
Abstract
Abstract
Objective:
To compare the perioperative outcomes of patients with uterine cancer, who were operated using advanced or conventional bipolar instruments.
Materials and Methods:
Patients with clinically early-stage endometrial cancer were randomized to advanced (LigaSure) or conventional (Robi forceps) bipolar groups. Surgeries were performed by laparoscopy. Hysterectomy and bilateral salpingo-oophorectomy with retroperitoneal lymphadenectomy were done in all cases. Primary endpoint of the study was to compare operation time for 2 groups. Other perioperative outcomes were also compared. ClinicalTrials.gov identifier number of the study was NCT02822820.
Results:
Sixty-eight cases with endometrial cancer were randomized to 2 groups and each group included 34 subjects. Mean age and body mass index of all cases were 56.8 ± 10.4 years and 31.1 ± 5.3 kg/m2, respectively. Mean operation time was found significantly shorter in advanced bipolar group (134.2 ± 29.7 minutes versus 163.5 ± 27.7 minutes, P < .001). The other variables investigated such as intraoperative blood loss, duration of hospital stay, and postoperative pain scores did not show statistically significant difference between the groups.
Conclusion:
Operation time was shorter in advanced bipolar group, however, advanced and conventional bipolar energy instruments were comparable for other perioperative outcomes in laparoscopic endometrial cancer surgery.
Introduction
L
In conventional bipolar electrosurgery, the two tines of the forceps perform the functions of both the active electrode and only the tissue grasped by the forceps is included in the electrical circuit. 3 The electrons travel from the generator to the forceps, through the tissue located between the jaws, and then directly back to the generator through the cable in the forceps. A neutral electrode is not required, thereby reducing the risk of electrical burns compared to monopolar devices. 3 Advancement in electrosurgery started with the introduction of bipolar vessel sealing capability, with the incorporation of tissue response generators.4–6 Advanced bipolar energy instruments denaturize collagen and elastin inside the vessel wall or tissue by using a highly pulsed or continuous electrical output.6,7 In addition to this mechanism, mechanical pressure to the tissue allows sealing of vessels up to 7 mm in diameter with up to thrice the normal systolic blood pressure. 8
Despite some favorable results,9,10 the advantages of advanced bipolar instruments in laparoscopic uterine cancer surgeries have not been evaluated sufficiently and proven yet. In this randomized controlled trial, we aimed to compare advanced and conventional bipolar energy instruments in terms of perioperative outcomes in patients who underwent laparoscopic surgery for clinically early-stage endometrial cancer.
Materials and Methods
Patients with clinically early-stage endometrial cancer were included in this single-blinded, single-center randomized clinical trial. The study was registered at ClinicalTrials.gov (NCT02822820) and performed between July 2016 and August 2017. Institutional Ethical Committee approval (Approval no.: 18-771-14, Date: November 10, 2014) and informed consent of the patients were obtained. Patients with histopathologic diagnosis of endometrial cancer were assessed for eligibility (Fig. 1). Transvaginal ultrasonography and chest X-ray were routine preoperative tests. Additional imaging studies, including computed tomography, magnetic resonance imaging, or 18F-PET/CT for high-risk tumors, were performed to exclude extrauterine disease. Patients with presumed uterine-confined endometrial cancer were randomized to advanced bipolar or conventional bipolar groups using a computer-based system at a ratio of 1:1. The patients did not know in which group they were assigned to. Patients' features, including age, body mass index, and previous abdominal surgery, were noted.
