
Abstract
Abstract
Objectives:
The aim of this meta-analysis was to examine postoperative pain and surgical outcomes (operative time, hospital stay, the incidence of seroma and recurrence) with different mesh fixation methods following laparoscopic ventral hernia repair (LVHR).
Methods:
Randomized clinical trials compared different methods of mesh fixation in LVHR and reported on pain outcome measures analyzed. The results were expressed as odds ratio (OR) for combined dichotomous and mean difference (MD) for continuous data.
Results:
Five randomized controlled trials (RCTs) with a total of 466 patients comparing tack mesh fixation to suture mesh fixation technique in LVHR were identified, all were published after 2005. A meta-analysis gave statistically similar odds of postoperative chronic pain (OR, 1.24; 95% CI, 0.65–2.38; z = 0.65; P = .51). No difference in pain intensity (PI) scores was found at 4–6 weeks (MD, 0.18;% CI, −0.48 to 0.85; z = 0.54; P = .59) and at 3–6 months postoperatively (MD, 0.10; 95% CI, −0.21 to 0.42; z = 0.64; P = .52). There was no difference in the pooled analysis of seroma/hematoma formation (OR, 0.60; 95% CI, 0.29–1.26; z = 1.35; P = .18), recurrence (OR, 1.11; 95% CI, 0.34–3.62; z = 0.18; P = .86), and hospital stay (MD, −0.06; 95% CI, −0.19 to 0.08; z = 0.83; P = .40). Operative time was significantly lower with tack fixation (MD, −19.25; 95% CI, −27.98 to −10.51; z = 4.32; P < .05).
Conclusions:
Meta-analysis of RCTs comparing tacks to suture fixation in LVHR showed comparable results with regard to postoperative chronic pain incidence and PI, and hernia recurrence. However, the operative time is shorter with tacks compared to suture fixation technique.
Introduction
L
It is widely accepted that the method of mesh fixation plays a major role in the development of postoperative pain.9–12 Mechanical mesh fixation with helical tacks may cause irritation to the peritoneum and muscle injury; on the other hand, transfascial suture fixation may lead to tissue ischemia and nerve entrapment.8,9,13 Based on this assumption, noninvasive fixation techniques have been recently introduced to practice for different types of hernias, like using fibrin glue.14–16 For the above-mentioned reasons, interventions that focused on optimizing preventive and therapeutic strategies for post-LVHR pain have become the foundations of efforts of many authors, yielding a number of publications over the recent years. However, the lack of uniformity in outcome reporting and the methods used to assess early postoperative and chronic pain among the available published studies have resulted in significant heterogeneity. Unfortunately, such heterogeneous data may be insufficient to establish evidence-based recommendations of which technique is superior in terms of pain outcomes and what are the recommended pain management modules.
As a solution to improve outcome reporting, the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) group 17 and the International Association for Study of Pain (IASP) 18 have proposed core outcome domains and definitions to be adopted in study designs investigating chronic postoperative pain, which include the following: Pain Intensity (PI) using validated scoring system, effect of pain on physical and emotional functioning, and participant rating of global satisfaction.
The main objective of this review is to examine the level of early and chronic postoperative pain in relation to the methods of mesh fixation for patients subjected to LVHR. Furthermore, it is to identify if the recommendations made by IMMPACT group and IASP (2005) have been adopted to improve reporting on post-LVHR pain outcome.
Methods
The literature search was performed using the database from MEDLINE (through PubMed), Embase, and Cochrane Central Register for clinical trials (through cochrane.org). The Cochrane highly sensitive search strategy was applied to identify the relevant articles. 19 The following medical subject heading (MeSH) terms were used in combination using the Boolean operators (AND) and (OR), and with free text: “hernia, ventral,” “incisional hernia,” “hernia, umbilical,” “Hernia, abdominal,” “laparoscopy,” “minimally invasive,” and “Fibrin glue.” Also, equivalent free-text term such as “Ventral hernia,” “Incisional hernia,” “Umbilical hernia,” “epigastric hernia,” and “laparoscopic ventral and incisional hernia repair” were used in combination with “tacks mesh fixation,” “suture mesh fixation,” “stapled mesh fixation,” “mechanical mesh fixation,” “non-mechanical mesh fixation,” and “fibrin glue mesh fixation.” The highly sensitive search strategy details can be found in Table 1. In addition to that, reference lists of the reviewed articles were manually selected to identify the relevant articles not identified in the electronic search. The last search was run on April 20, 2017.
Review process and study selection
All searched titles were reviewed; the selected abstracts were assessed based on predefined eligibility criteria, consulting the full text in the case of doubt to assess whether it meets these criteria. All selected studies were individually analyzed by two independent reviewers to determine eligibility for systematic review and meta-analysis. Randomized controlled trials (RCTs; irrespective of the language, blinding, country of origin, and sample size) that reported on mesh fixation were included in this review. Pain should be either primary or secondary outcome to be entered into the analysis. Trials comparing laparoscopic versus open repair and experimental studies on animal were excluded. With regard to pain and Quality of Life (QoL) assessment reporting tools and pain intervention models, no restrictions were applied. To warrant homogeneity namely “patient” and intervention,” optimum comparability between the hernia type and method of mesh fixation was aimed for. The fixation methods assessed in each of the included RCTs are shown in Tables 2 and 3.
Patients' age, 18 years and older.
Value in mean, unless otherwise indicated.
Median (range).
DC, double crown; FU, follow-up; QoL, quality of life.
PCA, patient-controlled analgesia.
Data extraction
The extracted data from each trial included the following: (1) article-specific data: primary author's name, year and name of journal, study country, and name of institution/s; (2) characteristics of trial participants: number of study patients, age, gender, type of hernia, and mean defect size; (3) intervention: type of surgery and mesh, method of fixation and the control group, number and type of tacks used (absorbable or nonabsorbable), and number and type of sutures used for mesh fixation; (4) outcome data and type of outcome measures (validated scales): visual analogue score (VAS 0–10 cm or 0–100 mm), basal preoperative score, time interval after surgery and at discharge, long-term VAS (3 months and after), duration of follow-up (FU) as decided by trial methodology, number of patients who have completed FU, “long-term VAS” and “chronic postoperative pain,” QoL measures, and time interval recorded and duration of FU, mean recurrence rate, measures used for recurrence diagnosis, and duration of FU. To assess the validity of eligible trail according to Cochrane Collaboration, two authors independently determined the adequacy of randomization and allocation concealment, blinding of participants and outcome assessors, incomplete and selective reporting, and the extent of loss to FU. Lack of reporting on outcome was not considered a lack of event. In the case of missing or unclear data, a copy of the review draft was e-mailed to the corresponding author asking for further information; two authors were contacted and both of them have e-mailed us back with most of the information that we required.
