
Abstract
Abstract
Background:
Transanal endoscopic microsurgery (TEM) has been accepted worldwide for the treatment of local rectal lesions. Rare rectal tumors consist of several different types of malignant or benign tumors. Surgical management is considered to be the only curative option. The aim of this study is to investigate the role of TEM in the treatment of rare rectal tumors.
Materials and Methods:
A total of 147 patients with rare rectal tumors underwent TEM in our center from April 2006 to May 2017. Clinical data were collected and a retrospective accurate database was constructed. Demographic characteristics, operative details, tumor details, complications, and follow-up data were analyzed.
Results:
Seventy-eight patients were male. Mean tumor diameter was 1.2 ± 0.7 cm and mean distance from the anal verge was 6.6 ± 2.3 cm. Full-thickness and complete resection with negative margins was achieved in all patients. Complications occurred in 3 patients during surgery and in 20 patients after surgery. Histopathologic results were neuroendocrine tumors in 104 patients; gastrointestinal stromal tumors in 35; melanoma, lymphoma, and leiomyoma each in 2; lipoma, and squamous carcinoma each in 1. One hundred thirty-five patients were followed up for 49.3 ± 33.2 months. Two patients died, 1 had local recurrence and 1 had a rectovaginal fistula 1 month after surgery. No local recurrence or metastasis, or fecal incontinence was observed in the remaining patients.
Conclusion:
TEM is an optimal treatment option for selected rare rectal tumors. The complication rate is low and the therapeutic effect is satisfactory.
Introduction
T
Total mesorectal excision (TME) has been widely accepted as a routine procedure for the treatment of rectal cancer for its low rate of local recurrence and excellent long-term survival. 5 However, both low anterior resection and abdominoperineal resection with TME can be followed by high perioperative mortality and morbidity, such as sepsis, anastomotic leakage, and bowel dysfunction. Transanal endoscopic microsurgery (TEM) was first introduced in 1983 by Dr. Gerhard Buess, 6 and has been accepted worldwide for the treatment of local rectal tumors, including benign and selected malignant lesions. TEM is superior to traditional TME in terms of safety.
Most previous studies on TEM are about adenoma and early-stage adenocarcinoma. Research on rare rectal tumors has only focused on one of the tumors, with NET being the most commonly reported one. Only a few reports are available on different types of rare rectal tumors. 7 To determine the role of TEM in the treatment of rare rectal tumors, we designed a retrospective clinical study, collected data in our center, and herein present our 10 years clinical experience.
Materials and Methods
Patients
A total of 593 patients underwent TEM for rectal lesions in our center from April 2006 to May 2017. All pathological specimens were studied by 2 independent pathologists and 147 patients were identified as having rare rectal tumors. All patients provided written informed consent, and the study was approved by the institutional review board for studies in humans. Clinical data were collected from both inpatient and outpatient medical records. A retrospective accurate database was constructed. Demographic characteristics, operative details, tumor details, complications, and follow-up data were analyzed.
All patients underwent physical examination and colonoscopy. Endorectal ultrasonography and/or rectal magnetic resonance imaging (MRI) were performed for each patient to exclude lymph node metastases. Computed tomography (CT) was performed to exclude distant metastases. Tumors were described by location, diameter, and distance from the anal verge. Oral laxatives were administered to patients the day before surgery for bowel preparation. Prophylactic antibiotics were administered via a peripheral vein before anesthesia induction. All patients underwent the surgery under general anesthesia in the lateral, prone, or lithotomy position with the tumor downward. The TEM equipment (Wolf, Tübingen, Germany) was installed after gentle dilatation of the anal sphincter. The detailed surgical procedures are shown in Figure 1. Under general anesthesia, a urinary catheter was placed in all patients and removed on postoperative day 1 or 2. All patients were allowed semi-liquid diets on postoperative day 1 and most were discharged on postoperative day 2 or 3.