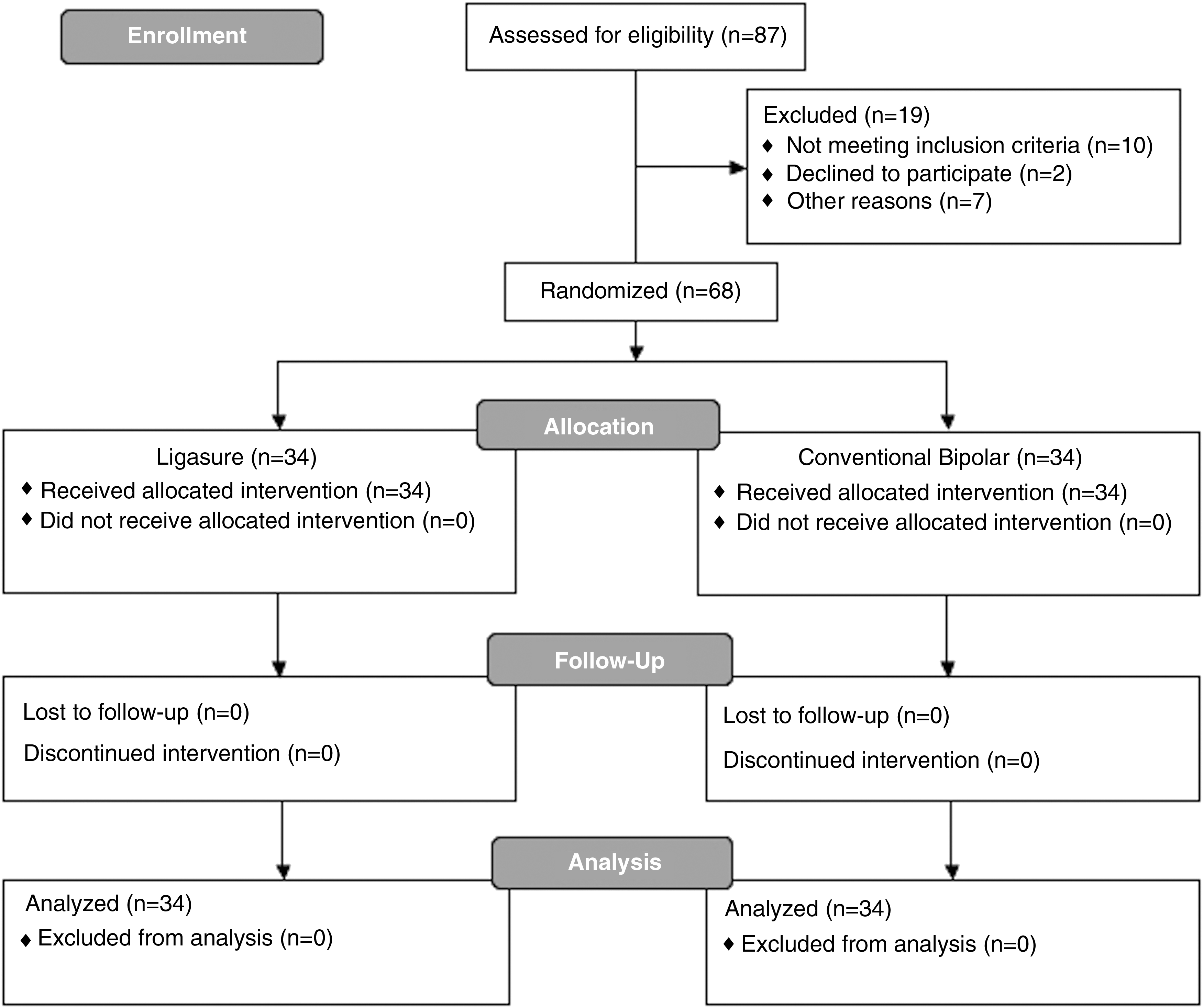
Flowchart of participants.
Surgeons had at least 10 years of postgraduate experience of endoscopic surgery, including lymphadenectomy. A first-year gynecologic oncology fellow was the first assistant. Surgeries were performed under general anesthesia by laparoscopy. Bilateral systematic pelvic lymphadenectomy was performed in all cases. Preoperative non-endometrioid histology, grade 3 endometrioid cancer, positive lymph nodes on intraoperative frozen section, or enlarged para-aortic nodes suspicious for malignancy were indications of para-aortic lymphadenectomy. Hysterectomy and bilateral salpingo-oophorectomy were performed after completion of lymphadenectomy.
