
Abstract
Abstract
Background:
The Soave pull-through for Hirschsprung's disease leaves a muscular cuff of aganglionosis surrounding the pull-through. In some patients, this cuff can extrinsically compress the pull-through, leading to chronic enterocolitis and failure to thrive. We describe a novel technique for managing the Soave cuff as an alternative to a complete redo pull-through.
Procedure:
A laparoscopic excision of the intraperitoneal portion of the Soave cuff is performed, taking care to avoid injury to bladder, vas deferens, or vagina. The extraperitoneal portion of the cuff, adjacent to the bladder/vagina, is left in place. The excision is tailored to eliminate the obstruction and minimize injury to surrounding structures. Diverting colostomy is not necessary and patients are discharged the next day.
Results:
Three patients successfully underwent excision without any operative complications and without the need for a colostomy. They had resolution of their chronic enterocolitis.
Conclusion:
In patients with an obstructing Soave cuff, a laparoscopic excision should be considered as a surgical option. We found that the procedure can be effective, with little morbidity.
Introduction
H
Methods
Surgical preparation
As described in Dickie et al.,1,2 patients with HD presenting with obstructive symptoms, such as distention, constipation, emesis, and failure to thrive, are investigated for possible surgical causes. A contrast enema helps to rule out a megacolon, twist of the pull-through, and extrinsic compression secondary to a Soave cuff. Extrinsic compression of the pull-through with poor evacuation of contrast is pathognomonic for a Soave cuff obstruction. 1 An examination under anesthesia with a full thickness rectal biopsy allows assessment of the anus to rule out an anastomotic stricture, and confirms that the pull-through has normal ganglionated bowel. If the only finding during the workup is extrinsic compression of the pull-through by a Soave cuff (Fig. 1), we offer a laparoscopic excision. In all cases, the patient is consented for a complete redo pull-through, in case an excision of the cuff is not feasible.
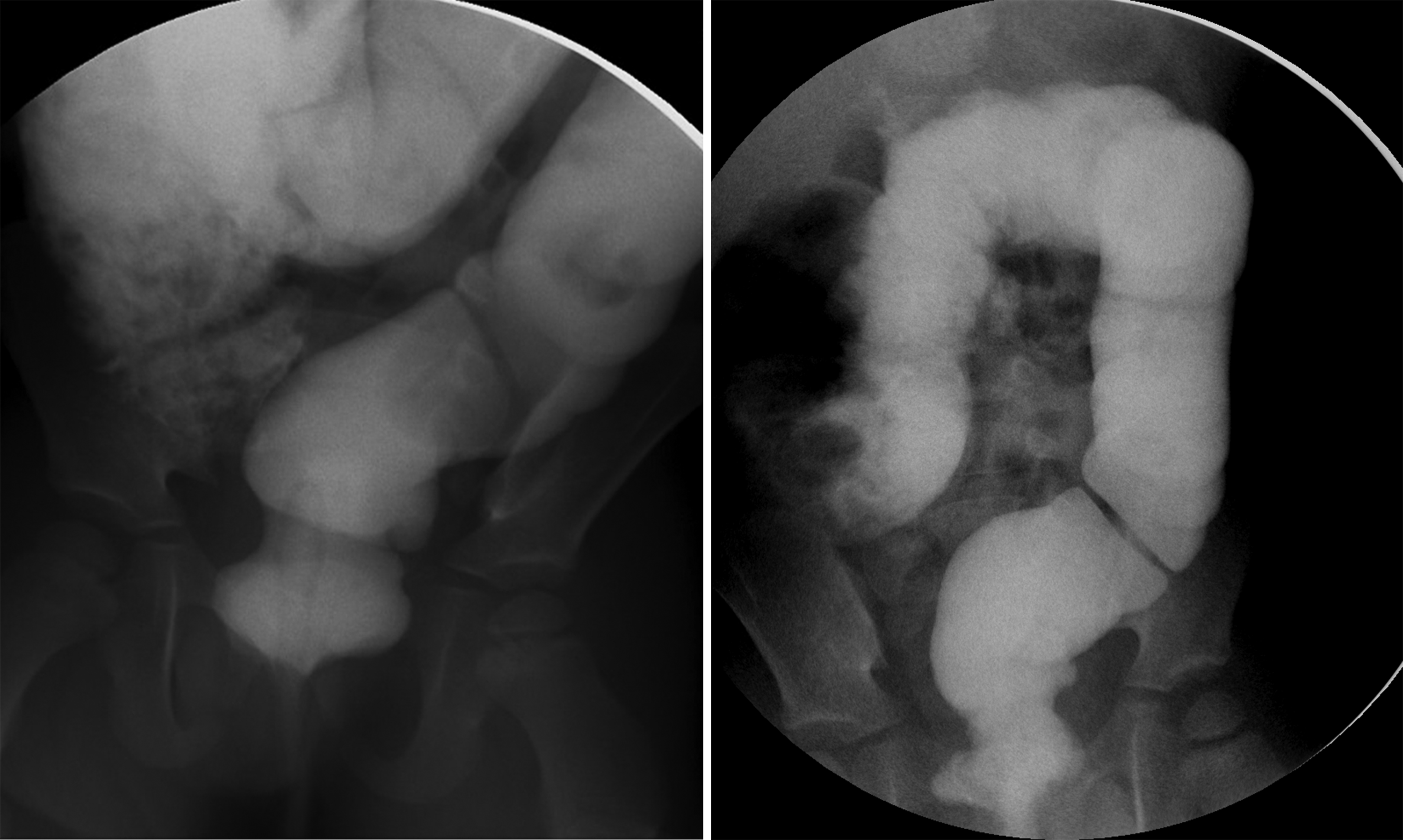
Contrast studies from 2 patients showing apple core-like lesions that suggests extrinsic compression. In a patient who has undergone a procedure, this is likely an obstructing Soave cuff.
Operative technique
After induction of general anesthesia, the rectum is washed out to remove any bulky stool. A catheter is placed to decompress the bladder. The patient is placed in lithotomy and the abdomen is prepped, including the perineum. This allows access to the rectum, if necessary.