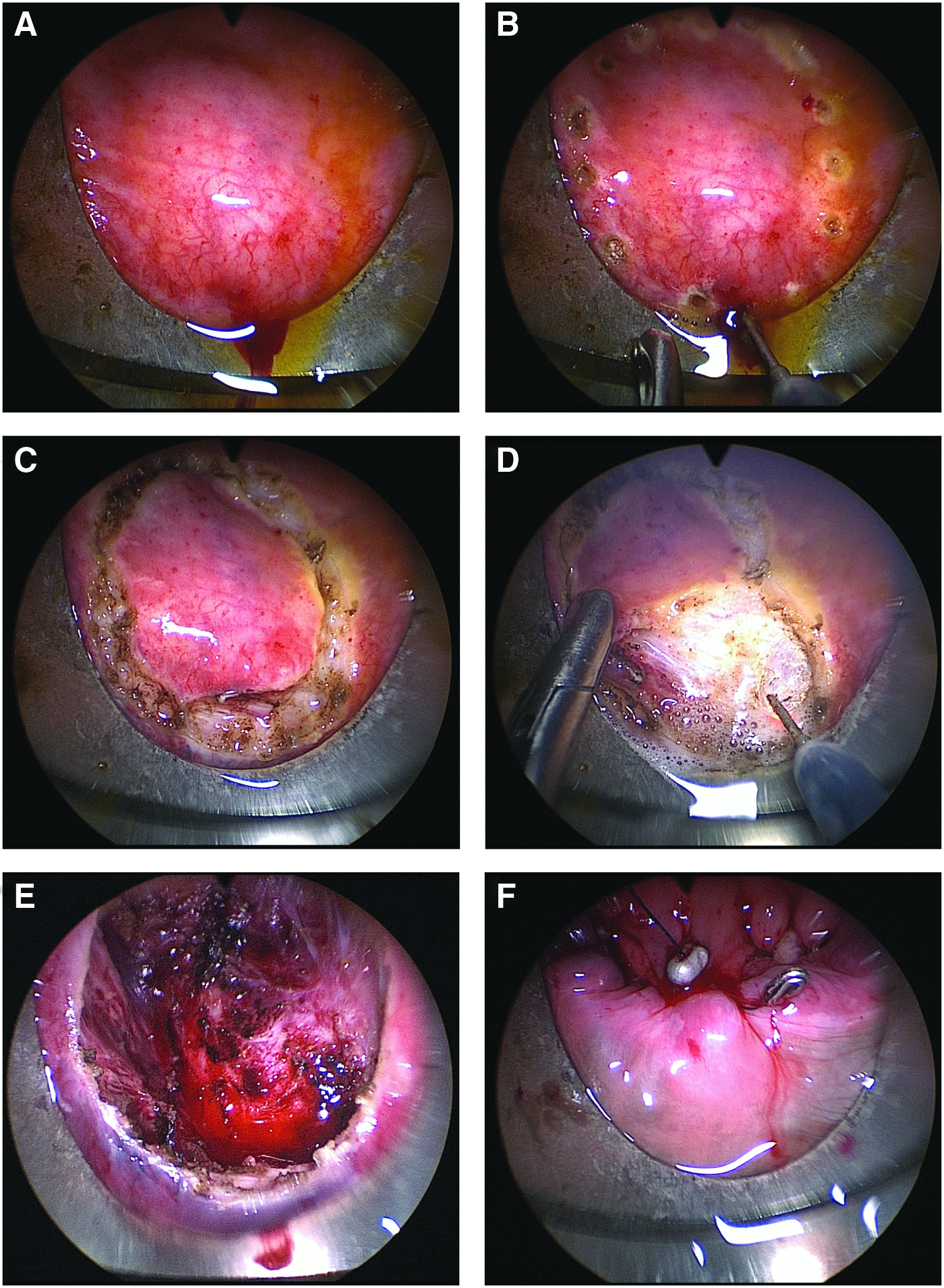
Detailed surgical procedures of TEM.