Outcomes of interest
The primary outcomes for this analysis were post-LVHR early and chronic pain in relation to fixation technique.
The secondary outcomes include the following:
A. Surgical outcomes include operative time, hospital stay, recurrence and complications (seroma and hematoma), and costs. B. To assess if IMMPACT and IASP group recommendations (2005) were adopted in the methodology of the included trials, by looking to the presence of chronic pain definition, the presence of validated assessment tool for PI and effect on QoL, sufficient FU of at least 6 months, and the presence of baseline pain score.
Statistical analysis
The statistical methods Mantel-Haenszel (M-H) and Inverse Variance (IV) were undertaken with the RevMan software package (Review manager 5.3, The Nordic Cochrane Centre, Copenhagen, Denmark). Pooled odds ratio (OR) with 95% confidence interval (CI) was used to measure the effect of each intervention on dichotomous data. Mean difference (MD) with 95% CI was calculated to assess the size and the effect of each intervention on continuous data. The fixed-effect model was used first to analyze the data and was applied if no heterogeneity was found. However, in the case of the presence of significant heterogeneity among the analyzed trials, a random-effect model was used and reported. 20 Heterogeneity was explored using χ2 test, with a significant value set at P < .05, and was quantified using the I2 test. If the outcome value was reported in median and range, means and standard deviations were calculated based on Cochrane collaboration. Pain scores reported with VAS 0–100 mm were divided by 10 to be entered in the analysis model.
Sensitivity analysis
Sensitivity analysis of the OR was planned for the analysis models with three or more studies reported on same outcomes, in which, no event occurred in one of the intervention groups by using the method recommended by Deeks et al. 21 This included the rates of chronic pain and recurrence outcomes of reports compared tack mesh fixation (TMF) and suture mesh fixation (SMF). A separate sensitivity analysis, based on Cochrane Collaboration recommendations, 20 was done for chronic PI outcome (3 and 6 months) by undertaking the meta-analysis twice: first, including all studies in the model to measure the effect. Second, including only studies reported on mean pain scores at 3 months, while studies that only reported on mean pain scores at 6 months were omitted from the model to assess if variability of chronic pain assessment time affects the pooled outcome.
Result
Study selection
Out of 896 studies identified in the electronic and manual search, eighteen trials were selected for a full article review after the first-level screening. Following full-text review, nine trials were found to fulfill the inclusion criteria.22–30 Only five trials that compared suture to the tack fixation technique were considered for meta-analysis.22–26 Four trials were excluded to limit the interventional heterogeneity; two trials compared absorbable to nonabsorbable tack fixation,27,28 one compared two concepts of mesh/fixation systems (elastic vs. rigid), but the fixation technique used in this study was absorbable tacks in both limbs, 29 and the other compared tacks to glue fixation. 30 The selection process is summarized in Figure 1.
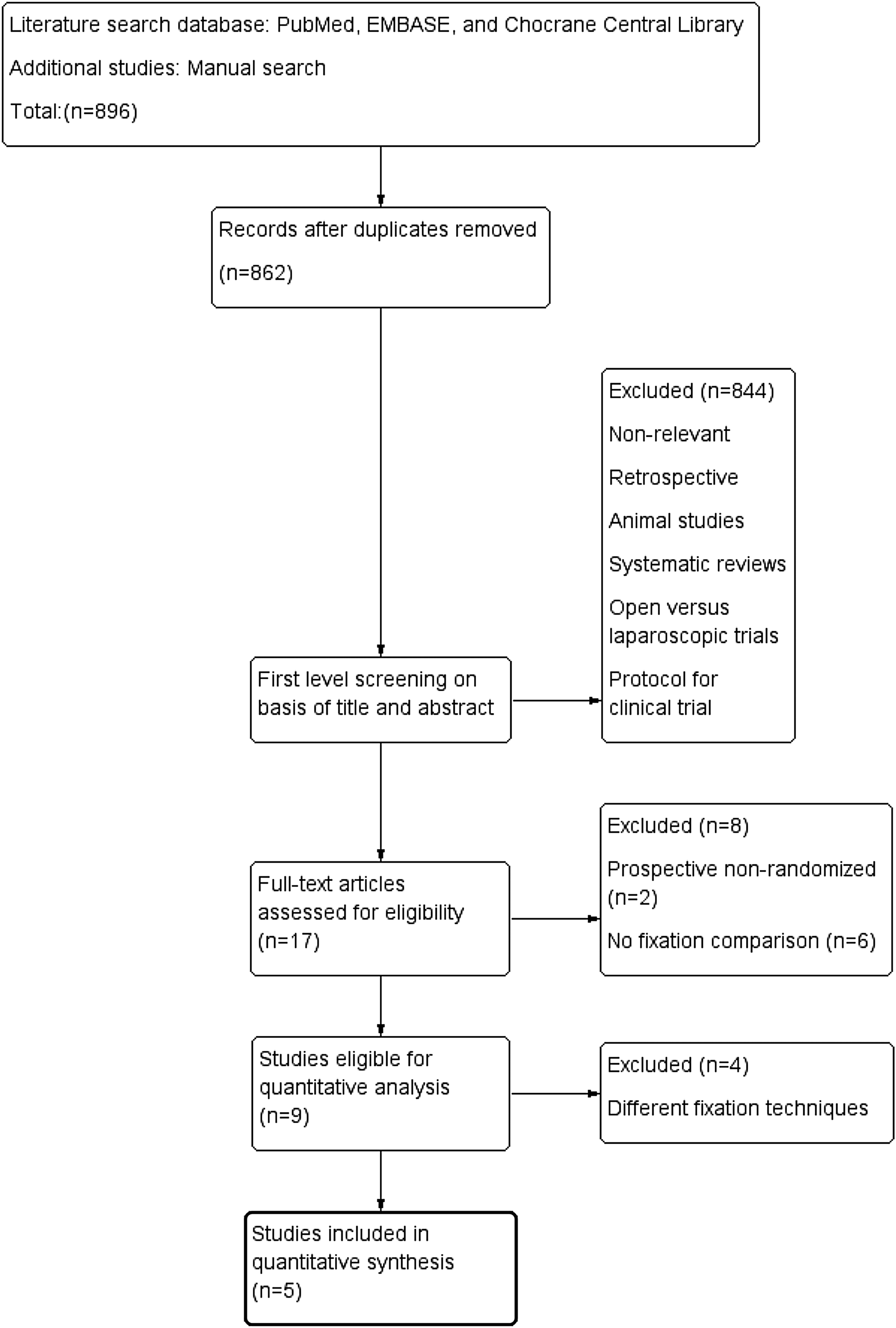
PRISMA flow diagram showing study methodology.
