
Abstract
Abstract
Background:
The majority of submucosal tumors (SMTs) are benign. However, large SMTs with irregular outer shapes are proved to harbor a higher risk for malignancy. Submucosal tunneling endoscopic resection (STER) has emerged as a feasible technique for resecting SMTs.
Objective:
To evaluate the safety and efficacy of STER for large and irregular SMTs with a diameter no <35 mm originating from the muscularis propria layer, and to share the technical skills of STER for complete and en bloc resection.
Patients and Methods:
We retrospectively reported 10 cases in which the new technique of STER was performed to remove large and irregular SMTs with a diameter no <35 mm of upper gastrointestinal tract in our hospital between April 2014 and April 2017.
Results:
All 10 (100%) patients underwent STER successfully, with a mean operation time of 156 minutes. Among the 10 SMTs, 3 (30%) were located in the esophagus, 7 (70%) were in the cardia. All the SMTs had a maximum diameter no <35 mm, ranging from 35 to 100 mm. The mean size was 57.2 mm. En bloc resection was achieved in 8 (80%) of the tumors. Only two (20%) of the SMTs were resected into more than one piece. Complication occurred in 1 (10%) of the patients as a representation of pneumothorax. No recurrence was noted during a median follow-up of 15 months.
Conclusion:
In this retrospective study, STER may be an effective and safe technique resecting large and irregular SMTs with a diameter no >40 mm in transverse diameter and no >100 mm in longitudinal diameter.
Introduction
W
Submucosal tunneling endoscopic resection (STER) has emerged as a feasible technique for resecting upper GI SMTs through natural orifice transluminal endoscopic surgery (NOTES). The submucosal tunneling technique was originally described by Sumiyama et al. 2 and later modified by Inoue et al. 3 as an endoscopic therapy for achalasia. Inspired by Inoue et al., 3 Xu et al. 4 developed a similar submucosal tunnel for endoscopic muscularis dissection to resect SMTs originating from the MP layer. Longitudinal submucosal tunneling technique may not only maintain mucosal integrity but also reduce the risk of postoperative perforation and abdominal infections, and promote rapid wound healing. 5 As a result of the complicated manipulating skills and possible adverse events, most studies are limited to small and regular SMTs with a diameter <35 mm.6,7 In this study conducted between April 2014 and April 2017, we retrospectively reported 10 cases using the new technique of STER to remove large and irregular SMTs originating from MP of upper GI tract in our hospital.
Patients and Methods
Patients
This retrospective study was approved by the ethics committee of the First Hospital of China Medical University. The inclusion criteria for enrollment were as follows: (a) presence of SMTs with large and irregular margins confirmed by computed tomography (CT) and endoscopic ultrasound (EUS), (b) normal epithelial covering the SMTs confirmed by narrow band imaging endoscopy, (c) no signs of metastasis invasion outside the GI tract, and (d) age between 20 and 70 years.
From April 2014 to April 2017, 10 consecutive patients with large and irregular SMTs underwent STER at our hospital. All patients were informed of possible adverse events related to STER procedure, such as pneumothorax, pneumoperitoneum, and subcutaneous emphysema. Written informed consent from all patients was obtained before the operation.
Definition
(a) Large and irregular SMTs were defined as those >35 mm in diameter with irregular or lobulated outer margin. (b) En bloc resection was defined as the intact fibrous capsule of the resected tumor, with vertical and lateral margins free of remnant tumors at endoscopy.
STER procedure
Before STER procedure, a thoracoabdominal CT is needed to identify the integral lesion property and surrounding anatomic structure. As presented in Figure 1, a lesion with dotted calcification is located in middle esophagus. The specific procedure and technical details of STER in case 4 are shown in Figure 2, described as follows: (1) diluted indigo carmine or methylene blue is injected into the submucosa to locate the SMT, (2) a fluid cushion is made using an injection needle 3–5 cm proximal to the oral side of the tumor, (3) at least 2 cm longitudinal or “T” shaped mucosal incision is made at the top of the fluid cushion using an electric knife as the tunnel entry point, (4) a submucosal longitudinal tunnel between the submucosal and muscularis layers is created with a hybrid electric knife. In addition, the tunnel end 3–5 cm distal to the SMT to ensure a satisfactory view of the SMT. (5) Expose the tumor, then carry out an en bloc resection along its margin without the interruption of its capsule with insulated-tip (IT) nano knife or IT 2 knife. (6) The mucosal incision was sealed by several clips after removing the tumor. All patients were operated on with conventional endoscopic accessories under propofol sedation. No sedation-related adverse events occurred during or after the procedure.
