
Abstract
Abstract
Purpose:
The Nuss procedure for surgical correction of pectus excavatum often causes severe postoperative pain. Cryoanalgesia of intercostal nerves is an alternative modality for pain control. We describe our modification of the cryoICE™ probe that allows for nerve ablation through the ipsilateral chest along with early results utilizing this technique.
Methods:
To allow for ipsilateral nerve ablation, a 20-French chest tube was cut and secured to the cryoICE probe, thus providing insulation for the malleable end of the probe. A 3-year retrospective review of patients undergoing Nuss repair at our institution was performed. Patients who received cryoanalgesia (cryo, n = 6) were compared with a historical control cohort who did not receive cryoanalgesia (nocryo, n = 13) during Nuss repair. Hospital length of stay, postoperative narcotic requirement (PNR), and highest postoperative pain score were collected.
Results:
Both cohorts were similar regarding age, BMI, and pectus index. The cryo group had a significantly less PNR (6.4 versus 17.9 doses, P = .05) and was discharged on average >1 day earlier than nocryo patients (3.7 versus 2.2 days, P = .01). No complications occurred in either group.
Conclusions:
Our technique modification simplifies previously described approaches to intercostal nerve cryoablation. Patients undergoing this adjunct benefit with less PNR and a faster discharge time.
Level of Evidence: Level III—Case control study, Retrospective comparative study.
Introduction
S
Cryoanalgesia of the intercostal nerves in conjunction with Nuss repair for pectus excavatum has recently shown promising results.8–10 Previous reports describe utilizing a sternal elevator and a transmediastinal approach to access the contralateral chest when performing cryoanalgesia.8,10,11
We describe a technique modification that allows for ipsilateral cryoablation through the same incisions utilized for the Nuss repair and describe our initial results with this technique.
Materials and Methods
A study protocol was submitted to and approved by our institution's Institutional Review Board.
Anesthesia
All patients underwent general anesthesia at the same hospital with the use of propofol and a narcotic pain medication (usually 100–350 mcg fentanyl except for 2 nocryo patients who received Dilaudid instead of fentanyl). Most patients (except for 3; 2 in the nocryo group and 1 in the cryo group) received intraoperative Tylenol®. One patient in the cryo group also received a dose of ketamine.
Surgical technique
Before start of cryoablation, the cryoICE™ probe is modified by cutting a 20-French chest tube and sliding the malleable portion of the probe through. The chest tube is then secured to the nonmalleable insulation of the probe using steri-strips (Fig. 1). This allows the surgeon to curve the probe while maintaining insulation over the portion of the probe that would otherwise be exposed. Standard incisions for Nuss procedure are made and the curved probe is introduced into the ipsilateral chest under thoracoscopic observation (Fig. 2). Cryoanalgesia of the ipsilateral intercostal nerves two ribs above and two ribs below site of bar insertion is then performed. The procedure is then performed in a similar manner for the contralateral intercostal nerves.