Typically, three 5 mm ports are used (umbilical, right, and left lateral abdomen), with the option for a fourth if needed. The patient is placed in Trendelenburg and the pelvis is inspected. The pull-through is often distended and thickened from the chronic enterocolitis. The cuff is typically rolled down and found at the interface between the bladder/vagina and the dilated pull-through (Fig. 2).
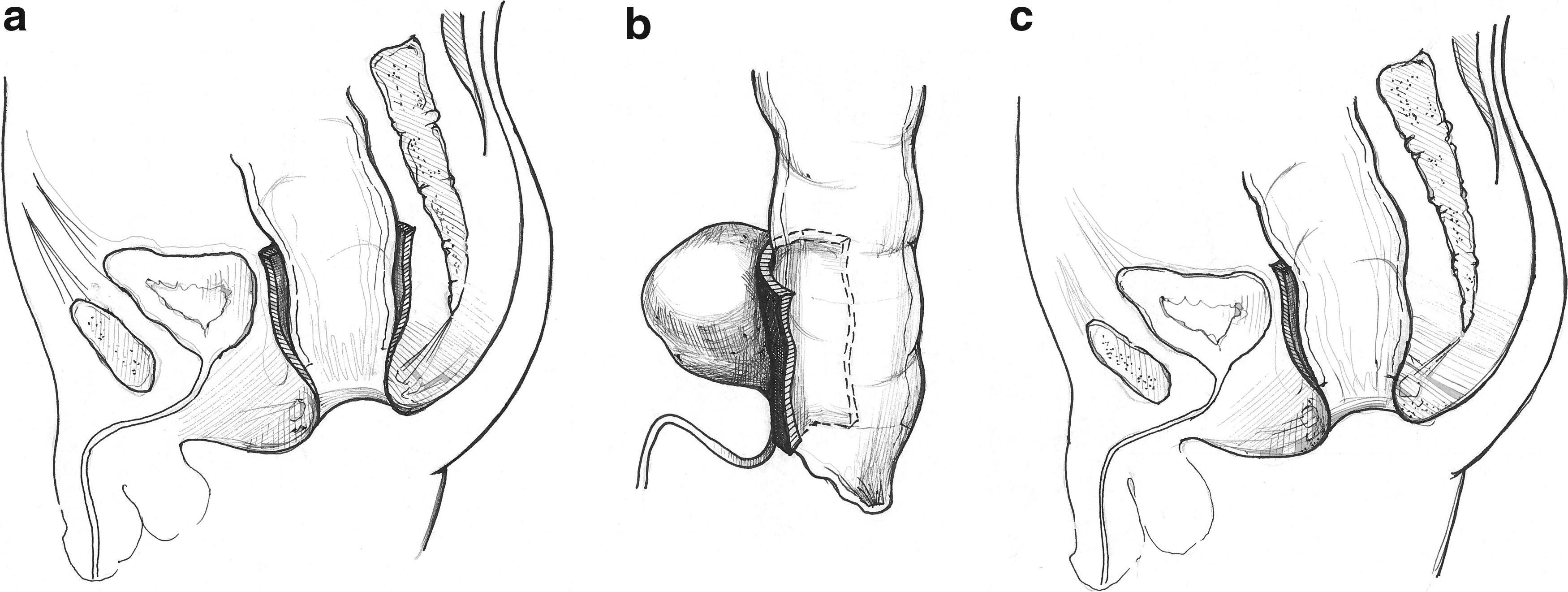
Illustration demonstrating the Soave cuff before
The cuff is unrolled and the plane between the Soave cuff and the pull-through is dissected. In general, there are minimal adhesions between the cuff and the pull-through, which may explain why the cuff can roll down and obstruct the pull-through. The ureters are identified, as are the vas deferens in males and the gynecologic structures in females. The right lateral edge of the cuff is unrolled and followed down to the base of the pelvis. Using a sealing device, the intraperitoneal portion of the cuff is excised from lateral to medial, taking care to protect the ureter. The extraperitoneal plane between the cuff and the bladder/vagina is not dissected to minimize potential injury to the bladder/vagina and nerves of sexual function (Fig. 3). The dissection continues from the right side to the left, excising the intraperitoneal portion of the cuff only. The left side is more challenging and often requires mobilizing the pull-through from the lateral pelvic wall. This helps to identify the left ureter and the left Soave cuff safely.
