
Abstract
Abstract
Aim:
To compare the short-term and long-term outcomes of laparoscopic versus open surgery for low rectal cancer.
Methods:
Patients with low rectal cancer who underwent laparoscopic or open surgery at our department from January 2009 to December 2013 were enrolled in this retrospective study. The primary end points were 3-year local recurrence and overall and disease-free survival (DFS) rates. Secondary end points were intraoperative and postoperative outcomes.
Results:
Laparoscopic group had longer operative time (165.0 versus 140.0, P < .001), less blood loss (20.0 versus 40.0, P < .001), shorter length of incision (5.0 versus 18.0, P < .001), and more lymph node harvested (11.0 versus 9.0, P = .002). However, time to first flatus (P = .941), postoperative hospital stay (P = .095), postoperative complications (P = .155), and 30-day mortality (P = .683) was similar between two groups. With the median follow-up period of 65 months, the 3-year local recurrence rate was 4.3% in laparoscopic group and 7.5% in open group (P = .077); the 3-year overall and DFS rates were similar in two groups (85.9% versus 88.8%, P = .229 and 76.9% versus 79.2%, P = .448, respectively); and the overall and DFS curves were comparable between two groups (hazard ratio [HR] = 0.858, 95% confidence intervals [CI] 0.709–1.037, P = .112 and HR = 1.076, 95% CI 0.834–1.389, P = .275, respectively).
Conclusions:
Laparoscopic surgery is safe and has equivalent long-term oncologic outcomes for low rectal cancer when compared to open surgery. Furthermore, large-scale, prospective randomized clinical trials are needed to confirm the present findings.
Introduction
S
Three RCTs (CLASICC,6,12 COLOR II,13,14 and COREAN15,16 trial) reported that compared to open surgery, laparoscopic surgery for rectal cancer provided quicker recovery of bowel function, shorter hospital stay, similar resection margins and completeness of resection, and comparable 3-year survival. On the contrary, other two RCTs (ALaCaRT and ACOSOG Z6051) failed to validate noninferiority in terms of pathological and adequate surgical resection outcomes when laparoscopic surgery was compared to open surgery.17,18 Besides, ALaCaRT reported that there was no significant difference between two groups in terms of length of hospital stay, intensive care unit stay, or analgesic requirement, 17 and ACOSOG Z6051 reported that there was no significant difference between the two procedures in terms of length of hospital stay, readmission within a month, or severe complications. 18
Some surgeons think that the possible explanation for conflicting results may be that those RCTs included mixed rectal cancer (high, middle, and low rectal cancers). Most of high and middle rectal cancers can undergo partial mesorectal excision, while all low rectal cancers must undergo total mesorectal excision (TME). However, evidence on laparoscopic versus open surgery for low rectal cancer is limited. Therefore, we conduct this retrospective cohort study to compare the short-term and long-term outcomes of the two procedures for low rectal cancer.
Materials and Methods
Study patients
Rectal cancer patients who underwent surgery at the Department of Gastrointestinal Surgery, West China Hospital, Sichuan University, from January 2009 to December 2013 were enrolled in this retrospective study. Medical records of patients were reviewed retrospectively. Patient demographics, perioperative outcomes, and pathological characteristics were collected, as well as survival data. Distance of tumor from the anal verge was measured by hard straight colonoscopy. Tumor-node-metastasis (TNM) stage was assessed according to the American Joint Committee on Cancer TNM staging standard, seventh edition. In our department, all patients were put under a similar enhanced postoperative recovery care protocol. The follow-up was done regularly, which was described in detail in our previous work. 19 The last follow-up time was until November March 2017. No ethical approval or informed consent was required because it was a retrospective study.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) histologically confirmed rectal adenocarcinoma; 2) low rectal cancer (distance of tumor from the anal verge ≤5 cm); and (3) laparoscopic or open radical surgery. Exclusion criteria were as follows: (1) distance of tumor from the anal verge >5 cm; (2) multiple colorectal cancers; (3) tumors infiltrating to adjacent organs or synchronous metastatic diseases; (4) local recurrent rectal cancer; (5) medical history with malignance in any other organs; (6) transanal local excision or trans-sacrococcygeal excision; and (7) American Society of Anesthesiologists >3.
