
Abstract
Abstract
Background:
A systematic analysis of the evidence regarding oncological, perioperative and postoperative outcomes of open nephroureterectomy (ONU), laparoscopic nephroureterectomy (LNU), and hand-assisted laparoscopic nephroureterectomy (HALNU) was designed.
Methods:
The summarized data were abstracted from 52 original research articles representing 19,195 patients. PubMed/Medline, Scopus, Google Scholar, EMBASE, and the Cochrane Library were reviewed in March 2017, following PRISMA framework. A total of 52 publications were selected for inclusion. The primary outcomes were 2- and 5-year cancer-specific survival (CSS) rate, overall survival (OS) rate, and recurrence-free survival (RFS) rate. The secondary outcomes were operative time, lengths of hospitalization period, estimated blood loss, transfusions, major Clavien complication rate, metastasis rate, bladder recurrence rate, and positive surgical margin.
Results:
On comparing LNU versus ONU and HALNU versus ONU, no significant differences between the 5-year CSS rate (P = .25, P = .39), OS rate (P = .06, P = .46), and RFS rate (P = .85, P = .73) were found. On comparing LNU versus ONU and HALNU versus ONU during a 2-year follow-up period, the following were found: CSS rate (P = .61, P = .04) and OS rate (P = .33, P = .19). There were no significant differences between the LNU versus ONU and HALNU versus ONU rates, regarding bladder recurrence (P = .12, P = .85) and metastasis rate (P = .07, P = .27). Significant higher operative time (P = .01, P = .0004), lower length of hospitalization period (P < .001, P < .001), and estimated blood loss (P = .0004, P < .001) were found in comparison to that of LNU versus ONU and HALNU versus ONU.
Conclusion:
Both LNU and HALNU had comparable oncological and better perioperative and postoperative outcomes, when compared with ONU.
Background
T
There is an ongoing debate concerning the real improvements for the minimally invasive surgeries over the open approach. In recent years, a number of studies have been published in an attempt to explore this issue.2–4 Nevertheless, the limitations, such as small sample size and single-center research, have prevented strong conclusions from being drawn. Therefore, this study conducted a systematic literature review and meta-analysis to determine the current position of ONU, hand-assisted laparoscopic nephroureterectomy (HALNU), and laparoscopic nephroureterectomy (LNU).
Methods
A systematic literature review was performed in March 2017 in multiple databases. The study design, search strategy, data abstraction, and excluded studies were determined using Preferred Reporting Items for Systematic Reviews and Meta-analyses criteria (www.prisma-statement.org) (Table 1 and Fig. 1). The items retrieved were restricted to publications in English.

Flowchart of study design and included studies.
CSS, cancer-specific survival; HALNU, hand-assisted laparoscopic nephroureterectomy; LNU, laparoscopic nephroureterectomy; ONU, open nephroureterectomy; OS, overall survival; QAS, quality assessments; RFS, recurrence-free survival.
Original research articles reporting on treatment of upper tract TCC were included. The reference lists of review/meta-analysis articles that included articles not already in our database were also reviewed.3,4 Conference abstracts were not included because they lacked detail and had not undergone rigorous peer review.
To assess the methodological quality of the studies included, they were initially reviewed by 2 independent reviewers using total quality assessment (QAS) (Table 2). Although the QASs were reported for each study, they were not used to weight the studies in the meta-analysis.
The same authors independently extracted the data, which were later jointly reviewed to reach agreement that the data were accurate. If disagreement existed, it was resolved by consensus or consultation with the senior authors. The data collected from all articles regarding treatment groups included the nephroureterectomy approach (open, laparoscopic, and hand-assisted laparoscopic), type of publication (retrospective, nonrandomized trial, or randomized trial), duration of follow-up, patient characteristics (number, age, and pathological stage; Table 3), management of the distal ureter (open, endoscopic, and LigaSure), management of lymph nodes, and total intraoperative and perioperative major Clavien complication rates 5 and other outcomes (mean operative time, length of hospital stay, estimated blood loss, blood transfusions, 2- and 5-year cancer-specific survival [CSS] rate, 2- and 5-year overall survival [OS] rate, 2- and 5-year recurrence-free survival [RFS] rate, bladder recurrence rate, metastasis rate, and positive surgical margin rate; Table 3).
CSS, cancer-specific survival; HALNU, hand-assisted laparoscopic nephroureterectomy; LNU, laparoscopic nephroureterectomy; N/D. not determined; ONU, open nephroureterectomy; OS, overall survival; RFS, recurrence-free survival.
The primary and secondary outcome measures were oncologic and perioperative outcomes, respectively. Two measurements on oncologic outcomes were evaluated. We looked at the 5-year RFS rate, 2- and 5-year CSS rates, 2- and 5-year OS rates, recurrence rate, bladder recurrence rate, and metastasis rate. Recurrence was defined as tumor relapse during the follow-up period.
Statistical methods
Review Manager version 5.2 (downloaded from http://community.cochrane.org/tools/review-production-tools/revman-5) was used to analyze the selected studies. Continuous data for each arm of a particular study were expressed as mean and standard deviation (SD). Dichotomous data were expressed as proportions or risks and the treatment effect was reported as odds ratios (OR) with a 95% confidence interval (95% CI). To use all data, if only median and range were reported in an article, the median was substituted for the mean when the sample size was greater than 25 and if the sample size was lower than 25, we used the following formula: a +2(m) + b/4 using the values of the median (m), low and high end of the range (a and b, respectively). The SD can be estimated using the formula as follows, which was discussed in previous study: a − b/4 (for moderately sized samples [15 < n ≤ 70]) or a − b/6 (for large samples [n > 70]).