Statistical analysis
The Statistical Package for Social Sciences software (version 19.0; SPSS, Chicago, IL) was used. Linear variables were presented as mean ± standard deviation, and categorical variables were described by frequency. Differences between study groups were analyzed by χ2 test, Fisher's exact test, and Student's t test as appropriate. A P value <.05 was considered statistically significant.
Results
One hundred forty-seven patients with rare rectal tumors underwent TEM from April 2006 to May 2017. Seventy-eight patients were male (53.1%) and 69 were female (46.9%) with a mean age of 51.8 ± 12.1 years (range, 24–85 years). Ninety-two patients (62.6%) were asymptomatic and were diagnosed with rectal lesions incidentally or during routine physical examination. Other patients had preoperative symptoms such as alteration in bowel habit (17/147, 11.6%), hematochezia (13/147, 8.8%), abdominal pain (12/147, 8.2%), perianal discomfort (8/147, 5.4%), and diarrhea (5/147, 3.4%). Tumors were located anteriorly in 55 patients, posteriorly in 66, and in the lateral rectal wall in 26. Mean tumor diameter was 1.2 ± 0.7 cm (range, 0.2–5.3 cm) and mean distance from the anal verge was 6.6 ± 2.3 cm (range, 2–12 cm).
Full-thickness and complete resection with negative margins was achieved in all patients. Lymphadenectomy was not performed. Mean operative time was 60.2 ± 20.4 minutes (range, 25–120 minutes) and mean blood loss was 11.8 ± 6.5 mL (range, 2–25 mL). No conversion to laparotomy or laparoscopic surgery occurred. The operation was uneventful in 144 (98.0%) patients. Perforation occurred in 2 patients during surgery. The rectal wall defect was primarily repaired with TEM technique. Rectovaginal fistula was observed in 1 patient. Temporary transverse loop colostomy was performed after the repairing.
Mean postoperative hospital stay was 2.8 ± 1.6 days (range, 1–12 days). There was no early postoperative mortality. Postoperative complications occurred in 20 patients, including fever in 12, hemorrhage in 3, diarrhea in 3, urinary retention in 1, and pneumonia in 1. Fever, diarrhea, and pneumonia were resolved by antipyretic, antidiarrheal, and antibiotic agents, respectively. Urinary retention was treated by catheterization. One of the patients with hemorrhage was returned to the operating room for transanal hemostasis. The others recovered without surgery or blood transfusion. According to the Clavien-Dindo classification of surgical complications, 8 13 patients were classified as grade I, 6 patients as grade II, and 1 patient as grade IIIb. Postoperative morbidity rate was 13.6%.
Postoperative histopathologic results were NETs in 104 patients, GISTs in 35 patients, melanoma in 2 patients, lymphoma in 2 patients, leiomyoma in 2 patients, lipoma in 1 patient, and squamous carcinoma in 1 patient (Figs. 2 and 3).

Specimens of different rare rectal tumors after TEM.