Study characteristics
The included five trials were all published in the English language between 2009 and 2016; reports were originated from India, Netherlands, United States, and Switzerland.22–26 The cumulative study population comprised 466 patients subjected to laparoscopic ventral hernia mesh repair between 2004 and 2014. All trials utilized the criteria of “ventral hernias morphological classification” in their reports 31 ; these criteria include the following: (1) recurrence rating (primary ventral or incisional); (2) morphology (location); (3) size of the hernia gap; and (4) risk factors. Mean percentage of incisional hernia was 63% and primary ventral hernia was 37% from four trials.22,23,25,26 Mean hernia defect size was 19.3. No statistical difference was reported between the study groups within the included trials with respect to hernia etiology, hernia gap, and location. Moreover, apart from size, there was limited variation with regard to inclusion and exclusion criteria among the included RCTs. Exclusions were mainly for cases with previous mesh repair and hernias close to bony prominences. Median FU ranged between 3 and 32 months.
Fixation technique
In tack fixation arm, all trials used nonabsorbable tacks of the same type; double-crown tack technique was adopted in all trials except in the study of Beldi et al., 25 where single-crown technique was used. In suture fixation arm, nonabsorbable sutures were used in all five trials, transfascial sutures were placed 1–2 cm apart22,25,26 or placed 4–5 cm apart23,24 (Table 3).
Quality assessment
Quality assessment of the included trials was carried out based on the Cochrane collaboration's tool (adopted from Higgins and Altman). 20 All five studies specified the randomization process. One trial had patient and assessor blinded, 26 and one trial had patients blinded only. 25 Two trials were considered to have a high or unclear risk of reporting bias, because they did not provide data on outcomes considered of principle importance, such as early or long-term pain score, QoL, and baseline pain score.23,25 Four studies were considered to be of unclear or high risk of bias due to one or more reasons like lack of power calculation, small study group, short length of FU, significant imbalance in age, early stopping of recruitment, and small defect size that cannot be generalized.22,23,25,26 Quality assessment is summarized in Figure 2a and b.

Data Analysis
Primary outcomes
Pain incidence and severity
As shown in Table 4, post-LVHR PI peaks at day 0, particularly during the first 6 hours, with mean value range between 4.2 and 6.8 cm, VAS (0–10). Generally, the PI trend decreases with time; however, it differs between the analyzed studies. Pain scores during the first 24 hours and 1–2 weeks post-LVHR were reported in three trials.22,24,26 They all showed reduction in PI scores at 1–2 weeks; however, the statistical difference between the comparison groups within each trial was not changed compared to the early postoperative period. All five studies reported on chronic PI score. There were few differences in the time at which chronic pain was measured between the trials; pain was reported at 3 months in four trials22–24,26 and at 6 months in only one trial. 25 Wassenaar et al. 24 looked at pain outcome with three types of fixation techniques (absorbable suture, tacks, and nonabsorbable suture) at three postoperative time points; only two study groups were included in the meta-analysis (tacks and nonabsorbable suture) to ensure methodological homogeneity.
Data are presented as mean ± standard deviation (range).
% of patients with VAS>1 cm.
% of patients with VAS>2 cm.
NAS, nonabsorbable suture; AS, absorbable suture; R, rest; C, coughing; IQR, interquartile range; NA, not applicable; VAS, visual analog score.
The early postoperative pain was measured at various time points (within the first 24 hours) using VAS; two trials showed significantly lower mean VAS with SMF at 1, 6, and 24 hours.22,26 Muysoms et al., 23 however, reported significantly higher mean VAS with SMF during rest and coughing at 4 hours postoperatively compared with the SMF group (P = .028 and .013, respectively). Due to the variation in their reported time points and the status at which the pain is reported (during rest and with coughing) (Tables 4 and 5), and the variation in perioperative pain management protocols, it was not possible to get an accurate comparative analysis for this endpoint.
Value reported in mean ± SD unless otherwise indicated, P = P-value.
VAS mean during coughing at 4 hours postoperatively.
Mean ± SD was calculated from median and range based on Cochrane principles.
Examining pain at the period between 4 and 6 weeks post-LVHR, there was no statistical difference in VAS means with the use of TMF and SMF in the random-effects model (MD, 0.18; 95% CI, −0.48 to 0.85; z = 0.54; P = .59; Fig. 3). There was significant heterogeneity among trials (χ2 = 40.04, df = 4, P < .00001; I2 = 90%).