Surgical techniques
All procedures were completed by staff colorectal surgeons who were highly experienced in rectal cancer surgery, following the same oncologic and clinical principles, (TME principles) as described by Heald. 20 Further detailed procedures were described in previous literatures.21–23 All laparoscopic surgeries were performed by one surgeon, while open surgeries were performed by three other surgeons.
End points
The primary end points of this study were 3-year local recurrence, overall survival (OS), and disease-free survival (DFS) rate. Secondary end points included operative time, blood loss, length of incision, lymph node harvested, conversion, postoperative hospital stay, postoperative complications, and 30-day mortality. Conversion was defined as the length of incision beyond 8 cm to complete the surgical procedures and was assigned to open surgery. Postoperative complications were considered if they occurred within 90 days after surgery and were stratified according to the Clavien-Dindo classification. 24 Major complications were defined as complications with a grade 3 and higher of the Clavien-Dindo classification. Mortality was recorded if they occurred within 30 days after surgery.
Statistical analysis
Patients were stratified into laparoscopic and open groups. The categorical variables were analyzed by the χ2 test or Fisher's exact test. The ranked data were analyzed by Wilcoxon rank-sum test. The continuous variables were described as median (inter-quartile range [IQR]) and were compared using Student's t-test or Wilcoxon rank-sum test, depending on normality. The OS and DFS were analyzed and compared using the Kaplan-Meier method. Multivariate analysis was performed using Cox proportional hazards regression. Data analyses were all carried out using SPSS software (version 22.0; SPSS, Inc., Chicago, IL). A P value <.05 was defined as statistical significance.
Results
Patient characteristics
Patient selection diagram is shown in Figure 1. A total of 1127 patients met the study criteria. 236 (20.9%) patients were lost to follow-up. Therefore, 891 (79.1%) patients were enrolled in analysis (277 in laparoscopic group and 614 in open group). Patient characteristics between groups are shown in Table 1. The median (IQR) age was 59.0 (47.0–67.5) years for the laparoscopic group and 58.0 (48.0–66.0) years for the open group (P = .379). There were no significant differences between two groups in gender, body mass index, American Society of Anesthesiologists, carcinoembryonic antigen, or previous abdominal surgery. However, patients who underwent neoadjuvant therapy were more in laparoscopic group (20.6% versus 6.8%, P < .001).