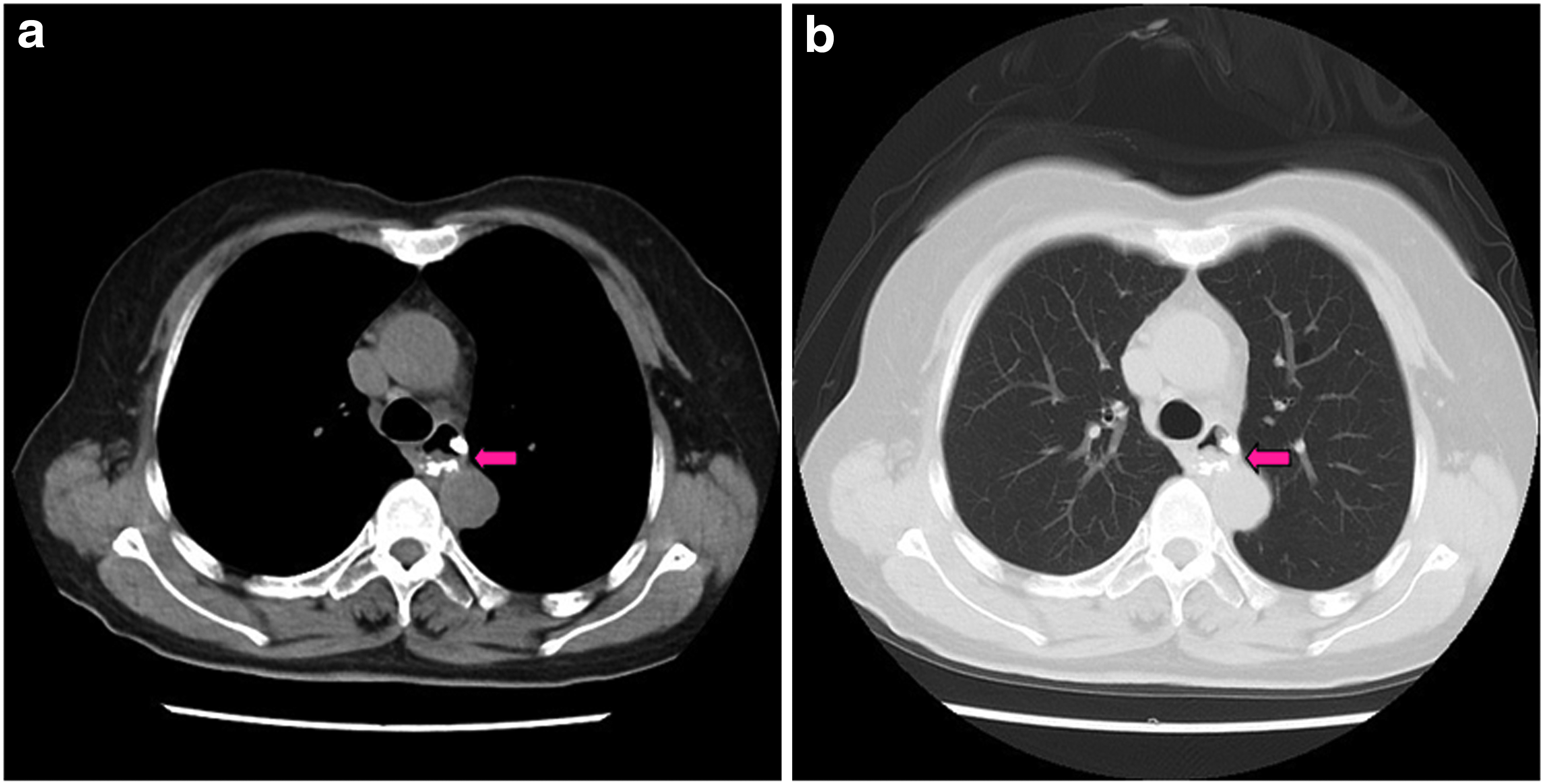
The presence of SMTs confirmed by CT. The arrows indicate the presence of SMTs confirmed by CT, with no signs of metastasis or invasion outside the gastrointestinal tract.

Specific procedure and technical details of submucosal tunneling endoscopic resection.