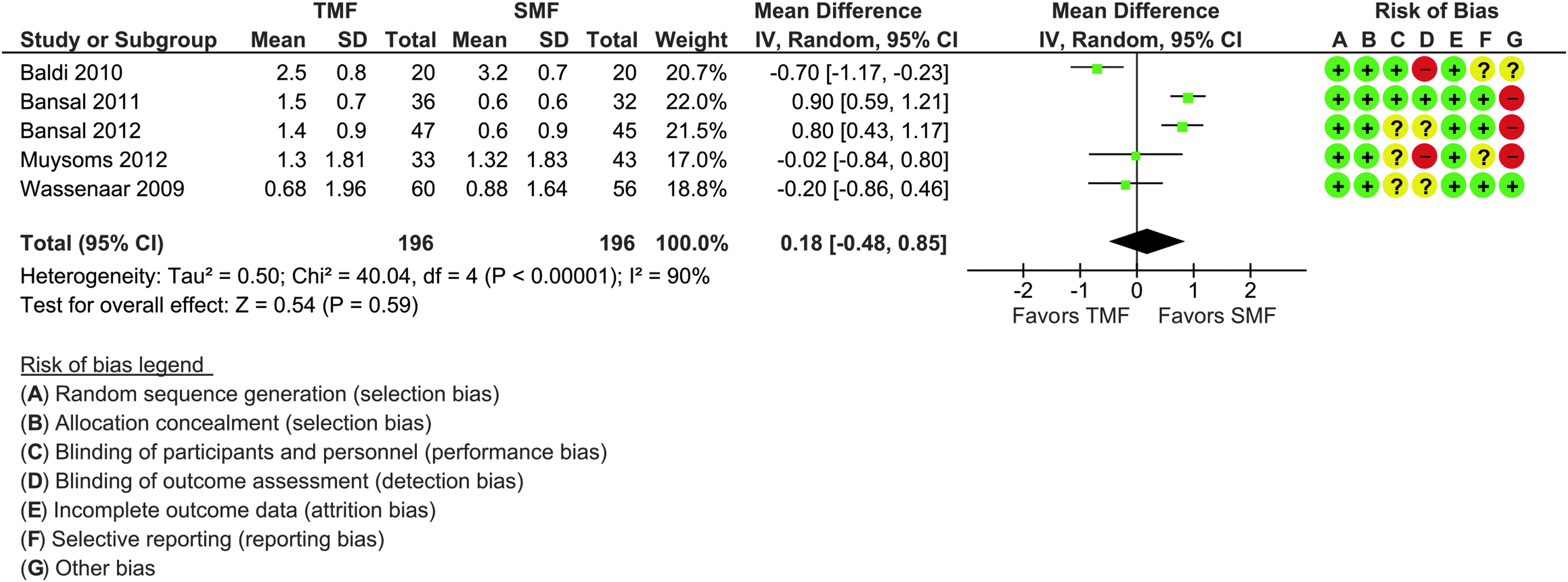
Forest plot of the difference in mean of pain scores (VAS) 4–6 weeks postoperatively between TMF and SMF in LVHR. SMF, suture mesh fixation; TMF, tack mesh fixation; VAS, visual analogue score.
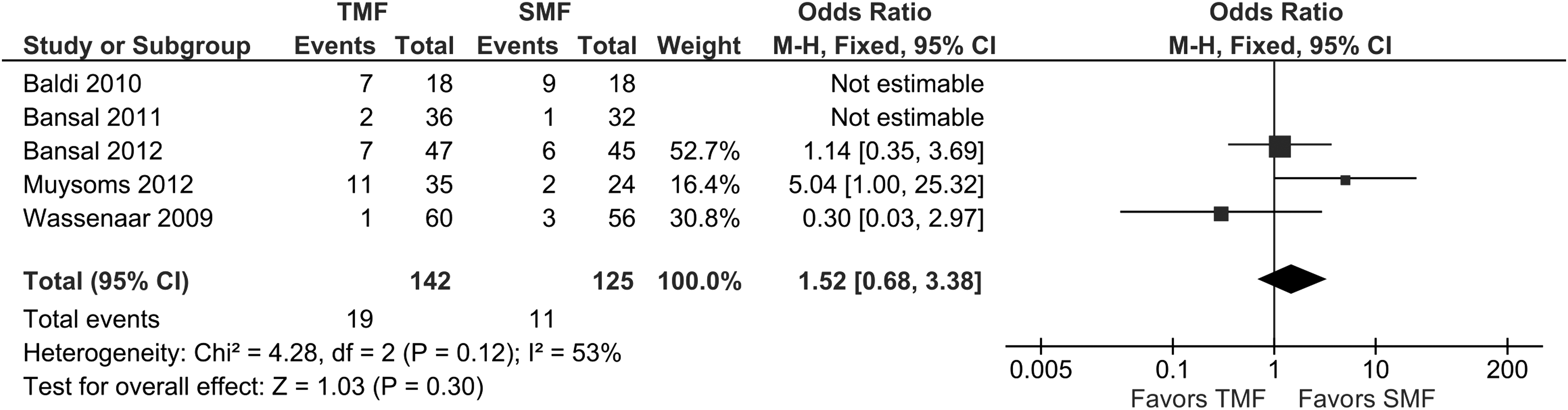
Chronic pain (>3 m) was reported in 13% and 10.8% of patients subjected to repair with tack and suture fixation, respectively. There was no statistical difference in the incidence of chronic pain occurrence between TMF and SMF in LVHR in the fixed-effect model (OR, 1.24; 95% CI, 0.65–2.38; z = 0.65; P = .51; Fig. 4). There was no significant heterogeneity (χ2 = 5.47, df = 4, P = .24, I2 = 27%) among the analyzed data. This effect was also evident in the sensitivity analysis by including only the studies that reported on the chronic pain rate at 3 months (Fig. 5).

Forest plot suggests no difference in odds of chronic pain with the use of TMF and SMF in LVHR. LVHR, laparoscopic ventral hernia repair.
Forest plot suggests no difference in the odds of chronic pain with the use of TMF and SMF with sensitivity analysis by including only studies reported at 3 months post-LVHR.
PI 3–6 months after LVHR was similar between SMF and TMF in the random-effect model (MD, 0.10; 95% CI, −0.21 to 0.42; z = 0.64; P = .52; Fig. 6). There was significant heterogeneity (χ2 = 17.25, df = 4, P = .002, I2 = 77%) among the analyzed data. A separate sensitivity analysis was done by omitting one trial reported on chronic pain at 6 months from the model; nevertheless, this effect was still statistically similar (Fig. 7).