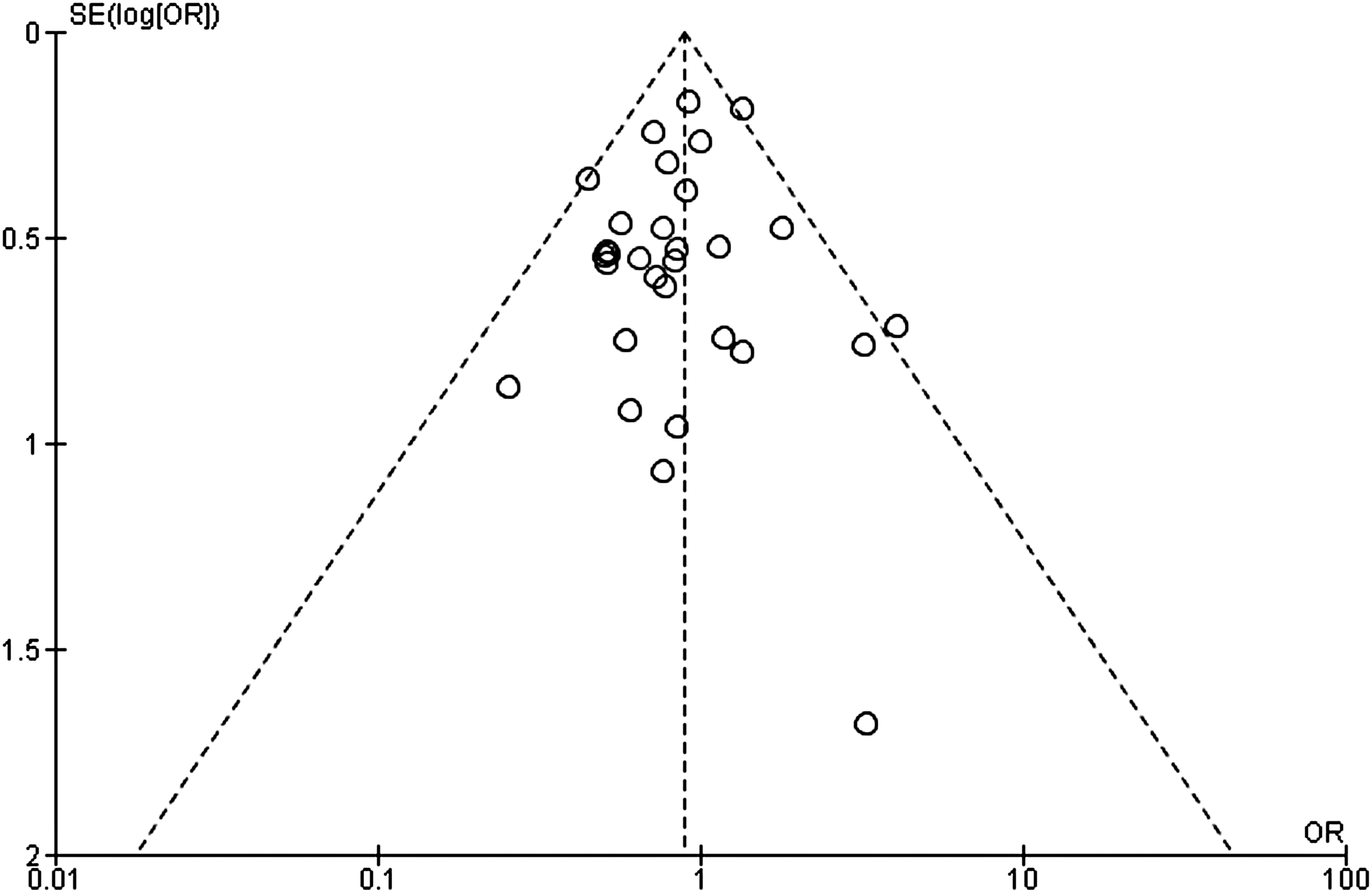
Heterogeneity between studies was assessed using the chi-squared test and I2 statistic. A P value <.1 and an I2 value >50% were considered suggestive of statistical heterogeneity, prompting a random effects modeling estimate. A nonsignificant chi-squared test result (P ≥ .1 and I2 ≤ 50%) suggested that there was no evidence of heterogeneity and a random-effect model was used. Funnel plots were constructed for the outcomes to assess publication bias, which is defined as the tendency not to publish studies with a negative result. The more asymmetric the funnel plot was, the higher the potential bias was. Statistical significance was set at P < .05.
Results
This systematic review and meta-analysis included 19,195 patients, 11,787 undergoing ONU, 7071 undergoing LNU, and 337 undergoing HALNU. Of the preoperative data, there were significant differences in pathological stages between studies (ONU: Ta, Tis 22.2%, T1 21.9%, T2 16.1%, T3 30.4%, T4 9.4%; LNU: Ta, Tis 28.7%, T1 28.4%, T2 16.0%, T3 25.3%, T4 1.6; and HALNU: Ta, Tis 9.7%%, T1 33.3%, T2 36.0%, T3 20.2%, T4 0.8%; P < .0001).
ONU versus LNU
Five-year CSS rate
There was significant heterogeneity between studies that compared ONU and LNU (I2 = 60%; P = .002); thus, random effects were used to analyze the outcome. There was no significant difference in CSS rate after 5 years between ONU and LNU (OR: 1.24; 95% CI: 0.86–1.79; P = .25; Fig. 2).