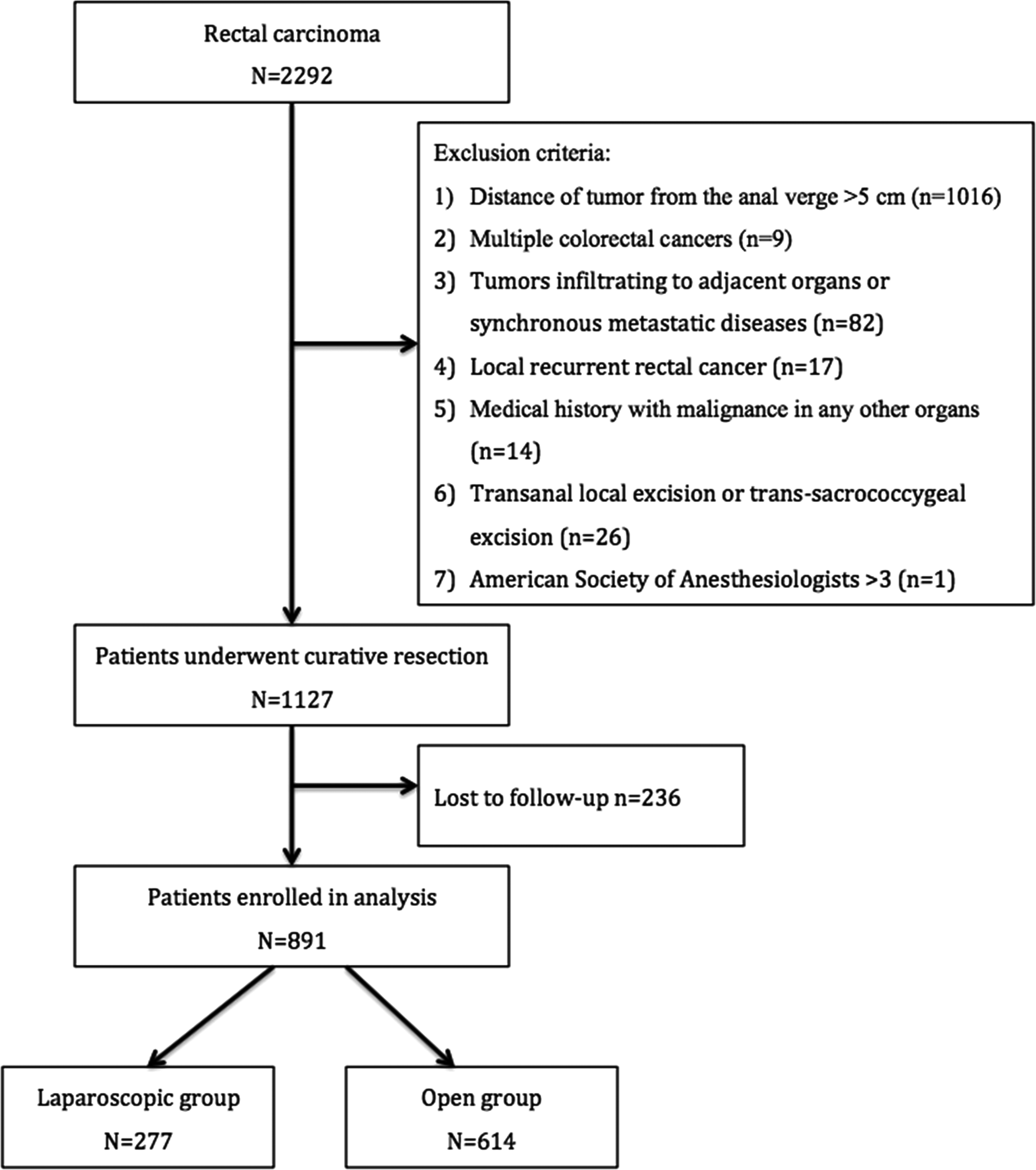
Patient selection diagram.
Data are shown as median (inter-quartile range).
ASA, American Society of Anesthesiologists; BMI, body mass index; CEA, carcinoembryonic antigen; PAS, previous abdominal surgery.
Short-term outcomes
Intraoperative and postoperative outcomes are shown in Table 2. The operative time was longer in the laparoscopic group [165.0 (145.0–185.0) versus 140.0 (105.0–185.0), P < .001]. However, the estimated blood loss was less in the laparoscopic group [20.0 (20.0–30.0) versus 40.0 (20.0–80.0), P < .001], and the length of incision was obviously shorter in the laparoscopic group [5.0 (5.0–6.0) versus 18.0 (16.0–18.0), P < .001]. No significant difference was observed in either time to first flatus [4.0 (3.0–4.0) versus 4.0 (3.0–4.0), P = .941] or postoperative hospital stay [9.0 (8.0–11.0) versus 9.0 (7.0–11.0), P = .095]. Total postoperative complication rate was 23.5% in the laparoscopic group and 28.0% in the open group (P = .155). No difference was observed for major complications between groups (4.7% versus 5.5%, P = .602). A total of 39 patients underwent reoperation [10 (3.6%) in laparoscopic group and 29 (4.7%) in open group, P = .453]. Besides, the 30-day mortality rate was 0.4% in the laparoscopic group and 0.7% in the open group (P = .683). Also, no difference was observed for adjuvant therapy (P = .761).
Data are shown as median (inter-quartile range).
Major complications were defined as complications with a grade 3 and higher of the Clavien-Dindo classification.
Table 3 summarizes the specific postoperative complications. The rates of abdominal infection and incisional complications were significantly lower in the laparoscopic group (0.4% versus 2.6%, P = .030 and 5.8% versus 10.3%, P = .029, respectively). Other complications were comparable between the two groups.
Others included colon rupture, vomit, hepatic encephalopathy, nasal bleeding, pelvic effusion, gout flare, chylous fistula, delirium, gynecological infections, and so on.
Pathological outcomes
Pathological outcomes are presented in Table 4. Tumor size, differentiation, N stage, T stage, TNM stage, lymphovascular invasion, and perineural invasion were comparable between the two groups, while the lymph node harvested was significantly more in the laparoscopic group [11.0 (7.0–16.0) versus 9.0 (6.0–14.0), P = .002].
Data are shown as median (inter-quartile range).
G, grade; TNM, tumor-node-metastasis.