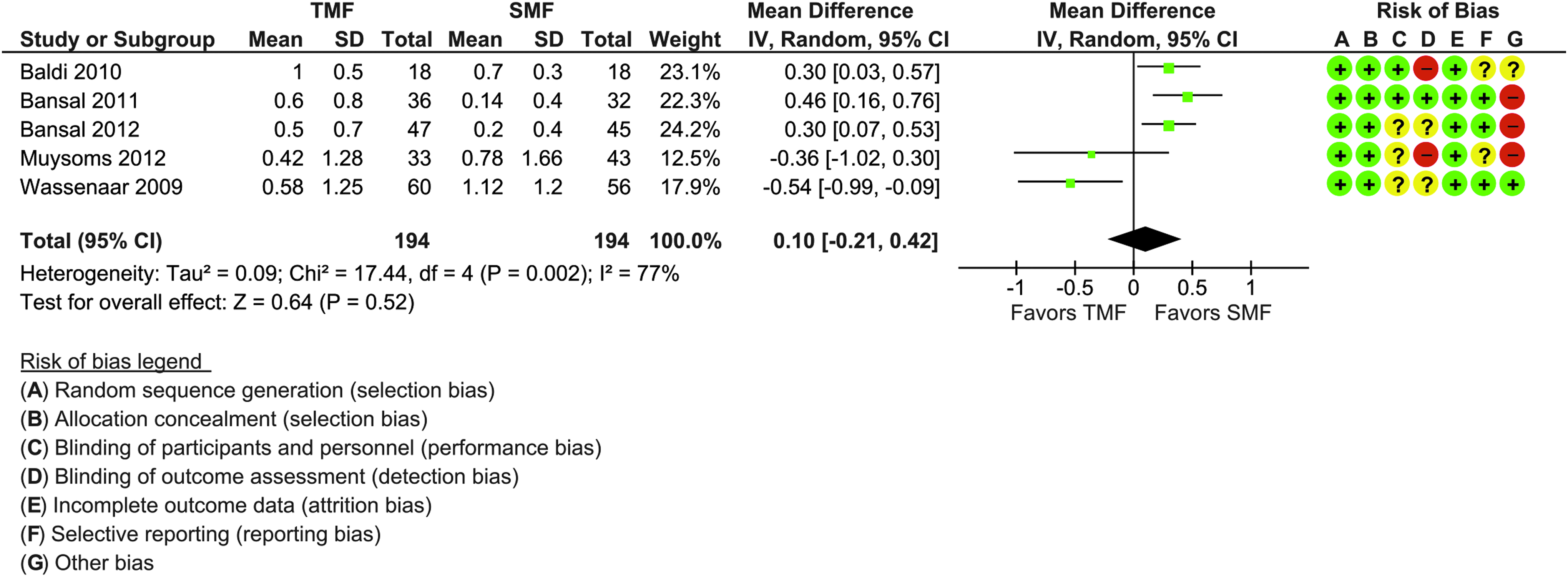
Forest plot of the difference in mean for chronic pain (3–6 month) after surgery with TMF and SMF in LVHR.

Forest plot suggests no difference in mean for chronic pain score (3–6 month) after surgery with TMF and SMF in LVHR with sensitivity analysis by including only studies reported at 3 months.
Secondary outcomes
Operative time
TMF has significantly lower operative time means compared with SMF in LVHR in the random-effect model (MD, −19.25; 95% CI, −27.98 to −10.51; z = 4.32; P < .0001; Fig. 8). This trend was depicted with all the five analyzed trials. There was significant heterogeneity (χ2 = 13.79, df = 4, P = .008, I2 = 71%) among the analyzed data.
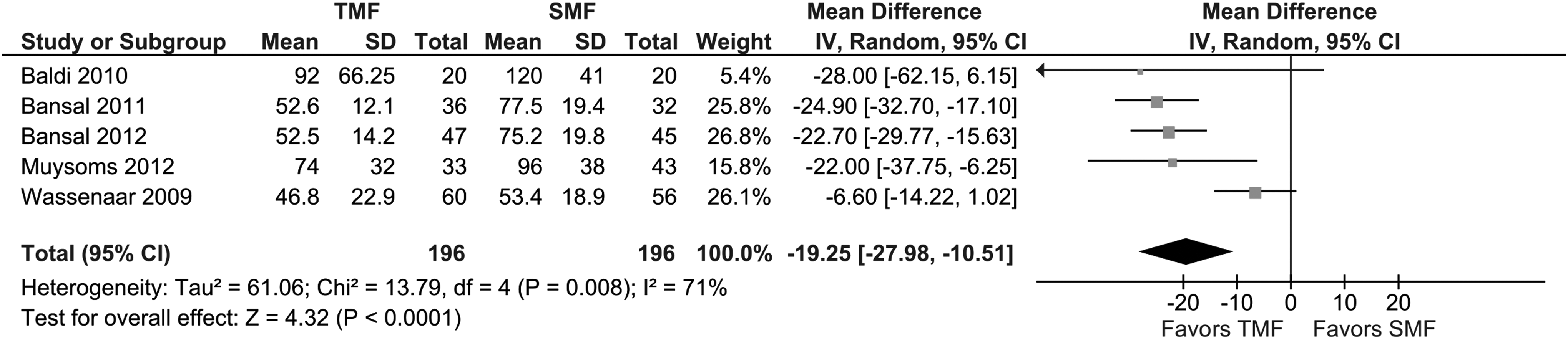
Forest plot of the difference in mean for the duration of surgery in minutes suggests TMF takes less time compared to SMF.
Length of hospital stay
The length of hospital stay was statistically similar in both TMF and SMF after LVHR. There was no heterogeneity (χ2 = 2.22, df = 4, P = .70, I2 = 0%) among the analyzed data in the fixed-effect model (MD, −0.06; 95% CI, −0.19 to 0.08; z = 0.83; P = .40; Fig. 9).
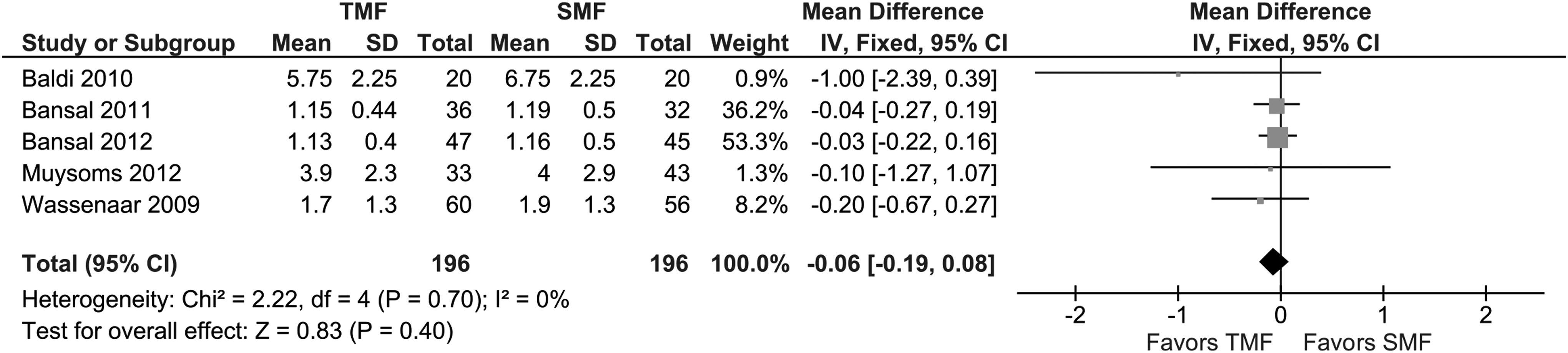
Forest plot for length of hospital stay after the use of TMF and SMF in LVHR.