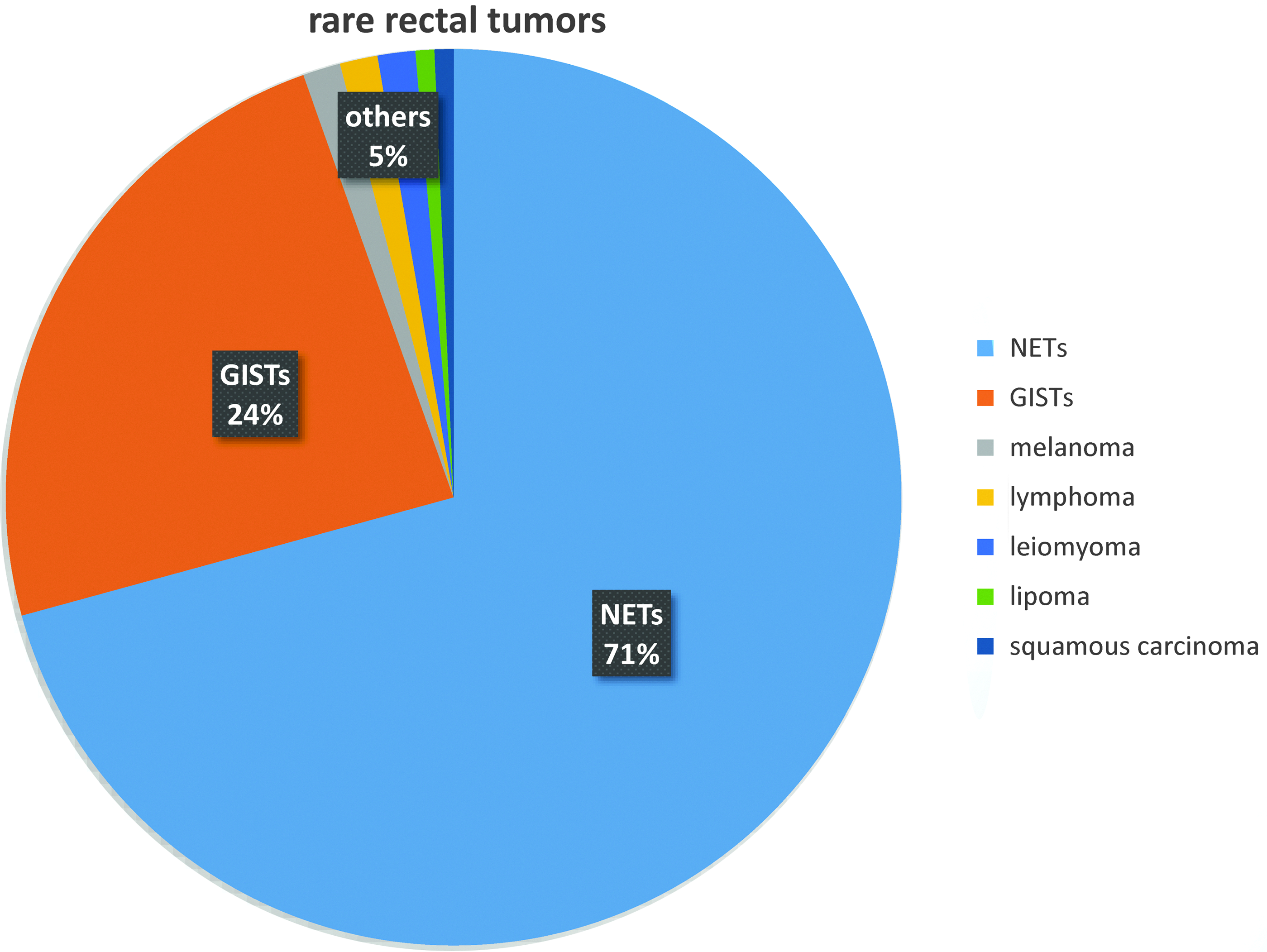
Percentage of different rare rectal tumors. NETs account for 71%, GISTs account for 24%, and all others account for 5%. GISTs, gastrointestinal stromal tumors; NETs, neuroendocrine tumors.
In the subgroup with NETs, 72 patients underwent TEM for primary tumor excision, while 32 patients had received previous endoscopic resection in other hospitals and were admitted to our center for a complete resection due to positive margins. Physical examination and colonoscopy were performed to determine the lesion location. The detailed data and statistical differences between patients with primary or complete surgery are shown in Table 1. In patients who underwent remedial complete resection, tumor remnants were confirmed in 53.1% (17/32). Vessel invasion was found in one of the patients with grade II disease and he was readmitted 2 weeks after TEM and underwent laparoscopic anterior resection.
Seventeen patients had residual tumor.