All the instruments were from Olympus; an endoscope (GIF-H260; Olympus, Tokyo, Japan) was used for all STER procedures. In addition, other auxiliary instruments were used for the specific procedure, included IT knife (IT2; Olympus and IT nano; Olympus), Hook knife (KD-620LR; Olympus), hemostatic forceps (FD-410 LR; Olympus), injection needle (NM-4L-1; Olympus), snare (SD-9L-1; Olympus), and carbon dioxide (CO2) insufflator (UCR; Olympus).
Postoperative management
Patients were kept in a fasting state for 48 hours, then on a liquid diet for 2 days; they were returned gradually to a normal diet within 1 week. A proton pump inhibitor (PPI) and antibiotics were used routinely for 3 days. On day 3 after the operation, thoracoabdominal CT was performed to check for the occurrence of gas or inflammation-related complications. Routine fecal examination was also performed to check for delayed bleeding.
Results
Clinical outcome
STER was successfully performed in 10 consecutive patients with 10 large and irregular SMTs with a diameter no <35 mm. In addition, there are two small SMTs with the diameter <35 mm simultaneously existing with large SMTs in cases 5 and 10, respectively. As presented in Table 1, 4 of the 10 patients (40%) were female and 6 (60%) were male. Median age was 47.5 years, ranging from 25 to 62 years. Among the patients, 40% (4/10) of the patients mainly complain about epigastric uncomfort. Other atypical symptoms include regurgitation, belching, dysphagia, and pharyngeal globus. The protrusion size was measured by EUS. There is no exact relationship between protrusion size and resected tumor size. What underlies a small protrusion may be a large SMT.
F, female; GERD, gastroesophageal reflux disease; M, male; NA, not applicable.
Therapeutic outcome
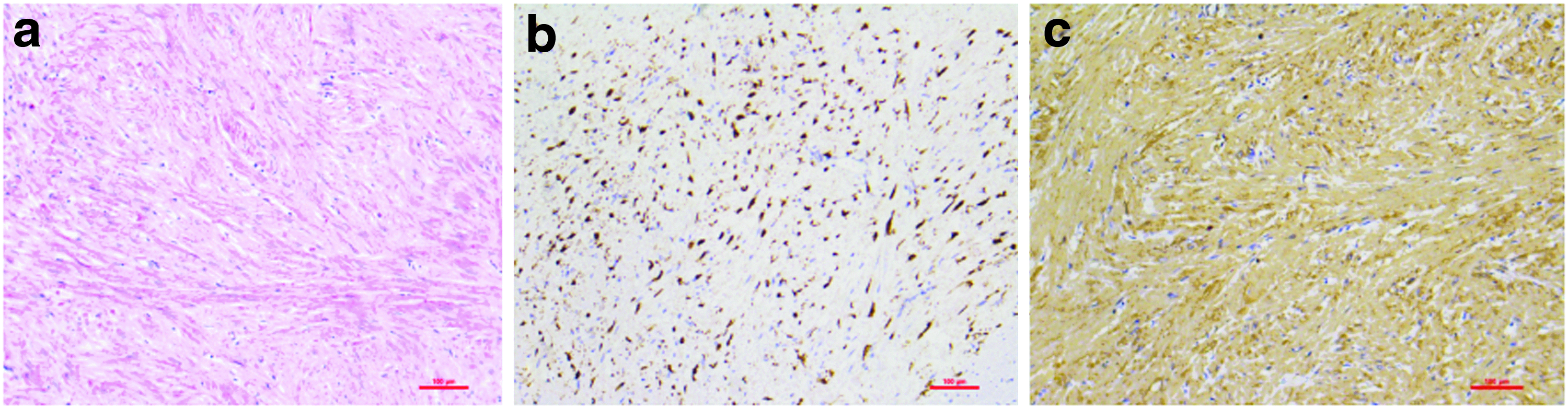
As presented in Table 2, of all the 10 large SMTs, 3 (30%) were located in esophagus and 7 (70%) were in cardia. The en bloc resection was achieved in 80% (8/10). Only two (20%) SMTs were resected into more than one piece, two pieces in case 10, and five pieces in case 2, as a result of comparatively narrow tunnel width. All resected lesions showed both lateral and vertical free of tumor margin through pathological evaluation. The average SMT size was 57.2 mm, ranging from 35 to 100 mm. Two to seven clips were used to seal the mucosal incision. Pathological and immunohistological assessment presented in Table 2 indicated that 8 of the 10 SMTs were GISTs, whereas 2 were leiomyomas. All the mitosis rate of the 10 specimens were <5%. Expression of p53 and c-kit was also presented in Table 2. Expression of ki64, CD117, and Dog-1 was assessed as auxiliary significance for diagnosis. Figure 3 shows the pathology and immunohistochemistry of the specimen in case 4. Complication occurred in only 1 (10%) of the patients as a representation of pneumothorax without serious pleural inflammation. No recurrence was noted during a median follow-up of 15 months. And other images of large and irregular SMTs removed by STER are presented in Figure 4.