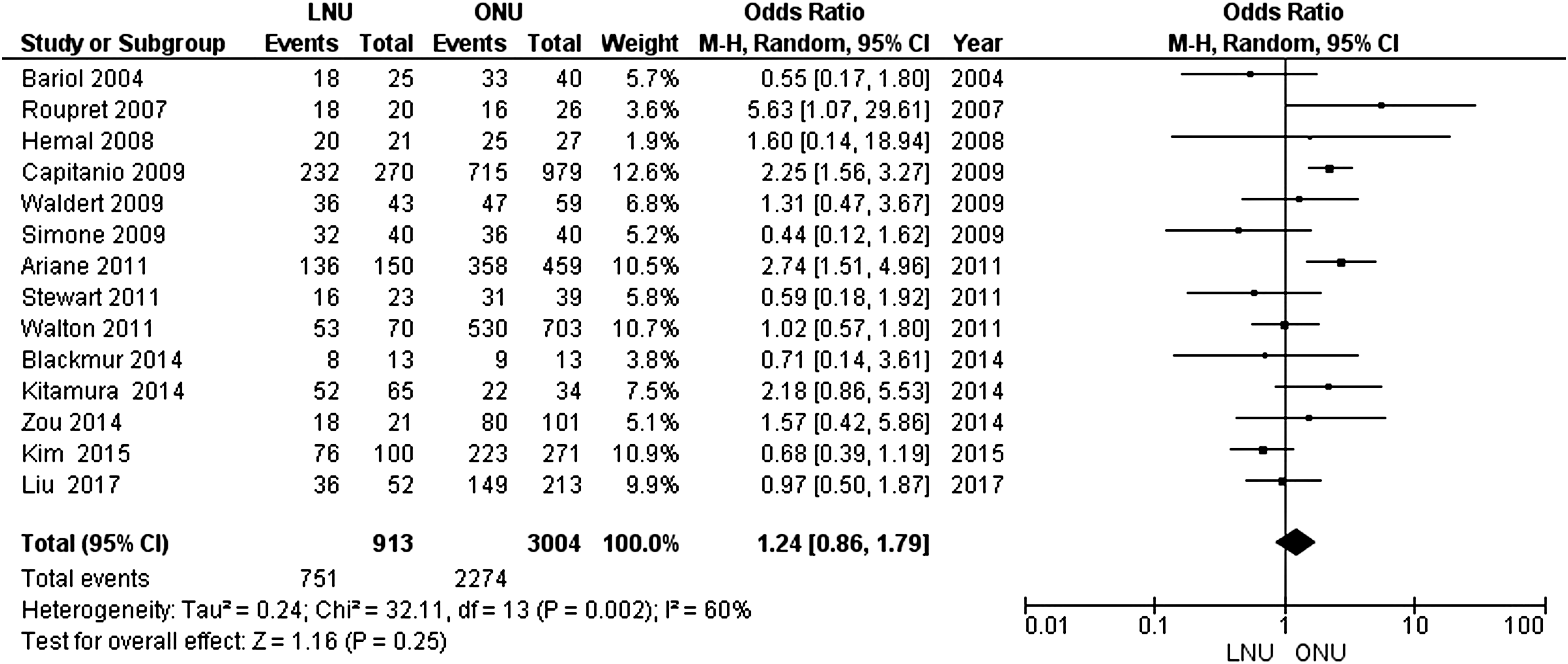
Analysis showed no significant difference in CSS rate after 5 years between ONU and LNU. CSS, cancer-specific survival; LNU, laparoscopic nephroureterectomy; ONU, open nephroureterectomy.
Five-year OS rate
No significant heterogeneity was detected between the studies in this outcome (I2 = 1%; P = .42); thus, fixed effects were used to analyze the outcome. There was no significant difference OS rate after 5 years between ONU and LNU (OR: 0.76; 95% CI: 0.57–1.02; P = .06; Fig. 3).
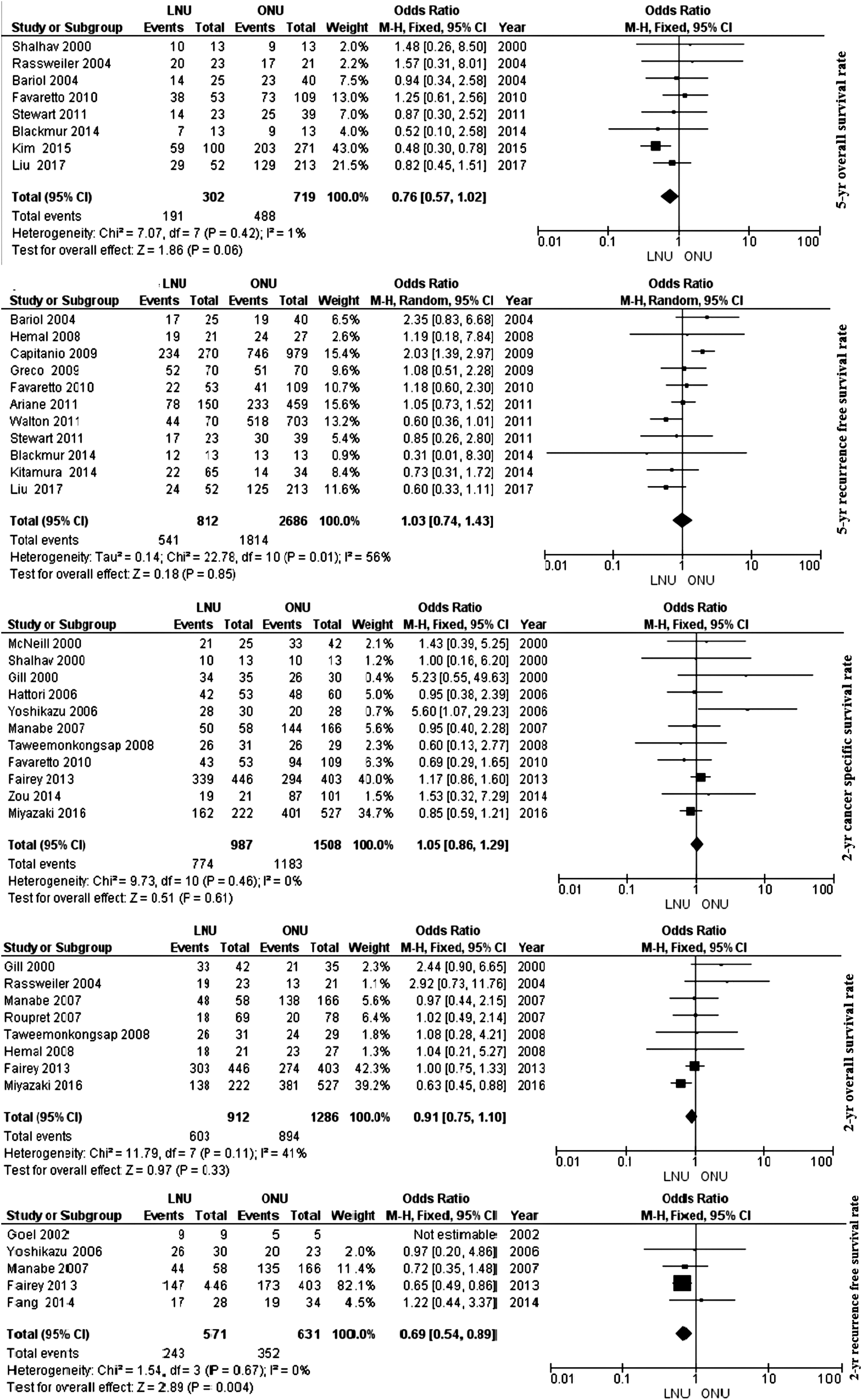
Analysis showed no significant difference overall, 5-year recurrence-free, 2-year cancer specific, 2-year overall, and 2-year RFS rate after 5 years between ONU and LNU. LNU, laparoscopic nephroureterectomy; ONU, open nephroureterectomy; RFS, recurrence-free survival.