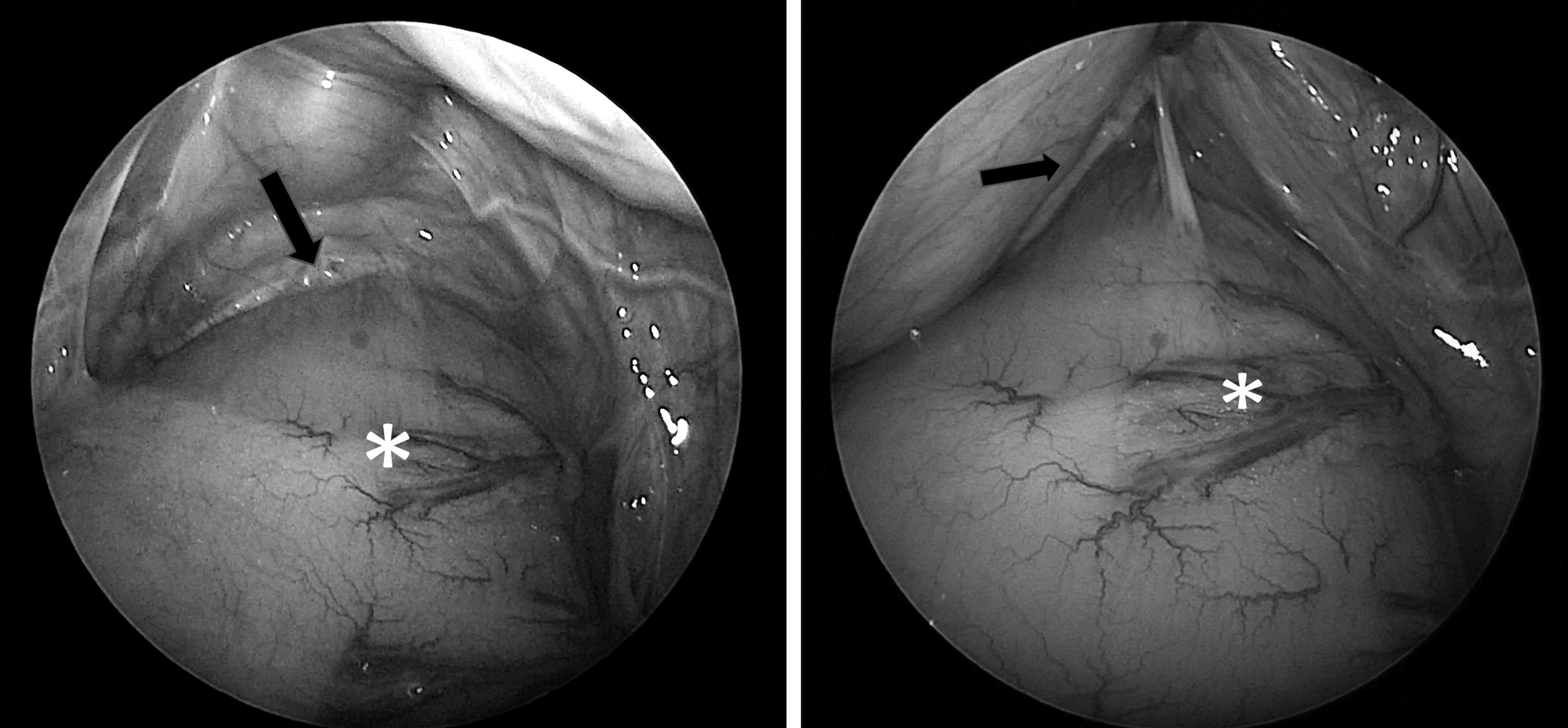
Images from the dissection of the Soave cuff. Note the dilated pull-through (*) and the vas deferens. The Soave cuff (black arrow) is found at the interface of the pull-through and the base of the bladder, often rolled down. Adhesions are usually minimal and can be managed with blunt dissection.
Once the cuff is excised, the pull-through is inspected for any injury and then the laparoscopic incisions are closed. Typically, the diet is advanced immediately and the patient is observed overnight.
Results
Case 1
EA is a 4-year-old male with HD, who presented to our clinic with recurrent enterocolitis, including episodes of distention, obstipation, and anorexia, since he was 1 month of age. He was managed with irrigations and Flagyl. Despite undergoing dilations and two myomectomies, he continued to suffer with obstructive symptoms. He could not stool on his own, emptying only with irrigations. A contrast study showed an obstructing Soave cuff, with extrinsic compression of the rectum and failure to empty the contrast on his own. No other causes for obstruction was found in the course of the workup. As he had already undergone a myomectomy, a laparoscopic-assisted redo pull-through was recommended. During the laparoscopic exploration, the cuff was found to be free and not adherent to the pull-through, and so an excision of the cuff was performed. Postoperatively, he was weaned off irrigations quickly and has thrived, stooling with a bowel regimen. A follow-up contrast study showed a resolution of the extrinsic compression (Fig. 4). He has had no enterocolitis for >3 years.

