
Abstract
Abstract
Introduction:
Respiratory manifestations of gastroesophageal reflux disease (GERD), particularly chronic cough, are being recognized with increased frequency in children. This survey aimed to investigate the efficacy of laparoscopic Nissen fundoplication for treatment of GERD-related respiratory symptoms not responsive to medical therapy in neurological normal children.
Materials and Methods:
We collected data of children with GERD-related respiratory complaints not responsive to medical therapy who underwent laparoscopic Nissen fundoplication in four European centers of Pediatric Surgery over a 10-year period. We excluded children with neurological impairment.
Results:
A total of 220 laparoscopic Nissen procedures were performed in the period 2005–2015. Twenty-four (12 boys and 12 girls, average age 9.5 years) out of the 220 patients (10.9%) presented with chronic cough and other respiratory manifestations, including asthma, reactive airway disease, and recurrent pneumonia. Average operative time was 65 minutes (range 45–100). As for postoperative complications, two tight wraps requiring endoscopic dilatation (IIIb Clavien) and two relapses of GERD for slipped Nissen requiring reoperation (IIIb Clavien) were recorded. None of these complications occurred in the group of patients with GERD-related respiratory symptoms. At follow-up evaluation, respiratory symptoms disappeared with a significant improvement of quality of life scoring (I Grade Visick) in 22/24 patients (91.6%).
Conclusion:
Our results confirm that GERD should be investigated as one of the possible etiologic factors in any child with persistent respiratory complaints. In patients with symptoms not responsive to medical therapy, laparoscopic Nissen fundoplication is the treatment of choice with a very high success rate (>90% in our series), a very low morbidity, a significant improvement in airway symptoms, and a marked reduction in the need for medications.
Introduction
G
Several mechanisms have been claimed to play a role in GERD-related cough, including the effect of refluxate on the esophagus, larynx, or bronchi. There are two main mechanisms in the pathogenesis of GERD-related cough. The first one is named “esophago-bronchial reflex,” and it is based on shared vagal innervations of the distal esophagus and airways. According to this theory, distal esophageal sensory nerve terminals stimulated by refluxate activate a reflex resulting in cough. The second mechanism is microaspiration, in which refluxate reaches the airways through the proximal esophagus and larynx directly resulting in cough. The risk of microaspiration is thought to be increased by decreased sensitivity of protective laryngeal and pharyngeal reflexes, impaired coordination of swallowing, and esophageal dysmotility.6,7
Different techniques, such as simultaneous measurement of esophageal and tracheal pH, scintigraphic scans of the lungs, detection of pepsin in bronchoalveolar lavage (BAL) or saliva, and detection of bile acids and lipid-laden alveolar macrophages (LLAMs) in airway specimens, have been used to identify microaspiration of refluxate into airways. Studies on those measurement techniques have been conducted in pediatric populations.8–11
Early diagnosis and antireflux medical therapy in cases with GERD-related respiratory complaints can result in significant improvement in symptoms.12,13 However, in patients not responsive to medical therapy, laparoscopic GER surgery improves airway symptoms with a success rate variable from 70% to 100%. The majority of these reports are focused on adult population.14–16
Very limited data are available in the literature about the role of laparoscopic GER surgery for treatment of GERD-related respiratory symptoms in pediatric patients.17–20
In the majority of cases, pediatric gastroenterologists are very reluctant to confirm the indications for surgery in pediatric patients with GER and persistent respiratory symptoms because they prefer to continue to treat these patients with only medical therapy.
This survey aimed to investigate the efficacy of laparoscopic Nissen fundoplication for treatment of GERD-related respiratory symptoms not responsive to medical therapy in neurological normal children.
Materials and Methods
We collected the data of children with GERD-related chronic cough and other respiratory complaints not responsive to medical antireflux therapy who underwent laparoscopic Nissen fundoplication in four European centers of Pediatric Surgery over a 10-year period (2005–2015).
The exclusion criteria were as follows: neurological impairment, congenital heart disease, tracheoesophageal fistula, presence of ear-nose-throat pathologies, immunosuppression, any other disease that can lead to aspiration, and findings compatible with upper airway cough syndrome.
