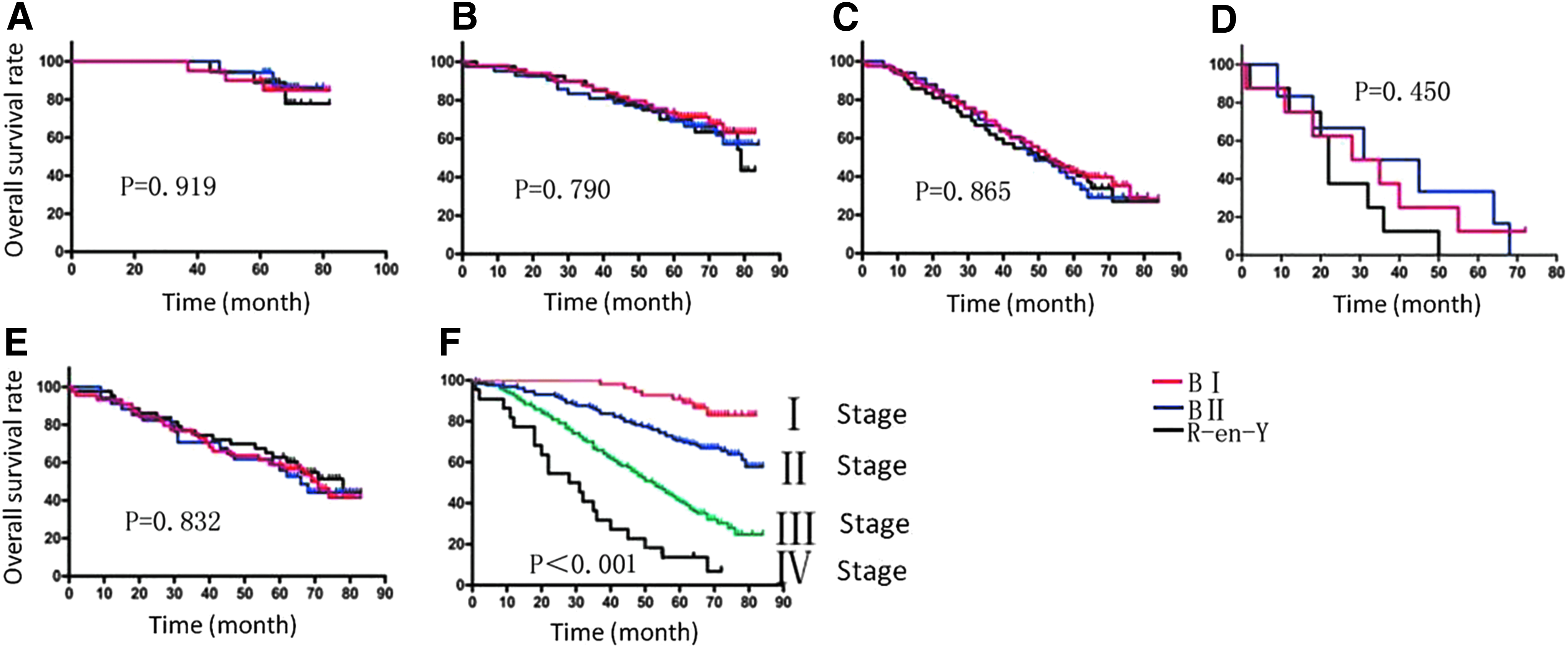
Comparison of survival curve in Billroth I, Billroth II, and Roux-en-Y anastomosis groups.
Discussion
Distal gastrectomy with lymph node dissection is the main surgical approach for cancer in the lower portion of the gastric body and antrum. 9 Billroth I, Billroth II, and Roux-en-Y anastomosis are common reconstruction methods for gastric cancer after distal gastrectomy.10–12 Opinions vary on the use of Billroth I anastomosis. In principle, Billroth I anastomosis is more suitable for distal benign gastric tumor and early distal gastric malignancies than for advanced gastric cancer.13,14 However, innovations in surgical instruments mean that it may now be possible to overcome difficulties associated with high gastroduodenal tension and that Billroth I anastomosis might be a suitable surgery for advanced gastric cancer. In the current study, the residual lesions of gastric stump and duodenal stump in the Billroth I group was similar to that in the other two groups, and the retrieved lymph nodes number was similar to that in the other two groups. Therefore, assuming that gastrectomy and lymph node dissection for distal gastric cancer are standardized, the method of digestive tract reconstruction will not affect the retrieved lymph node number or prognosis.
In the current study, several patients in the Billroth I group had gastric corpus cancer, raising a concern that Billroth I anastomosis might affect the success of the surgery and prognosis of the patients. However, the follow-up results showed that there was no significant difference in the 5-year OS rate among the Billroth I, Billroth II, and Roux-en-Y anastomosis groups (58.3%, 55.0%, and 62.2%, respectively; P > .05). Hence, Billroth I anastomosis is suitable for gastric corpus cancer.
After distal gastrectomy, the normal anatomic structure is altered, leading to postoperative complications, such as dumping syndrome and reflux esophagitis.15,16 Roux-en-Y anastomosis is thought to be an ideal method of digestive tract reconstruction after distal gastrectomy due to a reduced rate of postoperative gastroparesis. 17 However, in the current study, gastroparesis occurred in only one patient in the Billroth I group, and the symptoms in this case were relieved by conservative treatment for 4 weeks. There was no significant difference in the occurrence of postoperative gastroparesis among the Billroth I, Billroth II, and Roux-en-Y anastomosis groups. However, Roux-en-Y anastomosis is more complicated than the other two methods, with a higher number of anastomotic stomas.18,19 Additionally, the operative time in Roux-en-Y anastomosis is longer than in Billroth I and Billroth II anastomosis, with the shortest operative time achieved in Billroth I anastomosis.
In conclusion, there were no significant differences in lymph node dissection, postoperative complications, and overall prognosis among the three digestive tract reconstruction methods. As Billroth I anastomosis is easier to perform than Billroth II and Roux-en-Y anastomosis, it is a good choice for digestive tract reconstruction after distal gastrectomy. The present study was a single-center retrospective study and contained no data on disease-free survival. A multicenter study is needed to provide more evidence to guide the choice of digestive tract reconstruction after distal gastrectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.