Recurrence
There was no statistical difference in the odds of recurrence occurrence between TMF and SMF after LVHR. There was no heterogeneity (χ2 = 2.51, df = 3, P = .47, I2 = 0%; Fig. 10) in the fixed-effect model (−OR, 1.11; 95% CI, 0.34–3.62; z = 0.18; P = .86).
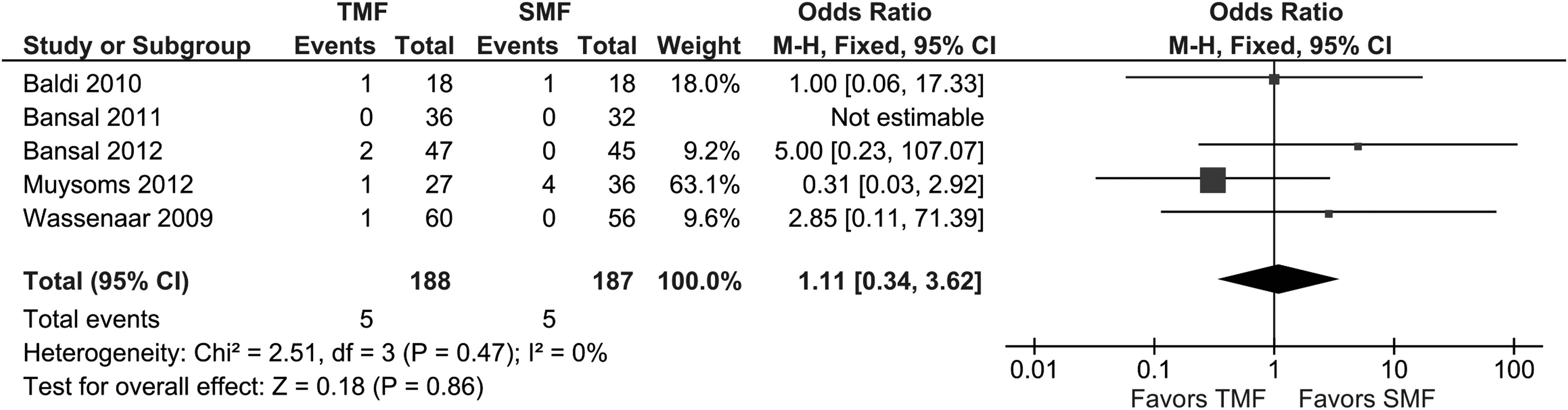
Forest plot of the odds for recurrence between TMF and SMF after LVHR.
Seroma and hematoma
Among four trials reported on seroma and hematoma occurrence,22–24,26 TMF and SMF were statistically similar (OR, 0.60; 95% CI, 0.29–1.26; z = 1.35; P = .18), There was no heterogeneity (χ2 = 2.62, df = 3, P = .45, I2 = 0%; Fig. 11).
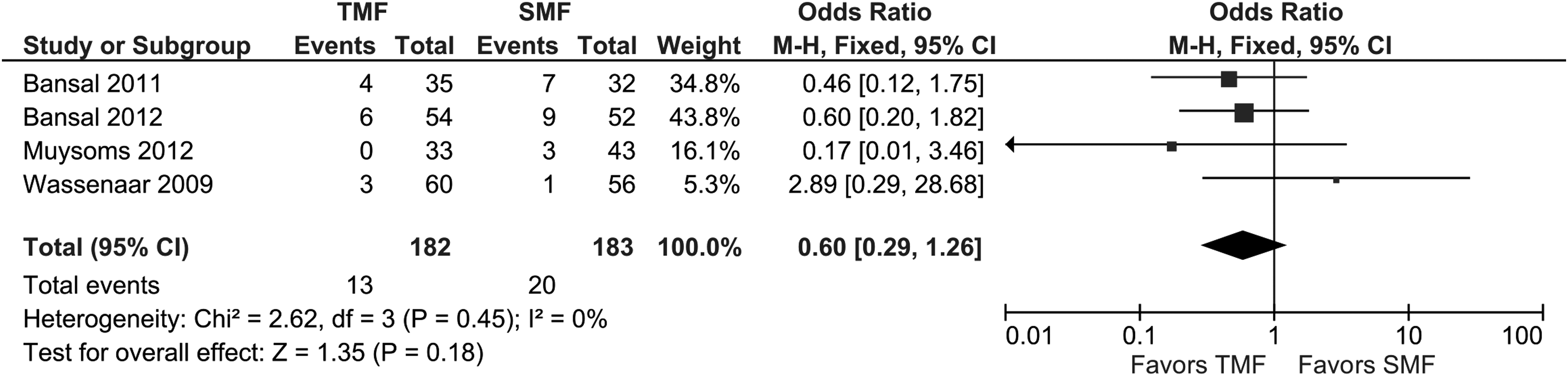
Forest plot suggests no statistical difference in (seroma and hematoma) formation between TMF and SMF in LVHR.
Cost
Only two trials reported on the cost difference,22,26 both studies showed a higher overall cost with tack fixation compared to suture fixation; however, this outcome could not be pooled due to inadequate data, “the standard deviations of the cost variable were not reported in one of the trials.” 26
Quality of trials based on pain outcome reporting
Quality assessment was applied to all included five trials No study adopted the all 4-point domain criteria recommended by IMMPACT. Two trials fulfill three points,22,24 and the other three reports reported on two points.23,25,26 Baseline scores were reported in two trials only.24,27 All trials were published after 2005, with only one trial that started recruiting before 2005. 23 For this reason, the comparison between the two periods was not possible. Table 6
Values in median.
+, Meets the criteria.
−, Does not meet the criteria.
Definition of chronic pain
Two of the included trials applied the agreed definition of chronic postsurgical pain (CPSP) by IASP group, “pain that persists 3 months postoperatively.”22,23 No clear definition was reported by the other three trials.24–26 Some studies included a quantitative assessment like PI in their definitions of chronic pain, which was either descriptive term, 24 VAS or QoL.23,24 In addition, some studies incorporated a minimal PI score to distinguish between clinically relevant or minor chronic PI (Table 7).
VAS, visual analogue score; VRS, verbal rate response; QoL, quality of life.