All patients included in the study presented persistent respiratory symptoms beyond 8 weeks (such as cough, wheeze, asthma, respiratory distress, and bronchopneumonia) or recurrence of respiratory symptoms (more than twice a year for two consecutive years) that were refractory to an adequate antireflux medical treatment which included both nonpharmacological therapy (frequent small thickened feeds, prone/upright position during waking hours) and pharmacological therapy (prokinetics, H2 blockers, and proton pump inhibitors [PPI] in appropriate dosages) for at least 6–12 months.
Preoperative workup included chest X-ray and pH-impedenziometry in all patients. Esophageal pH examination results were considered positive for GERD-related respiratory symptoms if they were pathologic or if there was a significant correlation between symptoms and pH drop in the distal and proximal recording channels (a pH drop of <4 during the respiratory symptom period was considered significant).
Upper gastrointestinal endoscopy was performed to identify gross abnormalities in the esophagus, such as mucosal erythema, linear ulceration, bleeding, and stricture. Upper airway and bronchial endoscopy associated with BAL was performed in only one center to assess the LLAM scoring and to demonstrate aspiration events.
Indications for fundoplication were discussed individually for each patient within a pulmonology board between pediatricians and surgeons, after evaluation of mentioned diagnostic findings. Surgery was performed after ineffective medical treatment which was administered over a period of 6–12 months and resulted in worsening or recurrence of symptoms after drug discontinuation, during the treatment itself, or because family compliance was lacking.
A laparoscopic four-trocar 360° Nissen fundoplication was performed in all patients. With regard to operative technique, the operation included three steps in each case as follows: (1) dissection of the gastroesophageal junction and the lower esophagus; (2) crural repair; and (3) formation of a 360° wrap using nonresorbable sutures.
Patients' records were analyzed with regard to the following: outcome of surgery, postoperative complications, relapse of disease and need for reoperations, and outcome of respiratory complaints after surgical treatment.
To objectively evaluate postoperative outcome of both upper gastrointestinal symptoms and respiratory complaints in our patients, we applied the modified Visick classification and the Cough Symptom Score (CSS). The Visick grading system is used to assess the subjective effect of antireflux surgery, evaluating resolution, persistence, or worsening of the symptoms, impact of surgery on quality of life, and need for medications after surgery (Table 1). The CSS is a 5-point scale aiming to assess the severity of the cough and the patient's perception (Table 2).
The study received the appropriate institutional review board approval. Statistical analysis was carried out using the Statistical Package for Social Sciences (SPSS, Inc., Chicago, IL), version 13.0. Data were compared using the Student's t-test. Significance was defined as P < .05.
Results
A total of 220 laparoscopic Nissen procedures were performed in all centers during the period 2005–2015. Twenty-four out of the 220 patients (10.9%) presented with GERD-related respiratory symptoms. There were 12 boys and 12 girls, with an average age of 9.5 years (range 6.5–17 years). The average weight of patients was 29 kg (range 15–65 kg).
Chronic cough was the principal symptom in 20 patients (83.3%), whereas in the remaining 4 children (16.7%) the main respiratory manifestations included asthma, reactive airway disease, and recurrent pneumonia. In most patients, the respiratory symptoms, especially the cough, were so strong that it limited their scholar and social activity. Age of onset of respiratory symptoms was <1 year in 15 cases (62.5%). Nocturnal symptoms of cough and wheeze were noted in 13/24 patients (54.1%). None of the cases of GERD-related reactive airway disease had a family history of asthma.
Only 3 cases (12.5%) had typical gastrointestinal symptoms attributed to GER. The other 21 cases (87.5%) did not have any gastrointestinal symptoms of GER.
Pathologies associated were esophagitis in 4 patients and Barrett's esophagus in 2 children.
Fourteen out of the 24 cases (58.3%) were detected to have severe reflux, 7 patients (29.1%) presented moderate reflux, and 3 patients (12.5%) had mild reflux. The DeMeester scores ranged from 20 to 240 (average 42), with 55% showing an association between reflux and respiratory symptoms.