Five-year RFS rate
There was significant heterogeneity between studies that compared ONU and LNU (I2 = 56%; P = .01); thus, random effects were used to analyze the outcome. There was no significant difference in RFS rate after 5 years between ONU and LNU (OR: 1.03; 95% CI: 0.74–1.43; P = .85; Fig. 3).
Two-year CSS rate
There was no significant heterogeneity between the studies in regard to this outcome (I2 = 0%; P = .46); thus, fixed effects were used to analyze the outcome. There was no significant difference in CSS rate after 2 years between ONU and LNU (OR: 1.05; 95% CI: 0.86–1.29; P = .61; Fig. 3).
Two-year OS rate
There was no significant heterogeneity between the studies in regard to this outcome (I2 = 41%; P = .11); thus, fixed effects were used to analyze the outcome. There was no significant difference in OS rate after 2 years between ONU and LNU (OR: 0.91; 95% CI: 0.75–1.10; P = .33; Fig. 3).
Two-year RFS rate
There was no significant heterogeneity between studies that compared ONU and LNU (I2 = 0%; P = .67); thus, fixed effects were used to analyze the outcome. There was a significantly higher RFS rate after 2 years in ONU compared with LNU (OR: 0.69; 95% CI: 0.54–0.89; P = .004; Fig. 3).
Bladder recurrence rate
There was no significant heterogeneity between the studies in regard to this outcome (I2 = 0%; P = .49, Fig. 4); with fixed effects analysis, there was no significant difference in intravesical recurrence between ONU and LNU (OR: 0.89; 95% CI: 0.77–1.03; P = .12; Fig. 5).
Analysis showed heterogeneity between studies in whom intravesical recurrence was compared between ONU and LNU. LNU, laparoscopic nephroureterectomy; ONU, open nephroureterectomy.
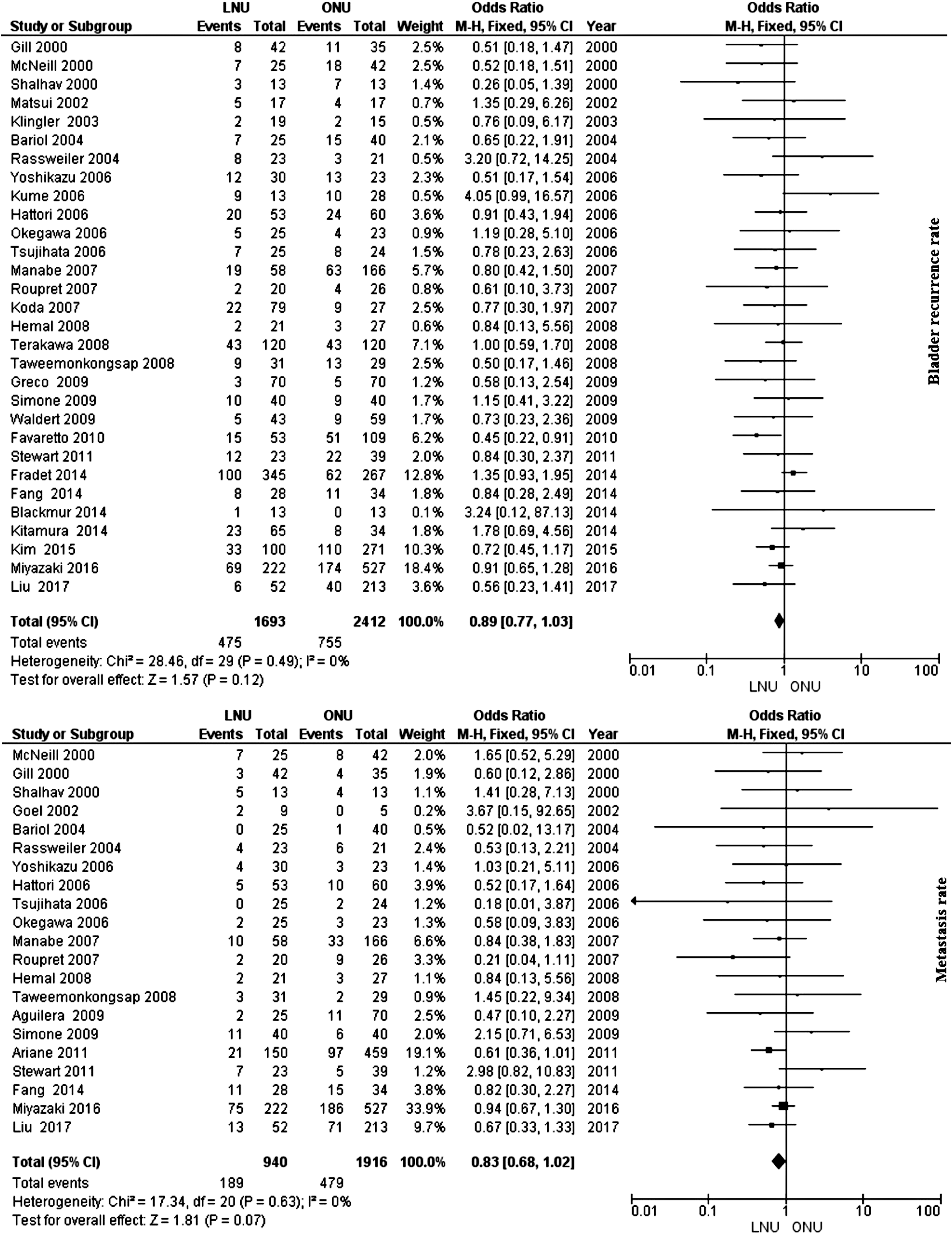
Analysis showed no significant difference in metastasis rate between ONU and LNU. LNU, laparoscopic nephroureterectomy; ONU, open nephroureterectomy.
Metastasis rate
There was no significant heterogeneity between the studies in regard to this outcome (I2 = 0%; P = .63); with fixed effects analysis, there was no significant difference in metastasis rate between ONU and LNU (OR: 0.83; 95% CI: 0.68–1.02; P = .07; Fig. 5).
Major Clavien complication rate
There was no significant heterogeneity between studies that compared ONU and LNU (I2 = 0%; P = .25); thus, fixed effects were used to analyze the outcome. There was no significant difference in major Clavien complication rate between ONU and LNU (OR: 0.95; 95% CI: 0.57–1.59; P = .86; Fig. 6).
