
Abstract
Abstract
Introduction:
To study the anatomical features and classification of the angle between the right gastroepiploic vein (RGEV) and superior mesenteric vein/portal vein (SMV/PV) and to guide the catheterization of intraportal infusion chemotherapy through RGEV and reduce surgical complications.
Patients and Methods:
A retrospective three-dimensional (3D) computed tomography study was undertaken on 200 consecutive subjects with or without hepatic malignant tumors with a dedicated workstation 3D-MIA (the improved MI-3DVS workstation) developed by ourselves to determine the prevalence of surgically significant angle between RGEV and SMV/PV anatomic variations and its classification.
Results:
The mean value of the angles between the end of RGEV and SMV/PV (AERS/P) (200 cases) was 84.2° ± 23.8 (31.4°–151.5°): 40.6° ± 92.3 (−177.9° to 178.0°) (sagittal angle), 81.7° ± 29.8 (−79.3° to 160.7°) (coronal angle), and 10.5° ± 94.3 (−178.7° to 175.8°) (horizontal angle). The mean value of the angles between the right bend of RGEV and SMV/PV (ARRS/P) (168 cases) was 104.8° ± 26.1 (20.5°–159.7°):49.3° ± 117.8 (−175.3° to 179.5°) (sagittal angle), 103.5° ± 37.7 (−178.8° to 168.9°) (coronal angle), and 12.6° ± 102.8 (−179.9° to 179.2°) (horizontal angle). The AERS/P were classified into large angle group (32 cases, 16%), middle angle group (113 cases, 56.5%), and small angle group (55 cases, 27.5%) based on angle variations and risks of catheterization.
Conclusions:
Precognition of the variations of AERS/P and ARRS/P before surgery is useful during chemotherapy pump catheterizing through RGEV in reduction of surgical complications by modulating the angle and direction of RGEV running into SMV/PV properly.
Introduction
R
Patients and Methods
This retrospective study was performed on 200 consecutive adults (51 women, 149 men; age range 18–80 years, mean 52 years) between 2014 and 2015 who were found to have a “normal” RGEV on CT scans with or without malignant hepatic tumors. The CT scans were done with a 64-row or 256-row multidetector CT scanner (Philips Brilliance 64; Philips Healthcare, Best, The Netherlands) and images with thickness of 1 mm were acquired.
The end of RGEV was defined as 1 to 3 cm from the bottom of RGEV, and the right bend of RGEV was defined as the rightmost curve of RGEV.
The CT images were transferred to, and analyzed with, a dedicated workstation 3D-MIA originally developed by us, to create 3D models of PV and its tributary structures.
The angles between the end of RGEV or the right bend of RGEV and SMV/PV (AERS/P [Fig. 1], ARRS/P [Fig. 2]) were measured. The projection of an angle in sagittal, coronal, and horizontal view was sagittal angle, coronal angle, and horizontal angle, respectively, which were defined as from the bottom up and forward (Fig. 1B), from the bottom up and right (Fig. 1C), and from the back forward and right (Fig. 1D) into a corner.