Eight patients (33.4%) had a preoperative bronchoscopy and BAL, and all of them had significant granulocytosis and LLAM (>5%) in their BAL samples.
Before surgery, all patients were treated with antireflux therapy for 6–12 months and after failure of medical treatment they were candidates to fundoplication. Fourteen patients (58.3%) were treated preoperatively with inhalative steroids and inhalative beta-2-mimetics, whereas 8 patients (33.3%) received oral steroids.
Average operative time was 65 minutes (range 45–100). No conversion to open surgery was reported. As for postoperative outcome, following four complications were reported with an overall complication rate of 1.8% (4/220): two tight wraps requiring endoscopic dilatation (IIIb Clavien) and two relapses of GERD for slipped Nissen requiring reoperation (IIIb Clavien). None of these complications occurred in the group of patients with GERD-related respiratory symptoms.
Average follow-up length was 7 years (range 2–12). Patients were assessed with anamnestic evaluation and physical examination at 1, 3, 6, and 12 months after surgery and thereafter with annual clinical controls. Radiologic examinations were performed only in presence of postoperative symptoms or other problems.
At clinical controls, respiratory symptoms disappeared completely with a significant improvement of quality of life scoring in 22/24 patients (91.6%) after 2.8 ± 4.6 months. In fact, these 22 patients (91.6%) were assessed as Grade I according to Visick classification as they were asymptomatic, with no need for any medication and improved quality of life, whereas the remaining 2 patients (8.4%) were classified as Grade III according to Visick as they presented moderate symptoms with persistent need for medications and quality of life unaffected. These 2 patients with postoperative persistence of respiratory symptoms were managed by pulmonologists.
In regard to assessment of the cough severity, the 20 patients with GERD-related chronic cough recorded a preoperative CSS daytime average score of 4.3 ± 0.5 and a CSS nighttime average score of 3.8 ± 0.4. Postoperatively, both CSS daytime (0 ± 0.7) and nighttime (0 ± 0.5) average scores significantly improved in all these patients (P = .001).