Monopolar scissor (Karl Storz, Tutlingen, Germany) and bipolar forceps (Robi forceps, Karl Storz, Tuttlingen, Germany) were used for sealing, dissection, and hemostasis in the conventional bipolar group (Fig. 2A, B). Monopolar scissor was usually used as a cold knife. Advanced bipolar instrument (LigaSure Maryland Jaw Laparocopic 5 mm Sealer, Covidien, MA) was used in the advanced bipolar group (Fig. 2C). Colpotomy and detachment of the uterus from the vagina were done using a monopolar hook in both the study arms. Vaginal cuff closure was performed laparoscopically by using barbed suture. Operation time was defined as time from the initial skin incision to removal of last trocar.

Operative blood loss was calculated by subtracting irrigation solution volume used from the total amount of the fluid measured in the suction unite. Patients were positioned with reverse Trendelenburg position to remove all intra-abdominal fluid at the end of operations. Preoperative hemoglobin value, postoperative day 1 hemoglobin value, and difference between these values were also compared. Postoperative length of hospital stay was documented as day(s). Medication for postoperative analgesia was administered according to a guideline 11 and clinical standards. Postoperative pain was assessed by the visual analog scale (VAS), from 0 (no pain) to 10 (maximum pain), at the 8th and 24th hour postoperatively. Stable vital signs, flatus, spontaneous micturition, and no fever were the main criteria for discharge. Between 28th and 35th days postoperatively, all patients were seen, asked for any adverse events, and vaginal cuff was inspected.
Statistical analyses
Primary endpoint of the study was to compare the operation time. Operation time for the laparoscopic uterine cancer surgery that included total hysterectomy, bilateral salpingo-oophorectomy, and bilateral pelvic lymphadenectomy with or without para-aortic lymphadenectomy with the conventional bipolar instrument was ∼148 minutes in our clinic. 12 For an ∼20% reduction of operation time by using an advanced bipolar instrument, patient number in each study arm was calculated as 34, with 80% power and an α value of .05, for the confirmation of statistical significance.
Data analyses were performed by using SPSS Version 21.0 (IBM Corporation, Armonk, NY). Samples were tested with Shapiro–Wilk to determine normality of distributions. According to the results, parametric tests were preferred. Continuous variables were compared with Student's t test. Categorical variables were compared with chi-squared test. A P value <.05 was considered statistically significant.
Results
Sixty-eight eligible patients were randomized to advanced bipolar or conventional bipolar group and 34 subjects were included in each group (Fig. 1). Mean age and body mass index of all cases were 56.8 ± 10.4 years and 31.1 ± 5.3 kg/m2, respectively. In addition to total hysterectomy and bilateral salpingo-oophorectomy, 47 patients underwent bilateral pelvic lymphadenectomy and 21 patients underwent bilateral pelvic lymphadenectomy and para-aortic lymphadenectomy for endometrial cancers.
Comparison of 2 groups for demographic features, perioperative outcomes, and pathology results are shown in Tables 1 and 2. Operation time was found to be significantly shorter in the advanced bipolar group (134.2 ± 29.7 minutes versus 163.5 ± 27.7 minutes, P < .001). However, the other variables investigated such as intraoperative blood loss, duration of hospital stay, and postoperative VAS score did not show statistically significant difference between the groups.
BMI, body mass index.
Values were presented as mean ± standard deviation.
BSO, bilateral salpingo-oophorectomy; PLND, pelvic lymph node dissection; PPLND, pelvic and para-aortic lymph node dissection; TLH, total laparoscopic hysterectomy; VAS, visual analog scale.