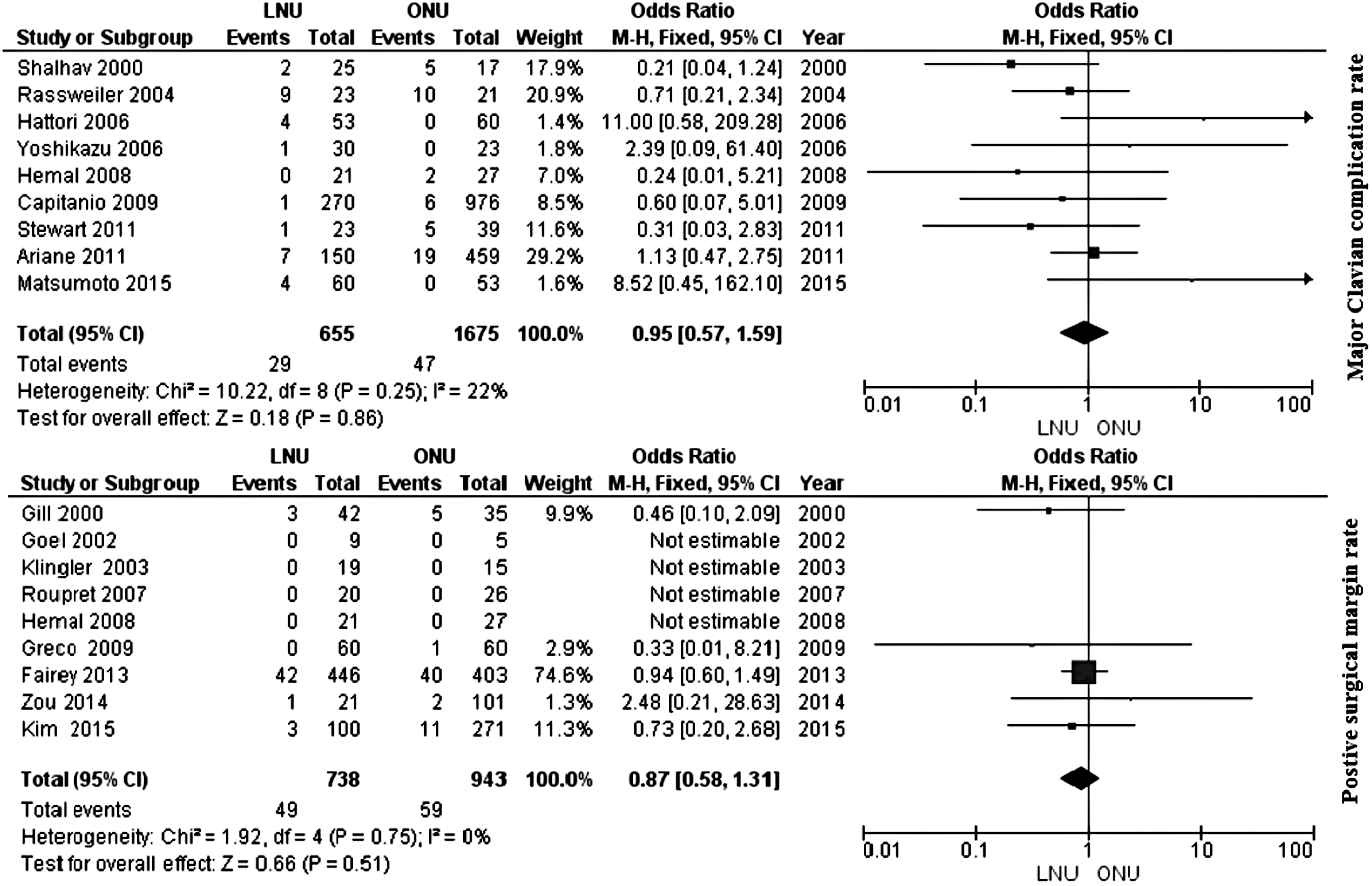
Analysis showed no significant difference in major Clavien complication rate, positive surgical margin between ONU and LNU. LNU, laparoscopic nephroureterectomy; ONU, open nephroureterectomy.
Positive surgical margin
There was no significant heterogeneity between the studies in regard to this outcome (I2 = 0%; P = .75); with fixed effects analysis, there was no significant difference in positive surgical margin between ONU and LNU (OR: 0.87; 95% CI: 0.58–1.31; P = .51; Fig. 6).
Mean operative time (minutes)
There was significant heterogeneity between studies that compared ONU and LNU (I2 = 98%; P < .0001); thus, random effects were used to analyze the outcome. There was a significantly higher operative time in LNU compared to ONU (mean difference: 26.44; 95% CI: 6.45–46.42; P = .01; Fig. 7).

Analysis showed significantly higher operative time, lower length of stay, and lower estimated blood loss and transfusion rate in LNU compared to ONU. LNU, laparoscopic nephroureterectomy; ONU, open nephroureterectomy.
Length of hospital stay (days)
There was significant heterogeneity between studies that compared ONU and LNU (I2 = 99%; P < .0001); thus, random effects were used to analyze the outcome. There was a significantly higher length of hospital stay in ONU compared to LNU (mean difference: −2.66; 95% CI: −3.10 to −2.22; P < .001; Fig. 7).
Mean estimated blood loss (mL)
There was significant heterogeneity between studies that compared ONU and LNU (I2 = 97%; P < .0001); thus, random effects were used to analyze the outcome. There was a significantly higher estimated blood loss in ONU compared to LNU (mean difference: −136.36; 95% CI: −212.48 to −60.24; P = .0004; Fig. 7).
Transfusion rate
There was no significant heterogeneity between the studies in regard to this outcome (I2 = 4%; P = .4); with fixed effects analysis, there was a significantly higher rate of blood transfusion in ONU compared to LNU (OR: 0.57; 95% CI: 0.51–0.64; P < .0001; Fig. 7).
ONU versus HALNU
Five-year CSS rate
There was no significant heterogeneity between studies that compared ONU and HALNU (I2 = 0%; P = 0.96); thus, fixed effects were used to analyze the outcome. There was no significant difference in CSS rate after 5 years between ONU and HALNU (OR: 1.34; 95% CI: 0.69–2.60; P = .39; Fig. 8).