Contrast study postlaparoscopic excision of the Soave cuff. The extrinsic compression seen previously is resolved.
Case 2
MR is a 4-year-old female who had undergone Soave procedure at birth, and had a previous myomectomy at age 2 for chronic enterocolitis. She presented with chronic distention, emesis, and obstipation with dilated colonic loops on X-ray examination. These symptoms were relieved with irrigations and metronidazole. Over the course of a year, she could not be weaned from the irrigations without recurrent symptoms. A contrast study showed an extrinsic compression of the pull-through, suggesting an obstructing Soave cuff. The complete workup found no other abnormalities. The patient then underwent a laparoscopic Soave cuff excision without any complications. She recovered well from the surgery and was discharged the next day.
Over the next 2 years, she has had a single episode of enterocolitis that resolved with a short course of irrigations and metronidazole. She is currently free of enterocolitis and is on a bowel regimen to manage constipation.
Case 3
KF is a 6-year-old male who presented 3 years after he underwent botox injections of his anal canal and then a posterior myomectomy—all to manage his obstructive symptoms. He presented to our clinic with distention and severe constipation, with significant straining and stools that were pencil thin. His contrast study suggested extrinsic compression. As he did not have symptoms of enterocolitis, an aggressive bowel regimen was started, but provided no relief. He continued to have pencil-thin stools, with significant straining. After a frank discussion with his parents, he underwent laparoscopic excision of Soave cuff. He had no surgical complications and has had no issues in the 2 years after his surgery.
Discussion
HD is a surgical disease that requires the resection of the involved aganglionic bowel. The Soave procedure, or endorectal dissection, was designed to prevent injury to structures surrounding the anterior rectal wall, especially the nerves of sexual function. However, this technique leaves behind an aganglionic muscular cuff that can extrinsically obstruct the pull-through. It appears that longer cuffs are more likely to lead to an obstructive pattern, and as a result, some surgeons recommend a 1–2 cm cuff.1,3 Patients with an obstructing Soave cuff present with chronic constipation, recurrent enterocolitis, and failure to thrive.1,2
Indications for a redo pull-through procedure include obstructive symptoms secondary to a stricture, persistent aganglionosis, an obstructing cuff, and a twisted pull-through.2,4–6 As described by Dickie et al., we perform a full workup in patients presenting with obstructive symptoms, including a contrast enema, an examination under anesthesia, and a rectal biopsy. 1 We find that the contrast enema is the best test to identify the extrinsic compression secondary to a Soave cuff, especially if the patient struggles to evacuate the contrast afterward. The typical finding is an apple core lesion in the distal rectum (Fig. 1).
Once an obstructing Soave cuff is identified, surgical options are required. There are no medical treatments that have been shown to overcome this problem and symptomatic management such as laxatives, rectal irrigations, or behavioral modification is temporizing at best.5,6 Surgical options include botox, myomectomy, or a redo pull-through. Botox has been used to treat internal anal sphincter achalasia. 7 Koivusalo et al. found that botulinum toxin can improve symptoms of enterocolitis, however, fecal incontinence persisted. 8 Evidence of long-term improvement is lacking, especially in patients with an obstructing Soave cuff. 8 Our last patient had had botox without improvement, before being diagnosed with an obstructing Soave cuff. It is unclear how botox injection in the anal canal would have a lasting effect on the Soave cuff, which is located high above the anal canal. As a result, we do not offer botox for an obstructing Soave cuff.