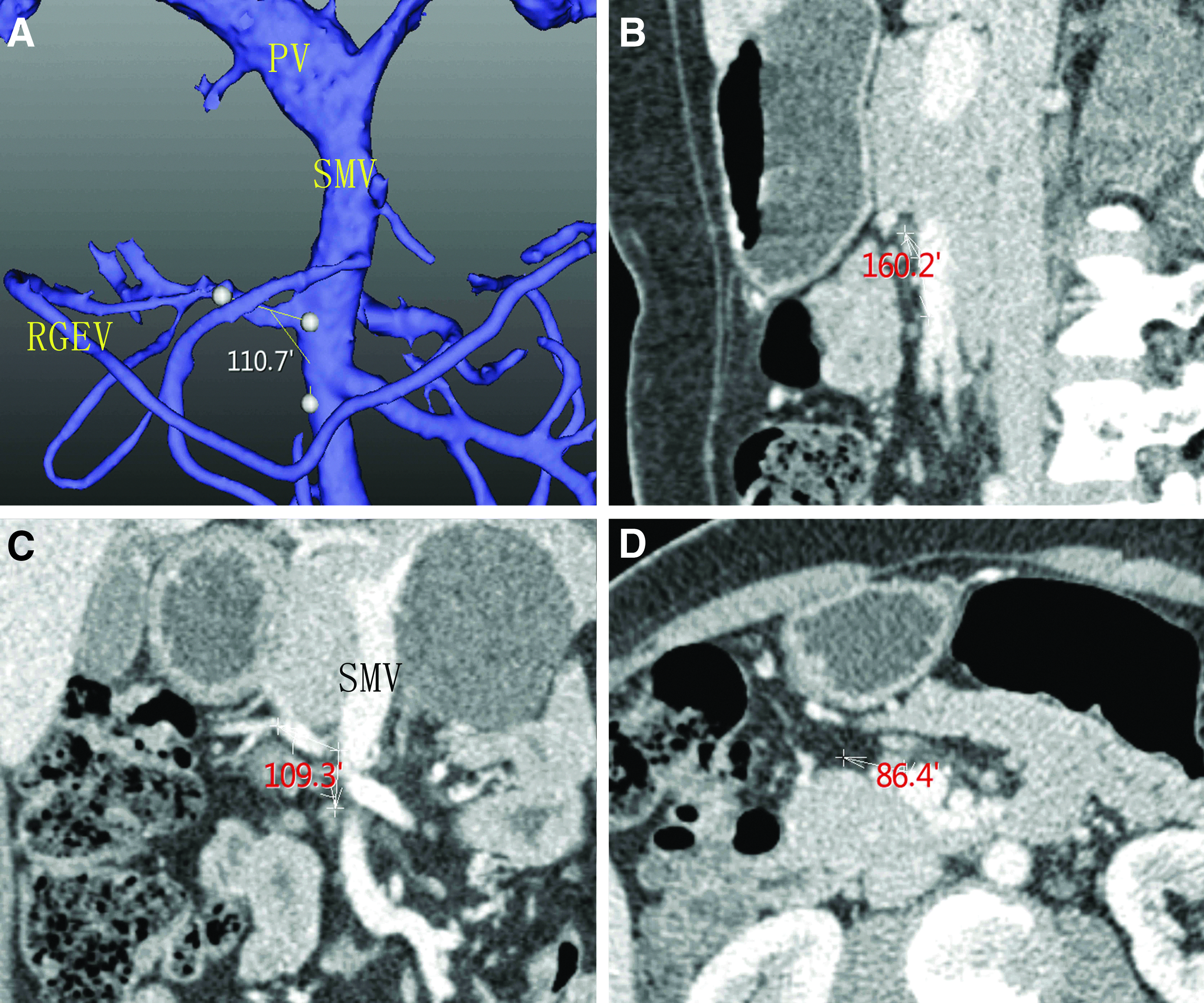
AERS/P of patient A are 110.7°
Exclusion criteria include the following: (1) age <18 years, (2) intra-abdominal tumors that change the shape of portal venous system, (3) abdominal infection, (4) intra-abdominal or cardiac diseases that impair venous return.
Statistical analysis
Continuous variables were expressed as a mean ± SD using SPSS13.0.
Results
The mean angle between the end of RGEV or the right bend of RGEV and SMV/PV are shown in Tables 1 and 2, and in Figures 1 and 2, respectively.