Other large and irregular SMTs removed using the technique of submucosal tunneling endoscopic resection.
EUS, endoscopic ultrasound; GEJ, gastroesophageal junction; GIST, gastrointestinal stromal tumors; MP, muscularis propria.
Discussion
Certain SMTs have malignant potential, especially in GISTs. Large lobulated lesions with irregular outer margins are proved to harbor a higher risk for malignancy. When the tumor develops to malignancy or becomes large enough, patients may lose the opportunity to undergo minimally invasive treatment. As a result, resection of SMTs not only allows the histological diagnosis but also cuts off its potential malignancy.
Before NOTES came into practice, open or laparoscopic surgery was performed to remove SMTs, even without accurate orientation. In addition, open surgery results in large surgery trauma, delayed recovery, and a high rate of complications. The complications adversely affect the patient's quality of life postoperatively. Since NOTES became widely acceptable, ESD and EFR have been recommended to remove SMTs, with a high complete rate. 8 However, higher risk of severe complications such as perforation and secondary mediastinal infection limits their wide implementation. 9 In 2012, Xu et al. 4 first reported a new endoscopic technique called STER, which had high complete and en bloc resection rates. STER was then successfully implemented in different clinical centers, especially in China.
Compared with conventional ESD, EFR, and open surgery, STER has four advantages10,11: (1) it results in higher en bloc and complete resection rates and (2) it maintains the integrity of normal epithelial cells that cover the SMT. As a result, it reduces the risk of postoperative GI tract leakage as well as secondary infection, (3) The distance between the mucosal incision and the SMT is about 5 cm. As a result, the mucosal incision is regular and can be easily closed by hemostatic clips, and (4) the gastroscope enters the submucosal tunnel, obtaining different endoscopic views from every aspect.
However, considering the limited tunnel space and fragile esophageal adventitia, most researchers recommended a maximum resectable size of 35 mm. SMTs >35 mm were also reported to be successfully resected by STER. 12 However, reports of STER for large and irregular SMTs are limited to case reports.13,14 In this pilot study, we attempt to remove a series of large and irregular SMTs originating from MP with a diameter no <35 mm using the technique of STER. Among the SMTs, 80% (8/10) were en bloc resected without any interruption of the capsule. Only 20% (2/10) were resected into five pieces and two pieces in cases 2 and 10, respectively.
We tried our best to remove all the SMTs without interruption of capsule. However, we encountered different difficulties during the procedure of STER in cases 2 and 10, respectively. In case 2, due to the limitation of equipment and immature technique in 2014, we could not get a clear view while dissecting the deep side of fibrotic tissue. To facilitate the following complete resection, we had to perform a piecemeal dissection. In case 10, the maximum axis of the tumor is not parallel with longitudinal axis of esophagus with a relatively larger angle compared with other cases. We tried our best to adjust the axis of SMT for en bloc removal. However, we failed as a result of the narrow tunnel space. From this failure, we learned that a relatively wide tunnel space plays a critical role for en bloc removing of large SMTs.
To clarify, piecemeal dissection and related adverse prognosis were provided in the written informed consent provided to the patients and signed before surgery. Facing the difficulties, we inquired their family about the choice between piecemeal dissection and open surgery again. The two families chose to accept endoscopic piecemeal dissection, and refused to undergo open surgery.
Theoretically, it is clear that piecemeal dissection may lead to tumor cell seeding, which is not safe for prognosis. However, considering the following points, we determined to perform piecemeal dissection according to their family's desire. (1) After piecemeal dissection and removal of the pieces, we irrigated the tunnel cavity repeatedly. Short-time seeding will not form compact connection with surrounding tissue, and can be easily flushed by repeated irrigation. (2) Seeding metastasis mainly focused on malignant tumor cells. Comparing with malignant tumors, SMTs whether benign leiomyoma or GISTs, possess a relatively low productivity and invasiveness. (3) Recently published articles have reported the safety of SMT piecemeal resection. The article “Submucosal endoscopic tumor resection for epithelial tumors in the esophagus and cardia” by Inoue et al. 3 has reported 2 cases of piecemeal resection for large SMTs as early as 2011. (4) Patients suffer from related symptoms such as epigastric pain, dysphagia, and belching for a long time, which may be caused by the SMTs. Dissection of SMTs may help to alleviate their obstructive symptoms.