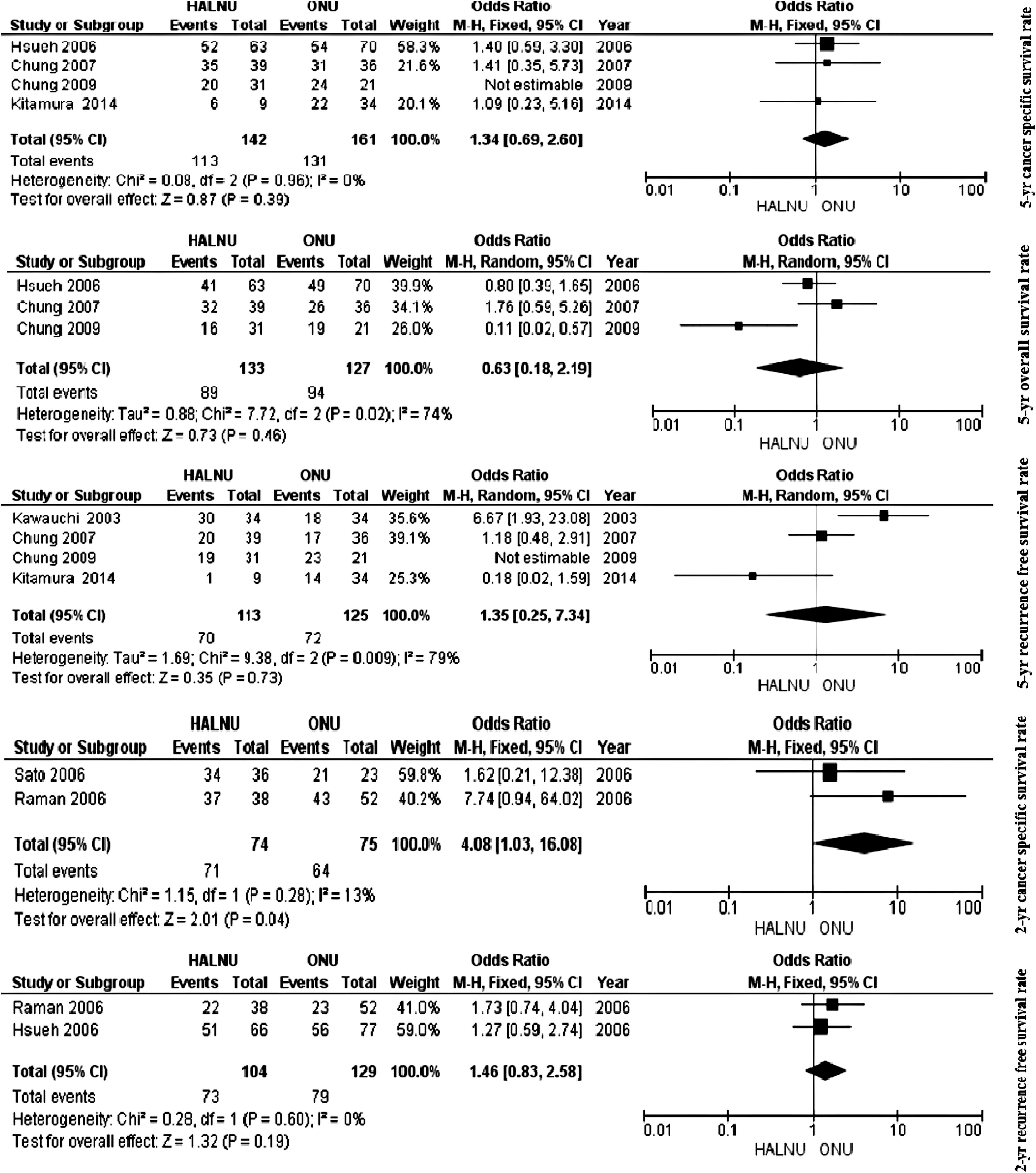
Analysis showed no significant difference in cancer-specific, overall, recurrence-free survival rate after five years between ONU and HALNU. Nevertheless, there was significant difference in CSS rate after 2 years between ONU and HALNU. CSS, cancer-specific survival; HALNU, hand-assisted laparoscopic nephroureterectomy; ONU, open nephroureterectomy.
Five-year OS rate
There was significant heterogeneity between the studies in this outcome (I2 = 74%; P = .02); thus, random effects were used to analyze the outcome. There was no significant difference in OS rate after 5 years between ONU and HALNU (OR: 0.63; 95% CI: 0.18–2.19; P = .46; Fig. 8).
Five-year RFS rate
There was significant heterogeneity between studies that compared ONU and HALNU (I2 = 79%; P = .009); thus, random effects were used to analyze the outcome. There was no significant difference in RFS rate after 5 years between ONU and HALNU (OR: 1.35; 95% CI: 0.25–7.34; P = .73; Fig. 8).
Two-year CSS rate
There was no significant heterogeneity between the studies in regard to this outcome (I2 = 13%; P = .28); thus, fixed effects were used to analyze the outcome. There was a significant difference in CSS rate after 2 years between ONU and HALNU (OR: 4.08; 95% CI: 1.03–16.08; P = .04; Fig. 8).
Two-year RFS rate
There was no significant heterogeneity between studies that compared ONU and HALNU (I2 = 0%; P = .60); thus, fixed effects were used to analyze the outcome. There was no significant difference in RFS rate after 2 years between ONU and HALNU (OR: 1.46; 95% CI: 0.83–2.58; P = .19; Fig. 8).
Bladder recurrence rate
There was significant heterogeneity between the studies in regard to this outcome (I2 = 81%; P < .0001); with random effects analysis, there was no significant difference in intravesical recurrence between ONU and HALNU (OR: 0.91; 95% CI: 0.32–2.59; P = .85; Fig. 9).