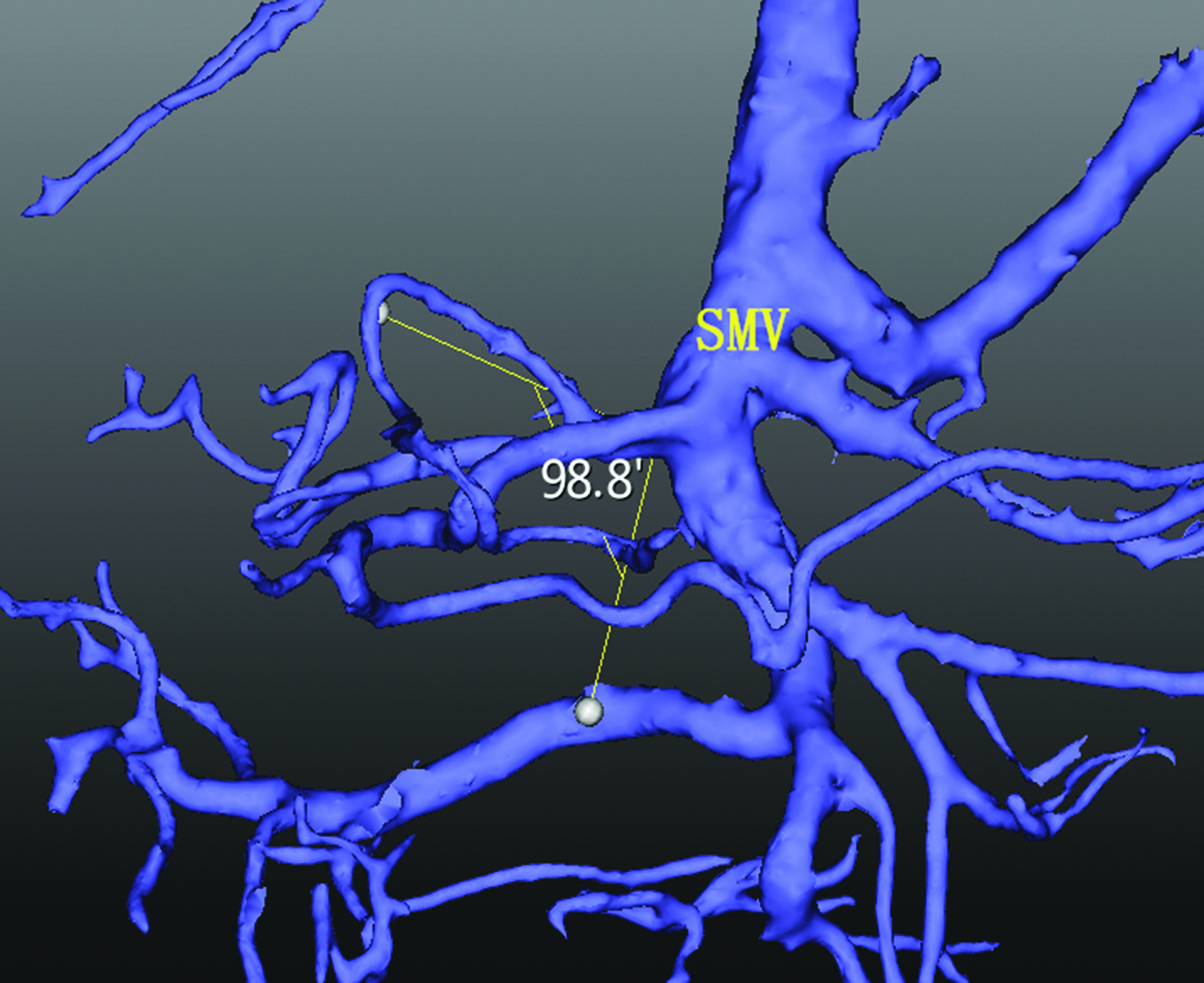
ARRS/P of patient C are 98.8° (sagittal, coronal, and horizontal angles are 43.9°, 98.3°, and −177.6°, respectively); ARRS/P, angles between the right bend of RGEV and SMV/PV.
AERS/P, angles between the end of RGEV and SMV/PV. RGEV, right gastroepiploic vein; SMV/PV, superior mesenteric vein/portal vein.
ARRS/P, angles between the right bend of RGEV and SMV/PV.
The AERS/P were classified into large angle group, middle angle group, and small angle group based on angle variations and risks of mechanical complications of catheterization.
Large angle group: both the sagittal angle and the coronal angle are between 75°and 105°, or between −105° and −75°, which is shown in Figure 5. There were 32 cases (16%) in total, whereas the sagittal angles satisfying large angle had 42 cases and the coronal angles satisfying large angle had 107 cases.
Middle angle group: exclusion of other two conditions, which is shown in Figure 1. There were 113 cases (56.5%) in total.
Small angle group: at least one of the sagittal angle or coronal angle is between −30° and 30°, which is shown in Figures 3 and 4. There were 55 cases (27.5%) in total, whereas the sagittal angles satisfying this criteria had 53 cases and the coronal angles satisfying this criterion had only 5 cases. One angle satisfies large angle and the other one satisfies middle or small angle in 14 cases (7%), of which coronal angle meets large angle criterion in 13 cases.