In regard to postoperative medication course, 85.7% of patients receiving inhalative steroids and inhalative beta-2-mimetics were completely weaned after 5.4 ± 2.6 months, while 14.3% significantly reduced their usage after 4.5 ± 3.9 months. Of those patients receiving oral steroids, 100% were completely weaned after 4.4 ± 3.1 months. Of the patients, 95.8% discontinued their use of PPI after 0.3 ± 0.8 months, while 4.2% of patients significantly reduced their usage after 1 month (Fig. 1).
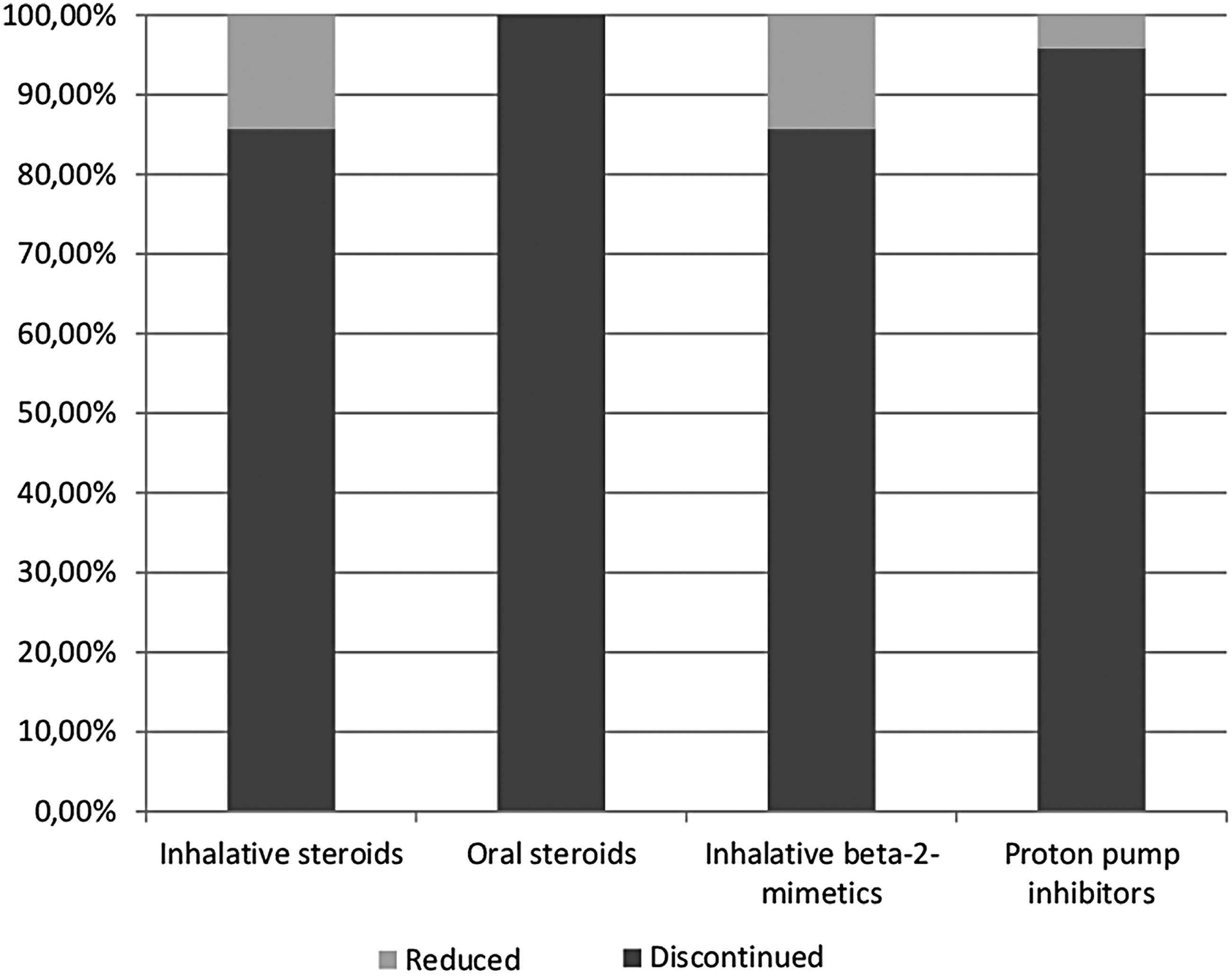
Course of postoperative medication.
All patients' demographics and outcome parameters are reported in Table 3.
CSS, Cough Symptom Score; GERD, gastroesophageal reflux disease; PPI, proton pump inhibitors.
Discussion
The relationship between GERD and respiratory disease in infants and children has been shown to be present in many forms.1,17 Hoarseness, sore throat, chronic cough, bronchitis, asthma, recurrent pneumonia, chest pain, and ear pain are the most common respiratory complaints reported. Epidemiologic data show that pulmonary symptoms occur in up to 50% of patients with GERD. 21
Several studies have shown that intensive medical management of GERD often fails to have any effect on the patients' respiratory symptoms. Shapiro and Christie reported a significant correlation between GERD and steroid-dependent asthma, but failed to show an improvement in their airway disease during a 3-week period of intensive medical therapy for their GER. 22 Fonkalsrud et al. suggested that in this subset of patients, medical therapy may be inadequate and surgical correction may be more efficacious. They reported that 90% of their patients who failed to respond to medical therapy had symptomatic improvement of their respiratory symptoms after fundoplication. 23 Rothenberg et al. showed that in this subset of patients, medical therapy may be inadequate in interrupting the reflex pathway between esophageal irritation and bronchoconstriction, but that surgical correction may act as a more effective barrier. 20
Surgical management of GERD by fundoplication has repeatedly proven to be superior to medical therapy in children with chronic airway disease (CAD) and GERD.6,24 Further support comes from several studies describing a postoperative improvement of respiratory symptoms and significant decrease in steroid and bronchodilator dose in 80%–90% of patients.17,20 Our results confirmed this evidence as we obtained a complete weaning from inhalative steroids and inhalative beta-2-mimetics in 85.7% of our patients and a significant reduction of these medications in 14.3% of cases.