PI and QoL
PI was mentioned by all included trials; however, only two studies have reported on QoL in conjunction with PI.22,24 All studies used VAS to report on PI. Two reports included pain severity with the duration to define chronic pain.23,25 QoL was assessed using SF-3622,24; the verbal rating scale (VRS) was used by one trial to report on overall satisfaction. 22
Duration of FU of at least 6 months
Median FU ranged from 3 and 32 months. Out of the five trials, four studies have an FU ≥6 months.22,23,25,26
Discussion
This review has systematically analyzed outcomes reporting from a number of recently published RCT concerning LVHR surgery. Nine RCTs that compared different methods of mesh fixation reporting on postoperative pain were identified. Out of them, five RCTs comparing TMF to SMF were included in this meta-analysis. Four trials were excluded from the analysis because their intervention groups were different; two trials compared absorbable to nonabsorbable tacks,27,28 one trial used absorbable types of tacks in both study groups, 29 and one trial compared fibrin glue to tacks. 30 The results of our analysis indicate that the included studies have uniformly reported on many variables, which we quantitatively analyzed; nevertheless, we found an absence of standardized definitions and variability in assessment times of postoperative pain outcome. These might have led to underreporting of chronic pain incidence, which is basically important for the practicing surgeon comparing outcomes from different trials.
Concerning the early postoperative pain, only three trials reported on this endpoint. Favorable results for SMF fixation were demonstrated by two reports; they provided pain scores at distinct time points during the first 24 hours after surgery,22,26 whereas, Muysoms et al. 23 reported higher mean VAS with SMF at one time point (4 hours postoperatively) (Table 3). However, this review does not provide a comparative analysis for this point. Due to the variation in the reported time points and status at which pain was assessed (during rest or coughing), relevant data could not enter the synthesis model.
This quantitative analysis shows that TMF and SMF techniques were equal in terms of intermediate and chronic PI, as well as chronic pain incidence. For Wassenaar et al.'s 24 study, we have included only limbs that compare nonabsorbable SMF to TMF in the analysis model. Excluding the absorbable SMF (AS) group from the analysis was justified; this is basically to make the comparison homogenous based on the finding that only nonabsorbable sutures were used in the SMF group in all other included trials.
Pain measurement scale was the same among these studies; nevertheless, there was diversity in the time points as well as the status of pain outcome reporting during the early postoperative period. For this reason, acute pain outcome data were not comparable. Looking at the inclusion criteria within each trial, namely “patients,” it is noticeable that all trials considered the criteria of ventral hernia classification in reporting hernia characteristics 31 : etiology (ventral or incisional), morphology (location), size of the hernial gap, and risk factors. No statistical differences were reported between the study groups within each included trial. This even distribution among study groups coupled with the uniformity of repair approach among the included trials basically limits clinical heterogeneity and warrants this quantitative analysis.
During recent years, guidelines advocate mesh repair for ventral hernias, even with defects less than 2 cm in diameter, and preferably by LVHR. 32 However, there is still no agreement about the best fixation technique because of lack of supporting evidence. In fact, this keeps the door open for surgeons to adopt various techniques aiming to achieve best outcomes. Surgeons tend to place at least four corner transfascial suture or 4–5 cm apart in conjunction with tack fixation.22–24,26 Furthermore, whenever tacks-only fixation was used in the included trials, the double-crown technique was adopted.22–24,26 The purpose behind these techniques basically is to decrease the risk of recurrence due to mesh migration and shrinkage. However, in the study of Beldi et al., 25 because the primary objective was to test mesh shrinkage with tack- versus suture-only technique, the four corners anchoring transfascial sutures, which were used to orient the mesh before firing the titanium tacks, were all removed at the end of the procedure, and a single-crown tack technique was described in the tack fixation limb. Although they found a significant shrinkage in horizontal mesh size in the tack group, there was no clinical effect on mesh displacement at 6 months. The pooled outcome of this meta-analysis is based solely on the available five RCTs that compared tacks and SMF in patients undergoing LVHR. These trials were of moderate to high methodological quality. However, the presence of some heterogeneity between trials and the shorter duration of FU (3–6 months) in two trials24,25 make it underpowered, in particular, the recurrence rate; therefore, the conclusion of this review might still be used with caution.
Latest guidelines of the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) on LVHR recommended that fixation type, the number of tacks or sutures, and the amount of fixation material (like fibrin glue) should be appropriate for the size, shape, and location of the hernia defect. Increased fixation strength is required as the defect becomes larger and the prosthetic/defect ratio decreases. 33 Larger hernia defect requires a larger mesh, which basically needs more fixations and that might obviously reflect in the postoperative pain and complications.23,34,35 However, Wassenaar et al. 24 stated that post- LVHR PI is not due to the cumulative effect of many fixation points; this was basically based on the findings of no correlation between the number of tacks used and postoperative pain severity. This hypothesis can also be supported by the findings of Schoenmaeckers et al. 36 ; they demonstrated that using fewer tacks does not reduce PI and more tacks does not mean higher pain severity after LVHR.
The pain outcome estimates of this analysis did not concur with the meta-analysis published to date, 37 which included two RCTs and two observational studies comparing TMF to SMF in LVHR. The pain outcome reported only at 4–6 weeks postoperatively and was significantly lower with TMF. The difference in postoperative pooled pain outcome at 4–6 weeks between the published meta-analysis and the current one could be explained by the fact that the former was based on two RCTs, and the mean and standard deviation of pain scores from one trial used 26 were indirectly calculated from the median (range) according to Cochrane guidelines, whereas this meta-analysis was based on five RCTs, and the data used in our model were different; the missing data from the study of Bansal et al. 26 were obtained directly from the primary authors by e-mail Figure 3. This analysis showed that both fixation techniques were comparable in efficacy with regard to recurrence rate. This was also evident in International EndoHernia Society (IEHS) guidelines, 32 and in an earlier study by Kitamura et al. 38 A low recurrence rate (4.4% and 4.5%) with tack-only fixation has been reported by Carbajo et al. 8 and IEHS, 32 respectively. This review suggests that using double-crown tack-only technique in mesh fixation is as effective as tacks in conjunction with suture technique for small- and large-size primary ventral and incisional hernias. However, it was not possible to make any recommendation in favor of using single-crown tack fixation technique in LVHR based on only one study with 6 months of FU. Also, we could not answer the question whether or not the hernias near bony prominences have more influence in recurrence rate postlaparoscopic repair as they were excluded from all included trials.