Long-term outcomes
The median (IQR) follow-up period was 65 (46–77) months. The 3-year local recurrence rate was 4.3% in the laparoscopic group and 7.5% in the open group (P = .077). Besides, the 3-year OS and DFS rates were similar in two groups (85.9% versus 88.8%, P = .229 and 76.9% versus 79.2%, P = .448, respectively). The survival curves of OS and DFS are shown in Figure 2. Both OS and DFS were comparable in laparoscopic and open groups (hazard ratio [HR] = 0.868, 95% confidence intervals [CI]: 0.653–1.153, P = .328 and HR = 0.996, 95% CI: 0.765–1.296, P = .974, respectively). Besides, in the subgroup analysis by TNM stage, there was no statistical difference between laparoscopic and open groups in terms of OS or DFS (Fig. 3).
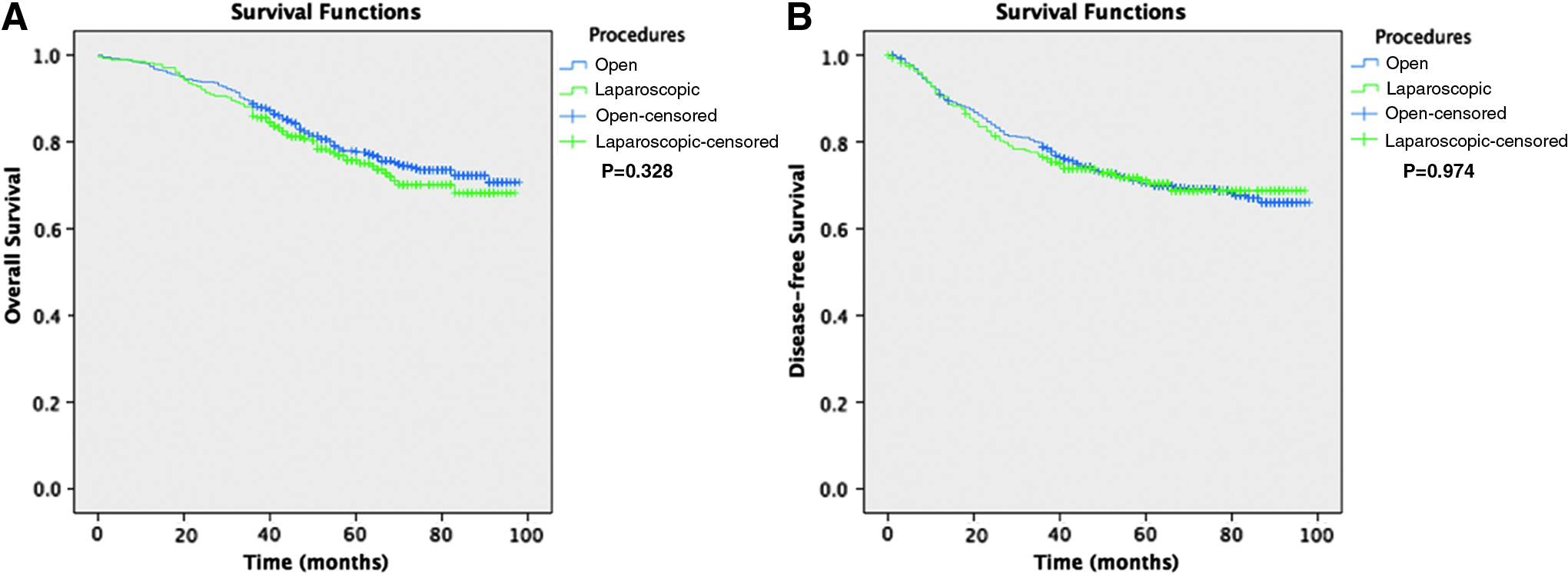
Kaplan-Meier curve of overall and disease-free survival for all patients.

Kaplan-Meier curve of overall and disease-free survival for patients with different TNM stage.
Prognostic factors
In multivariate analysis, the prognostic factors impacting OS were age (HR = 1.56, P = .004), carcinoembryonic antigen (HR = 1.43, P = .015), differentiation (HR = 1.78, P < .001), TNM stage (HR = 1.83, P = .023 and HR = 4.91, P < .001), and perineural invasion (HR = 2.25, P = .005), and the prognostic factors impacting DFS were differentiation (HR = 1.62, P < .001), TNM stage (HR = 1.70, P = .026 and HR = 4.55, P < .001), and perineural invasion (HR = 1.76, P = .043) (Table 5).