AERS/P of patient B are 62.5°(sagittal, coronal, and horizontal angles are 29.2°, 62.0°, and 15.7°, respectively) that belong to small angle group; AERS/P, angles between the end of RGEV and SMV/PV.

The end of RGEV of patient D runs from right to left, and then enters SMV at right ahead of SMV; AERS/P are 82.6° (sagittal, coronal, and horizontal angles are −22.9°, 82.3°, and −79.3°, respectively) and contained in small angle group, but still generates a bend when catheter enters SMV; AERS/P, angles between the end of RGEV and SMV/PV.
Discussion
The AERS/P and ARRS/P often determine whether chemotherapy pump through RGEV is catheterized smoothly or not. Our study found that the mean sagittal angle of AERS/P is close to 45°, the coronal angle is close to 90°, and the horizontal angle is 0°, whereas the horizontal angle has no effect on catheterizing. The other two angles are large so that catheterization could encounter resistance when the tube goes into SMV/PV with the risk of blood vessel injury and SMV/PV thrombosis. The mean value of ARRS/P is similar to that of AERS/P. Because of the larger angle value of the right curve, resistance and blood vessel injury could arise. Theoretically, the large angle group easily encounters resistance and most attempt with the largest rate of mechanical complications; the complications of middle angle group are not less, and still need caution and prevention. Lastly, in the small angle group, the end of RGEV is nearly parallel to SMV/PV with little complication so there is no need to modulate the direction in which RGEV flows into SMV/PV.
In the small angle group (55 cases, 27.5%), there are 13 cases (6.5%) whose coronal angle reaches the standard of large angle and its sagittal angle satisfies that of the small angle. In this condition, RGEV runs from right to left and then rotates to nearly right ahead of SMV and runs into SMV/PV in a small angle sequentially. Because of this condition, catheterization still needs caution and correction especially when encountering resistance (Fig. 4).
The complications of chemotherapy pump catheterizing through RGEV include catheter occlusion, blood vessels injury, hemorrhage, SMV/PV thrombosis, liver failure, congestion and ischemia of intestine.3,7–9 Treatments of the mentioned complications are unsatisfactory. The optional methods consist of phlebotomy and embolectomy, thrombolysis by intervention or intravenous drugs, and vascular patch or reconstruction. 10
Precognition of individual anatomy ahead of operation and effective surgical procedure to prevent complications during operation are the most important. Our research of the angles between RGEV and SMV/PV is based on 3D models made from preoperative CT images. No doubt it is one of the effective and feasible methods; we came up with a surgical maneuver to modulate the angle between RGEV and SMV/PV for the patients belonging to large or middle angle group: lift the right bend of RGEV with a wide range of motion forward and a little to the right after the catheter reaches the right bend to reduce the bend angle (the black bending arrow shown in Fig. 5); push the end of RGEV a little upward with operator's right thumb, then push the SMV/PV at the opposite position of the right thumb upward with the right forefinger after the catheter reaches SMV/PV (the red arrow in Fig. 5), thereby reducing the angle and decreasing the rate of complications. However, the effectiveness of this maneuver needs further study.

AERS/P of patient E are 88.7°(sagittal, coronal, and horizontal angle are −101.2°, 86.8°, and −68°, respectively) that belongs to large angle group; AERS/P, angles between the end of RGEV and SMV/PV.
According to the literature, there were 71.7% of RGEV combined with right or middle colic vein before entering SMV, and only 28.3% RGEV entered SMV directly 11 . So catheterization in operation through middle colic vein may also encounter the same vessel injury as that through RGEV when middle colic vein is combined with RGEV in some patients. In these conditions, operators should still make the angle between middle colic vein or RGEV and SMV clear before operation, and modulate the direction of catheter using the former maneuver proposed if necessary.
Ethics statement
This retrospective study was approved by the Ethics Committee of the Zhujiang Hospital, Southern Medical University (No. 2012-GDYK-001). Patients did not need informed consent forms.
Footnotes
Acknowledgment
This study was supported by the Natural Science Foundation of Guangdong Province (2014A030310393).
Disclosure Statement
No competing financial interests exist.