Recently, new techniques have emerged to improve the outcomes of ventral hernia repair. Absorbable tacks have been recently introduced to overcome the inherent problems associated with the conventional nonabsorbable tacks, including chronic pain and intraperitoneal adhesions, even though the latter is still considered the standard method of fixation in LVHR. 39 To date, two RCTs, comparing absorbable to nonabsorbable tack fixation, reported comparable results with respect to postoperative pain and complications,27,28 and the other available studies are either observational 40 or retrospective. 41 These studies were not included in this meta-analysis to ensure the intervention homogeneity among the analyzed data, Moreover, there are a few reports comparing robotic approach using SMF to standard laparoscopic approach using tack fixation, but was not included because of the nonrandomized nature.42,43 It is worth mentioning that with every emerging technology, the cost, and its economic impact remain an issue. Regarding LVHR, the cost may play a role in choosing between repair approaches and fixation techniques. In this review, only two trials are reported on this variable, both showed a higher overall cost with the tacks compared to the suture fixation, despite the shorter operative time.22,26 Unfortunately, this outcome could not be pooled because of inadequate data. Future RCTs, particularly those evaluating new technologies, will be necessary to fully assess the cost-effectiveness as it may affect choosing between interventions.
The International Association for the Study of Pain defines chronic pain as “that which persists beyond the normal time frame for healing, usually taken to be 3 months.” 44 The method of mesh fixation may influence chronic pain due to trapping cutaneous nerves or placing the muscle under tension. Based on this assumption, various strategies to tackle postoperative pain have been used with favorable, but controversial outcomes. Only two prospective trials have reported on the use of fibrin sealant in LVHR.15,30 Eriksen et al. 30 identified a significant reduction in early postoperative PI with fibrin sealant compared to tacks; also, the proportion of patients suffering moderate to severe pain ‘defined as VAS ≥5 cm or VRS (verbal rating score) ≥2 cm was significantly higher in the TMF on day 2. However, 1-year FU by the same group reported no difference in both chronic pain rate as well as the effect of chronic pain on different QoL parameters between the two fixation methods. 45 The results, however, do suggest that the use of fibrin glue for small umbilical hernias achieves slightly less pain in early postoperative period. Even though the study was not powered for recurrence, the rate was found to be higher than expected, especially in patients with larger hernia defects. For this reason, fibrin sealant cannot be recommended routinely for intraperitoneal mesh fixation. Nevertheless, a less invasive fixation method like fibrin sealant in LVHR is a prosperous field for further investigation.
Studies on the mechanical behavior of the whole fascia-mesh system have posed the hypothesis that “the mesh, the fixation material, and the fascia are functional systems that should not be treated and described separately.”46–48 The elastic property of the human fascia and the junction forces that affect the fascia-mesh connection should be well understood and considered.49,50 Based on this assumption, a recent data from Maciej Pawlak et al. 29 demonstrated that elastic mesh/fixation system is superior to the fixed mesh/fixation system in terms of PI and recurrence post-LVHR. They demonstrated that one of the most important factors affecting the tearing process of the tacks is the elastic physiology of the mesh; while it is fixed to the abdominal wall, the elastic mesh fixation system can emulate the elastic properties of the human fascia, and thus, the tearing effect will be decreased. However, the short-term FU makes its clinical validation questionable. Furthermore, many authors considered the site where the mesh is fixed and how effective the interface between the parietal side of the mesh and the abdominal wall is more important than the type of fixation used.23,29 To make it clearer, with adopting single-crown fixation near the edge of the mesh, the effective interface and thus the likelihood of proper mesh ingrowth and incorporation to the abdominal wall will be decreased; this is basically because of the movement of the abdominal wall and the possibility of the presence of seroma in between. On the other hand, this interface will be enhanced by adopting the double-crown fixation technique or could even increase to nearly the complete mesh surface by using other nonmechanical fixation alternatives like glue or self-fixing mesh. 23
Based on the recommendation of IMMPACT and IASP group in 2005,17,18 this review demonstrates that the available RCTs, which examined postoperative pain after LVHR, are not robust enough; this could be attributed to the lack of adherence to the standards in methodology. Although the majority of the trials provided, to a certain extent, a similar definition for chronic pain and used validated assessment tools, the variability in interpretation of these definitions affects the uniformity of outcome reporting and limits quantitative analyses. Some studies defined chronic pain based solely on time factors, “discomfort or any pain with VAS above 0 on a scale of 0–10 that lasts more than 3 months,” while others incorporated PI factor, “patient needs to express at least a VAS of two or three on a scale of 0–10 to be considered pain.” Such inconsistency in reporting of chronic pain obviously influences incidence and prevalence rates. Measurements of PI and its impact on QOL were assessed only in two trials22,24 and largely centered on the ability to return to work, to resume normal daily activities, and to an extent the improvement from baseline pain. Others reported on discomfort, fatigue, and overall satisfaction. Most authors believe that QoL rather than VAS scores may better represent the outcomes after LVHR. Mild chronic pain or occasional discomfort is unlikely to have a major effect on the patient's life unless associated with other factors like patient activity and occupation. Furthermore, a greater number of the included studies provided no preoperative baseline assessment of chronic pain. Baseline measurements are necessary for a meaningful interpretation of postoperative results. Also, preoperative pain is a known risk factor for developing chronic pain. 23 Therefore, trials on LVHR reporting on pain outcome might improve by adopting a common standard that includes one clear definition of chronic pain, incorporating pain duration, PI, and the effects of chronic pain on daily activities. In general, RCTs are designed to minimize the risk of bias and remain the source of best evidence. However, in LVHR, between-study variability still exists due to hernia variables, patient variables, available hernia repair materials, and techniques used. To solve this issue, a common study methodology is needed that uses well-defined standard outcome parameters, which are evaluated with validated instruments and over a sufficient period of FU. EuraHS (European Registry for Abdominal Wall HerniaS) 51 has offered an online platform for registration and outcome measurement of abdominal wall hernia repairs with clear definitions and classifications. This database will increase the quality and quantity of outcome reports in the repair of ventral hernias.
Conclusion
Based on this meta-analysis, tack and SMF techniques produce comparable results with respect to postoperative chronic pain incidence and PI, and hernia recurrence for laparoscopic repair of ventral hernias. Length of hospital stay is similar; however, operative time is shorter with tack fixation. This review also highlights the nonuniformity of the time points of pain assessment and pain definitions among the analyzed trials. Future trials should ensure that their methodology and outcome reporting adhere to the standardized core outcomes recommended by the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials group (2005), and the International Association for Study of Pain.
Footnotes
Disclosure Statement
No competing financial interests exist.