In our experience, the following ten opinions may be useful to facilitate an en bloc resection. (a) The mucosal incision should be extended according to the size of tumor. Sometimes a “T” shaped incision may facilitate retrieval of huge SMTs with both large transverse and longitudinal diameters, compared with longitudinal incision. (b) The width of the tunnel should exceed the transverse diameter of the tumor, which facilitates a satisfactory endoscopic view. (c) Compared with air, CO2 diffuses and be is absorbed at a higher rate. CO2 insufflation is recommended to extend the distance between mucosa and MP, facilitating following blunt dissection. (d) It is easy to lose the orientation to the tumor during tunnel construction. EUS is recommended to locate the tumor and adjust the orientation accurately. (e) The termination of tunnel should be 2 to 3 cm distal to the anal side of the tumor, which ensures a satisfactory view and ample operative space. (f) While dissecting the distorted part of the SMTs, we found that the fibrotic tissue connecting the SMT and MP layer was more compact and tight than other parts. This area is difficult to dissect and easy to disrupt the tumor capsule. Therefore, IT nano or IT 2 knife is recommended for its ceram hood, which is insulated and can protect the integrity of the tumor as shown in Supplementary Video S1. (g) While dissecting the adventitia side of the tumor, the dissecting direction by electric knife should be deviating from esophageal adventitia side in case of perforation as shown in Supplementary Video S2. (h) If there are vertical branches of penetrating vessels presented as in Figure 2f, the dissection at the base of the vessels should be done after precoagulation as shown in Supplementary Video S3. Maintenance of a clear field of vision plays a critical role by consistently treating the vessels not to bleed. (i) While having difficulty dissecting the fibrotic tissue between the normal mucosa and lesion, reiteration of methylene blue injection may help to separate the lesion and surrounding tissue as shown in Supplementary Video S3. This may facilitate the following dissection and reduce the damage to normal mucosa. (j) While removing the SMT, the maximum axis of the tumor is recommended to be parallel to the longitudinal axis of the esophagus. Let the minimum diameter of the SMT pass through the longitudinal incision or “T” shaped incision.
Similar with the study by Chen et al., 11 transverse diameter plays a critical risk factor for piecemeal resection and adverse events compared with transverse diameter. In their study, of the 11 SMTs with the transverse diameter >35 mm, 6 (54.5%) were piecemeal resection. In our study, according to the technical skills mentioned previously, the piecemeal resection rate was as low as only 20%, which continues to be decreasing.
All of patients, regardless of whether they displayed complications, should receive intravenous antibiotics and PPIs. Complication occurred in case 10 as a representation of pneumothorax. The patient recovered after 3 days of conservative treatment without closed thoracic drainage. All of the patients received a chest CT scan to check for the presence of air leakage. For the patients who received piecemeal resection, EUS examination was essential, every 6 months for the first 2 years, and once a year afterward.
This study has several notable limitations. (1) The study includes only a small series of cases, lacking of high reliability. (2) The study belongs to retrospective design, not perspective. (3) A relatively short-term follow-up cannot strongly prove the efficacy for large and irregular SMTs. Therefore, a perspective study including a large series of cases is needed to clarify the efficacy and safety of the new technique for large and irregular SMTs originating from MP.
Conclusion
In conclusion, this study has shown that STER may be an effective and safe technique for resecting large and irregular SMTs with a diameter no <35 mm from upper GI tract. Based on our experiences, SMTs with no >40 mm in transverse diameter and no >100 mm in longitudinal diameter could be removed by STER. Complete and en bloc resection plays critical roles for prognosis.
Footnotes
Acknowledgment
This research received the support granted by Natural Science Funding of Liaoning Province (Grant No. 2013021043).
Authors' Contributions
M.S. and X.W. designed the study. M.S. performed all the operations using the new technique. S.S., M.F., H.Z., and M.L. organized the project and wrote the article.
Ethical Approval
All the pathological assessments were necessary examination items in patients' treatment, which are not particular to, or for, this research or related to ethical issues. Informed consents were signed by all the patients.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.