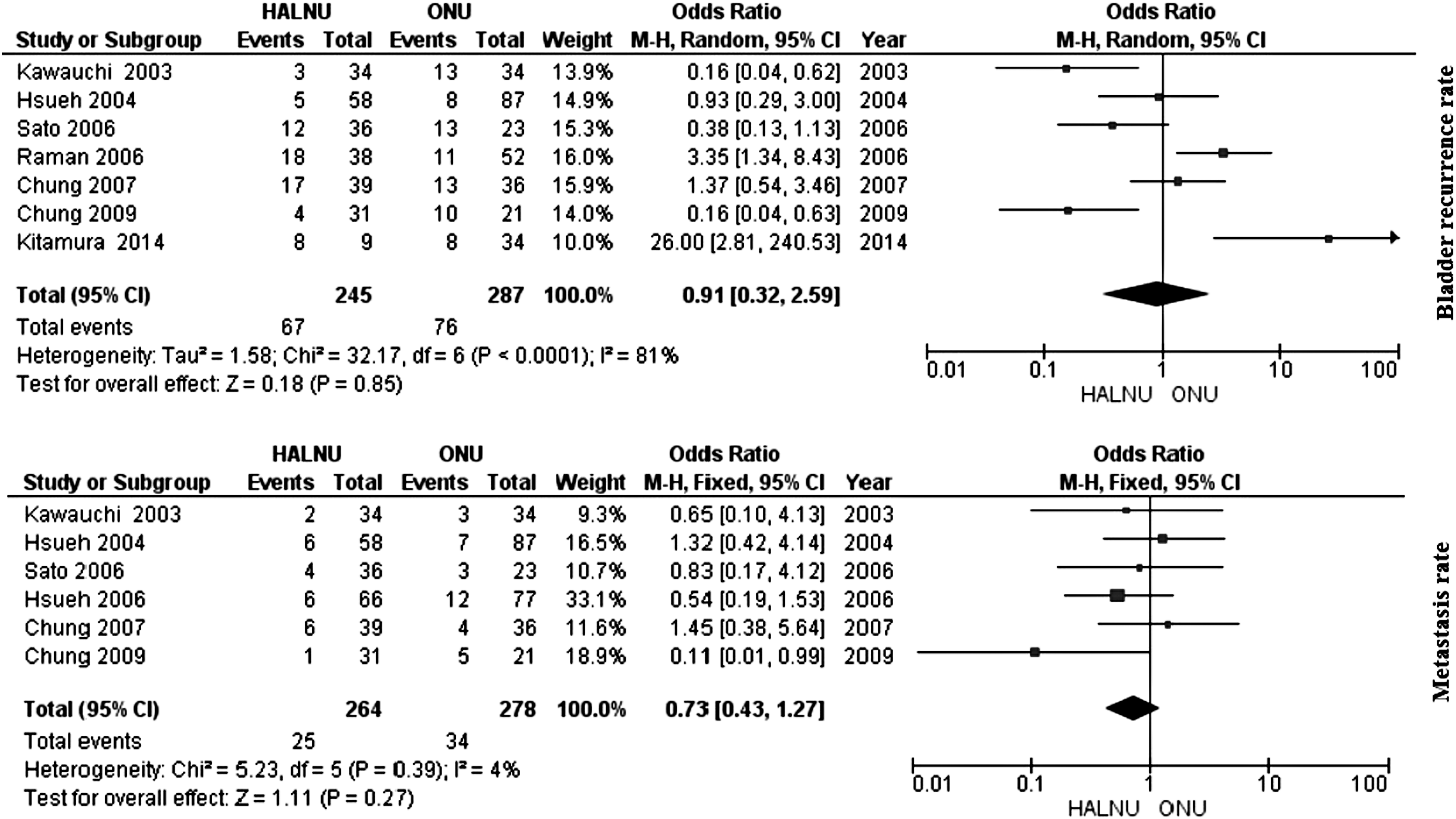
Analysis showed no significant difference in intravesical recurrence, metastasis rate between ONU and HALNU. HALNU, hand-assisted laparoscopic nephroureterectomy; ONU, open nephroureterectomy.
Metastasis rate
There was no significant heterogeneity between the studies in regard to this outcome (I2 = 4%; P = .39); with fixed effects analysis, there was no significant difference in metastasis rate between ONU and HALNU (OR: 0.73; 95% CI: 0.43–1.27; P = .27; Fig. 9).
Major Clavien complication rate
There was no significant heterogeneity between studies that compared ONU and HALNU (I2 = 0%; P = .50); thus, fixed effects were used to analyze the outcome. There was no significant difference in major Clavien complication rate between ONU and HALNU (OR: 1.43; 95% CI: 0.38–5.36; P = .59; Fig. 10).

Analysis showed no significant difference in major Clavien complication rate between ONU and HALNU. There was significantly higher operative time in HALNU compared to ONU. Nevertheless, there was significant higher length of hospital stay and estimated blood loss in ONU compared to HALNU. HALNU, hand-assisted laparoscopic nephroureterectomy; ONU, open nephroureterectomy.
Mean operative time (minutes)
There was significant heterogeneity between studies that compared ONU and HALNU (I2 = 83%; P < .0001); thus, random effects were used to analyze the outcome. There was a significantly higher operative time in HALNU compared to ONU (mean difference: 60.86; 95% CI: 27.30–94.41; P = .0004; Fig. 10).
Length of hospital stay (days)
There was significant heterogeneity between studies that compared ONU and HALNU (I2 = 67%; P < .006); thus, random effects were used to analyze the outcome. There was a significantly higher length of hospital stay in ONU compared to HALNU (mean difference: −3.34; 95% CI: −4.49 to −2.19; P < .001; Fig. 10).
Mean estimated blood loss (mL)
There was significant heterogeneity between studies that compared ONU and HALNU (I2 = 71%; P = .0009); thus, random effects were used to analyze the outcome. There was a significantly higher estimated blood loss in ONU compared to HALNU (mean difference: −215.64; 95% CI: −314.39 to −116.90; P < .0001; Fig. 10).
Transfusion rate
There was no significant heterogeneity between the studies in regard to this outcome (I2 = 0%; P = .66); with fixed effects analysis, there was no significant difference in rate of blood transfusion in ONU compared to HALNU (OR: 0.55; 95% CI: 0.27–1.13; P = .10; Fig. 10).
Discussion
This study is the largest compilation of comprehensive studies on nephroureterectomy patients till date. It is a systematic review and meta-analysis of this large body of literature. Due to the lack of randomized clinical trials, the differences in the patient characteristics between the surgical cohorts could explain the differences in the outcomes between the treatment groups. These differences cannot be fully corrected by statistical methods. In addition, unknown differences in the attributes of the patients and physicians and/or the treatments administered could contribute to the heterogeneous outcomes between the studies. Caution is advised when interpreting the findings of this meta-analysis within the context of the aforementioned considerations. The large number of patients included in the meta-analysis means that the statistically significant results may not necessarily be clinically meaningful.