There have been a number of descriptions of myomectomies, which involve excision of a strip of the rectal wall posteriorly, including the Soave cuff. This is typically performed through a transanal approach.9,10 Although less invasive than a redo pull-through, it is difficult to dissect high above the anal canal. 10 Complications can include a leak, fistula, or incontinence.10,11 Wildhaber et al. found that myomectomies in patients without aganglionosis had good results, but they did not identify any patients with an obstructing Soave cuff. 10 A posterior sagittal myomectomy has been previously described, which has the benefit of leaving the pull-through intact and undisturbed. 11 All 3 of our cases had undergone one or more transanal myomectomies because of their obstructive symptoms and had, at most, temporary success. This would suggest that a myomectomy is an incomplete solution for these patients. As a result, we do not offer a myomectomy if an obstructing Soave cuff is identified on contrast study.
A redo pull-through procedure is the most definitive treatment, as it excises the problematic cuff and addresses the anatomical and functional problems.1,4–6,12 However, a redo pull-through procedure is complicated and has significant risk, including anastomotic stricture, dehiscence, and pelvic abscess. It often requires a laparotomy and a diverting colostomy to protect the new coloanal anastomosis.1,4–6,12 Both Duhamel, Soave, and Swenson redo pull-throughs have been described.1,4–6,13 In the patient with persistent aganglionosis, or a twisted pull-through, a transanal redo pull-through, with or without laparotomy, is the ideal operation to manage these issues.
In our cases, the pull-through bowel was normal, without residual aganglionosis, twists, nor stricture. To avoid the risks of a redo pull-through, we attempted a laparoscopic excision of the cuff. With this technique, only the intraperitoneal portion of the cuff is excised, which minimizes injury to the bladder or vagina, and the nerves of sexual function. We hypothesize that the extraperitoneal portion of the rectum does not contribute to the extrinsic compression, as the natural attachments fix the rectum to the bladder or vagina, keeping the cuff from folding down and compressing the pull-through. It appears that a longer cuff predisposes to an obstructing cuff, and several surgeons, therefore, advocate for a shorter cuff (1–2 cm) to prevent this complication.1,3 In our case series, the cuff was long and intraperitoneal, making a laparoscopic approach reasonable. These patients required no diverting colostomy, could resume a regular diet immediately, and be discharged the next morning. Dickie et al. argue that with a redo pull-through, excising the thickened pull-through is theoretically advantageous as the pull-through may be dysmotile. They do not elaborate on how many patients require laxatives post redo pull-through. 1 In our series, laxatives have been sufficient to keep our patients stooling and symptom-free without excising the pull-through.
Mobilizing an adherent cuff off of the pull-through is the greatest risk with this procedure. Langer et al. recommend the Duhamel approach when performing a redo, because of concerns regarding the adhesions between the cuff and ganglionic bowel. 6 That being said, successful redo Soave pull-throughs have been described, indicating that the adhesions between the cuff and the pull-through can be manageable. 13 Interestingly, we found that in all cases, the adhesions were relatively mild, and the cuff was rolled down. It is possible that mild adhesions allow the Soave cuff to roll down and obstruct the pull-through, whereas patients with significant adhesions do not develop the same extrinsic compression. This might explain why a long Soave cuff does not always develop obstructive symptoms. That being said, all 3 patients were consented for a possible laparoscopic-assisted redo pull-through, in event that the cuff excision was not feasible.
This procedure does require some laparoscopic experience to identify and preserve vital structures, and safely perform the excision. Ureters, vas deferens, and gynecologic structures need to be identified and safely protected. The dissection must be performed between the wall of the pull-through colon and the cuff to prevent injury to pelvic structures and anal sphincter injury. 13 Trendelenburg position helps tremendously and surgeons comfortable with laparoscopic-assisted pull-throughs should not struggle with this procedure.
In summary, patients with HD who present with chronic enterocolitis should be worked up for surgical causes, such as persistent aganglionosis, anastomotic stricture, or an obstructing Soave cuff. In patients with an obstructing cuff, we have found that a laparoscopic excision of the Soave cuff is a feasible alternative, well tolerated, and with no morbidity.
Footnotes
Acknowledgment
The authors thank Ashley Lee for the line drawings included in this article.
Disclosure Statement
No competing financial interests exist.