Conversion to laparotomy was needed in 1 patient in the advanced bipolar group due to left renal vein damage, in which it was joining the vena cava just below the inferior mesenteric artery origin. It was repaired and patency was provided. There were no other perioperative complications, including urinary, intestinal, vascular, or trocar insertion related events.
Discussion
This is the first randomized study that compared LigaSure (advanced bipolar) and Robi forceps (conventional bipolar) in laparoscopic uterine cancer surgery. As the primary endpoint of the study, operation time was shorter in the advanced bipolar group as it was expected; results of this study showed that advanced and conventional bipolar groups were comparable for other perioperative outcomes.
In two previous studies, which were conducted in uterine cancers with different types of advanced energies rather than LigaSure, a significant improvement of operation time was also reported by advanced energy modalities.9,10 One of the main time consuming factors during the operation is to change instruments used to seal and cut. However, we can do both by using advanced bipolar instruments with no need to change the instrument. Shortening of operation time had not provided favorable perioperative clinical outcomes for the advanced bipolar group in this study. On the other hand, the advanced bipolar instrument is a single-use energy source and more expensive per case compared to conventional reusable energy sources. However, shortening of operation time could justify single-use device's own cost 13 in hospitals that operation room fee is applied and it reduced cumulative operation cost in the advanced bipolar group. 13
In studies including patients with uterine cancer, significantly lower blood loss was reported by advanced bipolar energy when compared to the conventional bipolar forceps utilization.9,10 There were no differences between the groups regarding operative blood loss measures in our study. Hemostasis could be achieved effectively with both instruments.
There were no major complications except conversion to laparotomy in 1 case due to left renal vein injury. Intraoperative complication rates were also reported very low in two previous studies including patients with uterine cancers, regardless of type of instruments.9,10 There is a concern about thermal spread during activation of energy-based instruments. Conventional instruments' tips are not covered like advanced instruments and lateral spread may be more than advanced instruments. Heating degree of advanced instruments' tips was also compared and it was found that ultrasonic instruments have a higher lateral heat flash than LigaSure. 14 It can be considered that 5 mm lateral margin may be safe for all devices. 10 Keeping away the ureter, bladder, major vessels, and intestines from energy-based instruments by traction may lower thermal complications of adjacent tissues. Increasing experience in using instruments and in gynecologic oncology surgery may be other factors that underlie very low complication rate.
Length of hospital stay was similar and short in both groups. Previous studies have also shown similar outcomes for duration of hospital stay.4,10,12 Significantly lower pain scores were shown at the 8th postoperative hour in the advanced bipolar group in a study conducted in patients with gynecologic cancers; 10 however, pain scores became similar at the 24th postoperative hour. We did not find a difference in postoperative pain scores. We speculate that length of hospital stay and postoperative pain may be affected primarily from minimally invasive approach and it may be the main determiner rather than type of using bipolar instrument.
Surgeons' thoughts for LigaSure and Robi forceps were evaluated subjectively and there was no difference between both energy modalities. 5 Evaluations were in favor of LigaSure in one center, but all measures were in favor of Robi forceps in other two centers. 5 We think that advanced bipolar instruments may provide fluency and lesser anxiety about thermal complication while operating, especially for inexperienced surgeons and fellows during their training. Further studies with subjective evaluation of the surgeons are needed.
The strengths of our study were prospective randomized design, adequate power, and performing study in uterine cancer surgeries, but there were some limitations. The major limitation was no evaluation of satisfaction and comfort of the surgeon according to the type of bipolar instrument. In addition, shortened operation times could effect the operation room fee. While the operation room fee is not applied in our center, we were not able to make such a calculation.
In conclusion, advanced and conventional bipolar energy instruments both have comparable perioperative outcomes, except operation time, which is shorter in the advanced bipolar group. Both instruments are safe in terms of complication.
Footnotes
Acknowledgment
This research has been supported by Ankara University Scientific Research Projects Coordination Unit (Project No.: 15A0230007, 2015).
Disclosure Statement
No competing financial interests exist.