Open radical nephroureterectomy has been the standard treatment for several decades. Nowadays, to minimize the morbidities, LNU is an appealing option and choosing LNU for treatment of upper urinary tract TCC is rapidly growing, as Inman 6 said, “the horse was already out of the barn.” Nevertheless, most of the studies that compare ONU with LNU are low in quality and consist of only one randomized clinical trial. 7 They have been designed to answer the question of which surgical approach is appropriate.
Regarding the survival outcomes, there is great discrepancy between the studies. Kim et al. 8 performed subgroup analyses by stratifying the study cohort by pathological tumor stages and showed that the LNU group had worse 5-year OS and CSS rates than the ONU group in only the pT3/T4 patients compared with the other stage patients. Moreover, they postulated that the LNU is an independent predictor of OS and CSS rates than ONU. In contrast, Terakawa et al. 9 showed that laparoscopic approach had no independent prognostic impact on the outcomes of the patients. Simone et al., 7 in a randomized prospective study, postulated that the CSS rate and the metastasis free survival rate were significantly in favor of the ONU than the LNU after matching for pT3 and high-grade tumors. These findings highlight the importance of careful selection of the surgical procedure (open or laparoscopic). Nevertheless, the small sample size, single-center experience, and the personal choice of laparoscopic technique could make the bias in the outcomes, especially when the sample size in Simone et al., study 7 was defined based on the mean time of discharge. Also, the oncologic outcomes have to be considered preliminary.
In most of the previous studies,10–12 no significant differences were found regarding the oncologic outcomes between the LNU and ONU. Our analysis found that the LNU had similar or better oncologic efficacy than the ONU. Other reasons for those inconsistent results could be explained as follows: owing to the retrospective nature of the studies, it is likely that there may be some inherent bias. In some studies, the surgical cases spanned multiple years with multiple surgeons, which resulted in the variation in surgical expertise and learning curve for laparoscopic surgery among surgeons, which could not be clearly identified in their studies, besides these factors perhaps being responsible for affecting the survival outcomes after the LNU. Also, given that most patients did not receive pelvic lymph node dissection in the studies, which is considered an important part in the current management of the upper urinary tract TCC. More importantly, all the oncologic outcomes should have been compared by pathologic stage and grade as preplanned. Unfortunately, such analyses could not be achieved due to insufficient data. In addition, the inclusion of patients with a prior or concomitant history of bladder cancer may affect the oncologic outcome of treating upper tract TCC; besides, this factor is not similar between the studies. Therefore, further studies with larger cohorts of patients and long follow-up will be able to provide a conclusive data.
Regarding the bladder recurrence, Xylinas et al. 13 showed that the laparoscopic approach was associated with a higher risk of intravesical recurrence than open surgery. It was suggested that the high-pressure pneumoperitoneum during LNU might trigger tumor dissemination and could result in a higher rate of recurrence. Some authors14,15 drew a similar conclusion, whereas others did not confirm these results.16,17 Our finding showed no significant difference in the rate of bladder recurrence between LNU and ONU. A recently published review described multifocality as the only repeatedly mentioned significant risk factor for bladder cancer recurrence after upper urinary tract TCC. 18 Nevertheless, Fradet et al. 19 showed that the age of every patient at diagnosis raises the risk of developing subsequent bladder cancer by 2.8% and reported tumor location in both the renal pelvis and the ureter. Treating with adjuvant systemic chemotherapy, extravesical ureterectomy and LNU were the factors with higher rate of bladder recurrence after nephroureterectomy. The question might arise whether probably other co-factors, such as distal ureter management, could be responsible for these discrepancies between the results. The patients subjected to LNU were more likely to undergo open bladder cuff excision or the transurethral resection of the orifice. Thus, we would expect a selection bias affecting the outcomes against ONU.
In our analysis, intraoperative and postoperative outcomes were found similar to the previous findings that exhibited a higher operative time, lower length of hospital stay, lower estimated blood loss, and a need to transfusion rate in LNU versus ONU.
On the comparison of HALNU with ONU, we found that the oncologic outcomes were comparable between the two approaches. Several reports have evaluated the short-term oncologic outcomes of HALNU in treating upper urinary tract TCC.20–23 Chung et al. in 2007 24 and 2009 25 compared these two approaches and showed that the oncologic outcomes were comparable between the two groups. Also, they found better perioperative outcomes and lower length of hospital stay in the case of HALNU. Raman et al. 26 compared the 38 patients who underwent HALNU with the 52 patients who underwent ONU. They showed that HALNU is an effective modality for the treatment of the upper urinary tract urothelial carcinoma. Patients benefited from less intraoperative blood loss and a shorter hospitalization with an equivalent intermediate-term oncologic outcome compared with that of the open approach. Our results were in agreement with previous studies, in which perioperative and postoperative morbidities were better in HALNU than ONU.
Conclusion
We also acknowledge certain inherent limitations in the studies included in our meta-analysis, which cannot be ignored when interpreting our data. First, most of the studies included in our analysis were retrospective, which is a reflection of the rarity of the disease. Second, the clinical and pathologic characteristics of the patients were different in the included trials. Similar to the other laparoscopic procedures, the LNU might be selectively performed in risk-favorable patients at an earlier tumor stage and therefore, the results of our analysis favoring LNU could be attributed mainly to a bias in the data from the LNU study arms. Third, the urologists widely accept that the distinguished differences that exist in the biological behavior and patients' prognosis between the locoregional recurrence and the recurrence in the remnant urothelium. Finally, it is well known that the indications for LNU were much stricter than those for ONU because of the more stringent requirements for comorbidities such as body mass index, cardiopulmonary disease, and previous abdominal surgery. Despite the fact that no data on the comorbidity status have been reported in this analysis, it could be regarded as a confounder in patient selection.
Footnotes
Acknowledgments
We thank Golnaz Shemshaki for assisting in the preparation of this article. Funding: Urology and Nephrology Research Center, Shahid Labbafinejad Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Authors' Contributions
H.S. and B.J. designed the research, interpreted the data, and revised the article. A.N., S.T., M.S., and N.S. performed the data extraction, carried out the meta-analysis, and drafted the article. All the authors approved the submitted and final version.
Ethics Approval and Consent to Participate
All analyses were based on previously published studies; thus, no ethical approval and patient consent are required.
Availability of Data and Materials
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Disclosure Statement
No competing financial interests exist.