A, anterior wall; CR, complete resection; L, lateral wall; M, mucosa; MP, muscularis propria; P, posterior wall; PE, primary excision; S, submucosa; TEM, transanal endoscopic microsurgery.
In the subgroup with GISTs, 12 patients received neoadjuvant therapy before surgery with 400 mg imatinib mesylate (Gleevec) once daily for 6 months. The inclusion criteria for neoadjuvant therapy were unclear adhesions between tumor and surrounding tissues, oversized tumors, and a high mitotic index (>5 high power fields). Abdominal and pelvic MRI and endorectal ultrasonography were performed to evaluate the effect of neoadjuvant therapy. The detailed data and statistical differences between patients with and without neoadjuvant therapy are shown in Table 2.
Before neoadjuvant therapy.
After neoadjuvant therapy.
A, anterior wall; L, lateral wall; P, posterior wall.
As of August 2017, 135 patients (91.8%) had been followed up for 49.3 ± 33.2 months (range, 3–122 months). Physical examination, colonoscopy, rectal MRI, and abdominal CT were performed during the follow-up period. Two patients with melanoma died during the follow-up period due to tumor metastasis, 6 and 14 months after surgery. One patient with squamous carcinoma had local recurrence 10 months after surgery and underwent a second surgery of abdominoperineal resection and had a tumor-free survival of 5 months up to last follow-up. One patient with GIST had a rectovaginal fistula 1 month after surgery, was readmitted, and underwent temporary transverse loop colostomy. The stoma was closed 7 months later. No local recurrence or metastasis, or fecal incontinence was observed in all other patients.
Discussion
Rare rectal tumors consist of several different types of malignant or benign tumors. Their characteristics, treatment mode, and prognosis differ greatly from rectal adenocarcinomas. 4 Surgery is the main choice in multimodality therapy. Some rare rectal tumors require radical resection, such as NETs >2 cm, lymphoma, squamous carcinoma, and any with local lymphatic metastasis. Some other types only require local resection, such as GISTs, leiomyoma, and lipoma. In addition, some patients choose local resection instead of radical resection to retain the anus and avoid permanent stoma.
TEM is a very viable alternative to the local resection of rectal tumors. It has been shown to have lower postoperative morbidity rates than radical resection and transanal excision.9,10 In this study, 20 patients (13.6%) were found to have postoperative morbidity. Most of these patients (12/20) were considered to have absorption fever, and only 7 patients (4.8%) had grade II or higher complications according to the Clavien-Dindo classification. Furthermore, no conversion to laparotomy or laparoscopic surgery occurred. TEM has also been proved to have lower recurrence rates than transanal excision. 10 It can provide a magnified visual view and a wider operative field that results in clear resection margins, less fragmentation, and an accurate surgical plane.11,12 Full-thickness resection and negative margins were achieved in all patients in this study, and only 1 patient (0.7%) had local recurrence.
There has been a significant increase in the incidence of NETs worldwide.13,14 This may be attributed to the widespread use of colonoscopy. The rectum is the most common site of gastrointestinal NETs among Asian patients.15,16 The standard treatment for rectal NETs is still controversial. Radical resection and TME are recommended for rectal NETs ≥20 mm.17–20 For rectal NETs <20 mm, especially for those 11–19 mm in size, endoscopic resection, transanal resection, TEM, and radical resection are all appropriate.21,22 For endoscopic resection, incomplete resection such as residual tumor and positive margins are intrinsic limitations. The rate has been reported to be 24%–42%.23,24 For traditional transanal resection, poor exposure of the surgical field and limited operative distance from the anus are inevitable. In addition, radical resection is associated with a high incidence of complications. Hence, TEM is the preferred procedure in our center for rectal NETs <20 mm without distant or lymph node metastases. The rate of free resection margins reached 100%, even in patients with tumors invading the submucosa and muscular layer. Furthermore, patients who had received previous endoscopic resection also benefitted from TEM. Operative time, blood loss, and postoperative hospital stay were not significantly different between patients who had primary excision and complete resection. In this study, all NETs were well-differentiated grade I or grade II tumors. Strict inclusion criteria also ensured the treatment effect.