ASA, American Society of Anesthesiologists; BMI, body mass index; CEA, carcinoembryonic antigen; CI, confidence intervals; HR, hazard ratio; LVI, lymphovascular invasion; OS, overall survival; PNI, perineural invasion; TNM, tumor-node-metastasis.
Discussion
Several high-quality RCTs have attempted to compare laparoscopic and open surgery for rectal cancer, but results, especially pathologic results, are conflicting.12–18 The location of rectal cancer might affect surgical results, but those RCTs included mixed rectal cancer (high, middle, and low rectal cancers). Our cohort study aimed to assess short-term and long-term outcomes in patients with low rectal cancer undergoing laparoscopic surgery. We found that the OS and DFS were comparable between the two groups; also comparable were time to first flatus, postoperative hospital stay, postoperative complications and mortality, and 3-year local recurrence, OS and DFS rates. However, laparoscopic surgery provided significantly less blood loss, shorter length of incision, and more lymph nodes harvested, although the operative time was longer in the laparoscopic group when compared to open surgery.
Several studies compared laparoscopic and open abdominoperineal resection (APR) for low rectal cancers25–28 and concluded that laparoscopic APR showed significantly earlier first flatus and length of hospital stay. Besides, another study comparing laparoscopic and open TME with anal sphincter preservation for low rectal cancer also found the same results. 29 However, the sample size of all these studies was small. In our large cohort study, we found that time to first flatus and postoperative hospital stay was comparable between the two groups. As for survival outcomes, the results were also similar in the two groups. Wang et al. 25 reported that the 3-year DFS rate in laparoscopic and open APR group was 88.1% and 71.9%, respectively (P = .317). Odermatt et al. 26 reported that the 3-year OS and DFS rate was 78% and 72% in laparoscopic group and 71% and 57% in open group (P = .167 and P = .186, respectively). Ng et al. 28 reported that the 5-year OS rate of the laparoscopic and open group was 75.2% and 76.5% (P = .20), and the 5-year DFS rate was 78.1% and 73.6% (P = .55). In our study, the 3-year OS and DFS rates were also similar in the laparoscopic and open group (85.9% versus 88.8%, P = .229 and 76.9% versus 79.2%, P = .448, respectively). There was no study comparing the local recurrence rate between the laparoscopic and open group. In this work, although there was no significant difference between the two groups, the 3-year local recurrence rate in the laparoscopic group (4.3%) was slightly lower than that in the open group (7.5%).
Literature has demonstrated that neoadjuvant chemoradiation for T3-T4N0 or T1-4N1-2 tumors has resulted in a decrease in local recurrence and increases the probability of curative tumor resection and the rates of sphincter-saving procedures for stage II and III rectal cancer patients.30–32 However, the overall rate of neoadjuvant chemoradiation in this study was only 11.1% (20.6% in laparoscopic group and 6.8% in open group). This was because neoadjuvant chemoradiation was not routinely recommended in western China during this period for T3-T4aN0 or T1-4aN1-2 tumors, while only T4b tumors were routinely suggested to undergo neoadjuvant chemoradiation, which were excluded in our study.
With regard to conversion, it is an important concern as it not only has higher morbidity but may also affect survival outcome.6,33–36 One Cochrane review has reported that conversion rates in laparoscopic surgery for rectal cancer can be as high as 35%. 37 In our study, only 4 (1.3%) patients were converted to open surgery. We thought this very low conversion rate was contributed to the high operation volume.
There are several limitations of this study. First, it is a retrospective study, which makes it susceptible to the effects of confounding and selection bias. Second, we could not collect the circumferential resection margin (CRM) data. Thus, we did not report the rate of positive CRM, although a CRM of 1 mm is a strong predictor of local recurrence. 38 Third, although we tried several ways such as searching electronic medical records, making calls, and writing letters to follow up, the rate of loss to follow-up was still 20.9%, which was higher than we expected. Despite these limitations, we believe that our results provide valuable evidence that laparoscopic surgery is safe and feasible for low rectal cancer.
In conclusion, laparoscopic surgery is safe and has equivalent long-term oncologic outcomes for low rectal cancer when compared to open surgery. Furthermore, large-scale, prospective randomized clinical trials are needed to confirm these findings.
Footnotes
Acknowledgments
This work was supported by the Science and Technology Support Program of the Science and Technology Department of Sichuan Province (No. 2016SZ0043).
Disclosure Statement
No competing financial interests exist.