The success of surgery depends on identifying patients who are most likely to benefit from surgical intervention. 25 Patients with pulmonary symptoms frequently have asymptomatic GERD; as reported in our series, 87.5% of patients did not have any gastrointestinal symptoms of GER. In this group, a high index of suspicion is needed to identify GERD as a contributing factor. A properly taken clinical history with detailed questions about the character and timing of respiratory and esophageal symptoms is helpful in finding suitable candidates for antireflux surgery. When patients are chosen appropriately, surgical therapy appears to be superior to medical therapy for alleviating supraesophageal symptoms. 21
Despite this evidence, pediatric gastroenterologists are often very reluctant to confirm the indications for surgery in pediatric patients with GER and persistent respiratory symptoms because they prefer to continue to treat these patients with only medical therapy. In our series, in 5 patients with chronic cough not responsive to medical therapy and causing an important invalidation in their social and scholar activities, the surgical indication was confirmed by pediatric surgeons in disagreement with the pediatricians that were reluctant to candidate the patient to surgery. The parents agreed with the surgeons to operate their children and the cough disappeared completely without need of any medication, 2 months after surgery.
In addition, Rothenberg et al. described the reluctance of some colleagues to refer CAD patients for surgical antireflux procedures, for example, owing to the perceived surgical morbidity in this subgroup. 26
However, with the proven success of laparoscopic antireflux surgery even in those patients with severe respiratory impairment, the threshold to refer patients for surgical therapy has been lowered.27–30 Even in GERD patients with severe pulmonary problems who would not otherwise tolerate an abdominal operation, laparoscopic fundoplication can be performed safely and with high success rate. The minimal surgical trauma and postoperative pain associated with laparoscopic fundoplication result in less splinting and inhibition to deep breathing and coughing than seen in open surgery and result in fewer respiratory complications. 17 Our results are consistent with most reports of the literature; in fact, none of the postoperative complications reported in our series occurred in patients with GERD-related respiratory complaints.
In contrast to medical therapy, surgery can correct the antireflux barrier of the lower esophageal sphincter and restore the gastroesophageal junction by correcting the hiatal hernia. 31 Surgery provides continuous control of reflux, whereas medical therapy does not. Surgery prevents both acid and nonacid reflux and promotes gastric emptying.
It is also important to offer surgery early in the course of the disease to prevent the development of esophageal body motility dysfunction. In fact, relief of GERD-associated respiratory symptoms after antireflux surgery is not as good in patients with impaired esophageal body motility. 32
According to our experience, the surgical approach is mandatory when GERD is the suspected cause of respiratory complaints, and the response to medical therapy is partial or temporary. We reported a very low reflux recurrence rate (<1%) and complication risk (<2%), which suggest the effectiveness of an early surgical treatment. More importantly, none of the complications recorded in our series occurred in the group of patients with GERD-related respiratory symptoms.
It is fundamental to manage these patients in a multidisciplinary setting among pediatricians, pulmonologists, and surgeons, and the indications for surgery have to be established on an individual basis, according to the results of the diagnostic workup.
Another important consideration is that, analyzing the current pediatric literature, there are no reports of tools to assess impact of chronic cough on quality of life, specifically designed for pediatric patients. Adverse Cough Outcome Survey and Sickness Impact Profile have been described as valid tools to assess impact of chronic cough on quality of life in adults, but they have never been applied to a pediatric population. 33 To objectively evaluate postoperative outcome of both upper gastrointestinal symptoms and respiratory complaints in our patients, we applied the modified Visick classification 34 and the CSS. 35 Both these tools demonstrated a significant postoperative improvement of the severity of the symptoms, need for medications, and quality of life in most patients of our series.
In conclusion, our results confirm that GERD should be investigated as one of the possible etiologic factors in any child with chronic cough or other persistent respiratory complaints. In patients with symptoms not responsive to medical GER therapy, laparoscopic Nissen fundoplication should be considered the treatment of choice with a very high success rate (>90% in our series) and a very low morbidity rate. It allows a significant improvement of respiratory symptoms with a marked reduction in the need for medications and, consequently, a significant improvement in the quality of life of patients and their families.
Footnotes
Disclosure Statement
No competing financial interests exist.