GISTs of the rectum are mostly located in the middle and lower section.25,26 Lymph node metastasis is quite rare. 27 This makes rectal GISTs especially eligible for TEM. In our series, tumor size ranged from 0.2 to 5.3 cm, distance from the anal verge ranged from 2 to 10 cm, and tumors were located on different walls of the rectum. However, all tumors were successfully resected by TEM, and no recurrences were observed. Thus, TEM is suitable for different types of rectal GISTs. Negative margins and R0 resection with complete tumor capsule are important in the treatment of GISTs. If the tumor is too large, TEM would be challenging due to limited operating space. Several studies have confirmed the safety and curative effect of imatinib.28–30 In addition, tumor shrinkage has been proved to benefit function preservation and the feasibility of local excision. 31 Twelve patients received neoadjuvant therapy before surgery in our study. The tumor sizes were reduced from 3.1 ± 1.2 to 2.6 ± 1.2 cm, which made surgery easier and safer. No significant differences in operative time, blood loss, or postoperative hospital stay were found between patients who did and did not receive neoadjuvant therapy. During the follow-up period, no recurrences or sphincter dysfunction were observed. Previous studies have also shown the advantages of TEM combined with imatinib in the treatment of rectal GISTs.32,33
All other tumors only account for 5% of rare rectal tumors. Rectal melanoma is an uncommon tumor with a poor median survival of 24 months. 34 Most patients die of metastases as there is no recognized treatment guideline due to its low incidence. 35 In this study, 2 patients with melanoma chose TEM because of severe underlying diseases and provided written informed consent before surgery. Primary rectal lymphoma is the third most common cause of rectal cancer following adenocarcinoma (90%–95%) and carcinoid (5%). 36 Surgery is generally reserved for clinical indications such as bleeding and bowel obstruction. 37 The 2 patients in this study with rectal lymphoma were asymptomatic. They underwent surgery due to rectal nodules and were diagnosed with lymphoma by postoperative pathology. The other 4 patients were also diagnosed postoperatively with leiomyoma, lipoma, and squamous carcinoma, respectively. TEM is not only a treatment method but also a diagnostic approach for these patients.
TEM is now accepted by more surgeons following more than 30 years of development. Its indications are constantly being expanded, and include the distance from the lesion to the anus, and the types of tumors.7,38 This study presented our 10 years of clinical experience in TEM and expanded its indication in different tumor types. However, this study still has some limitations, such as lack of a control group and its retrospective nature. In addition, NETs accounted for 71% of tumors in these patients, which may have resulted in some bias. Prospective, randomized, controlled and multicenter clinical trials are required to provide further supporting evidence with greater reliability.
In conclusion, TEM is an optimal treatment option for selected rare rectal tumors. It is suitable for rare rectal tumors with different locations, diameters, and distances from the anal verge. Short operative time, less bleeding, and short postoperative hospital stay were achieved. TEM can result in full-thickness and complete resection with negative margins. The complication rate was low and the treatment effect was satisfactory. Patients who have received previous endoscopic resection can also benefit from TEM. For selected patients, TEM can also be performed for palliative therapy and diagnosis.
Footnotes
Acknowledgments
This work was mainly conducted by Dr. X.W. and Prof. G.L. We would like to express our sincere gratitude to those who offered us valuable help, especially Professor Bin Wu and Professor Yi Xiao. We also thank the patients for their cooperation in the follow-up and for allowing us to report this study.
Authors' Contributions
X.W.: data acquisition and analysis, drafting the article; G.L.: conception and design of the study, drafting the article, surgeon for operations; H.Q.: design of the study, surgeon for operations; J.Z.: data collection and interpretation.
Disclosure Statement
No competing financial interests exist.