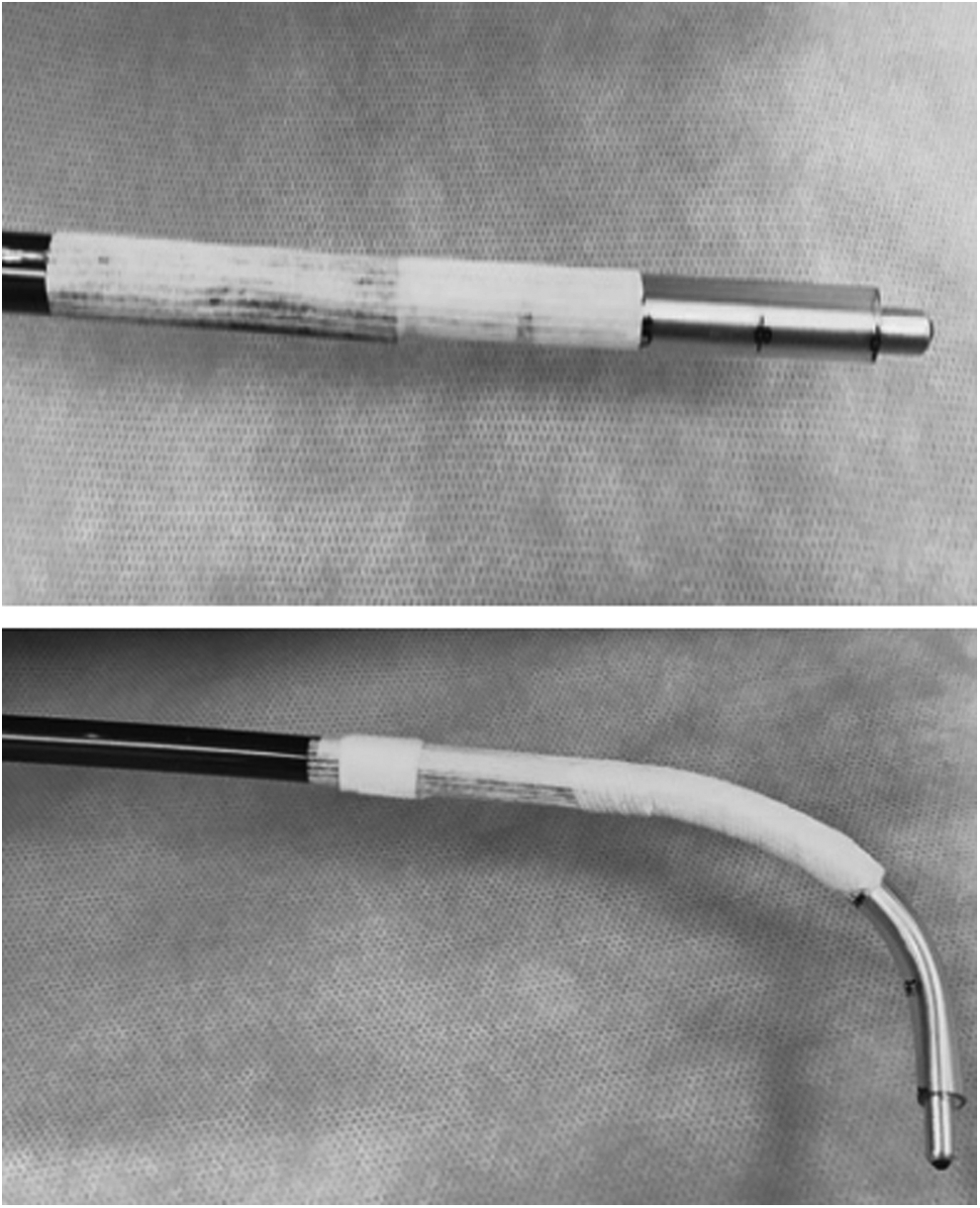
A 20-French chest tube cut (above image) and secured to cryoICE™ probe allowing for bending of malleable portion of probe (below image) while providing insulation.

Ipsilateral thoracoscopic view of cryoICE probe on intercostal nerve.
Postoperative management
Pain management was slightly different between the two groups. The cryo group also received gabapentin, scheduled Tylenol, Toradol® as needed, and a patient-controlled analgesia (PCA) pump that was discontinued on POD 1 and switched to oral pain medications. The nocryo group received local anesthetic given through an ON-Q™ infusion pump for 72 hours, scheduled Tylenol, prn Toradol, along with a PCA pump that was not discontinued on post-operative day (POD) 1 but instead was left in place until the patient's pain scores were satisfactory for switching to an oral regimen.
Retrospective review
A retrospective chart review of all pediatric patients undergoing Nuss repair at our institution from January 2014 to January 2017 was performed. Patients who received cryo (n = 6) during Nuss repair were compared with the nocryo group (n = 13).
Data collection and analysis
Data analyzed from the chart review included operative time, number of intravenous narcotic dosages required (0.1 mg/kg morphine sulfate equivalent = 1 narcotic dose), highest pain score recorded, time to discharge (days), and complications. The primary outcome measurement was time to discharge. Student's t-test was used for statistical analysis.
Results
A total of 19 patients who underwent initial Nuss bar placement during the 3-year study period were included (13 nocryo and 6 cryo). Average age was 14 years for both groups.
Average BMI
Average weight and height for the cryo group was 54.4 kg and 171.2 cm, respectively, versus 51.8 kg and 166.1 cm for nocryo group. Average BMI was 18.4 kg/m2 for the cryo group and 18.2 kg/m2 for the nocryo group.
Average pectus index
The nocryo group had an average pectus index value of 4.41, similar to the cryo group's average pectus index value of 4.23, P = .81. Most patients were noted to have severe extent of malformation but for some (8 patients), only the pectus index was noted. Three patients in the nocryo group required 2 bar placement whereas only 1 patient in the cryo group required 2 bars.
Operative time
Average operative time in the cryo group was 128 minutes (101–179 minutes) versus 121 minutes in the nocryo group (75–189 minutes).
Postoperative narcotic requirement
Patients in the cryo group required significantly less narcotic dosages (6.4 ± 5.6) as compared with patients in the nocryo group (17.9 ± 12.3), P = .05.
Highest postoperative pain score
Patients in both groups had similar highest reported postoperative pain scores (cryo 8.0 ± 1.9 versus nocryo 7.3 ± 1.6), P = .4.
Time to discharge
Patients who underwent cryoanalgesia were discharged significantly sooner (2.2 ± 0.4 days) than the historical control group (3.7 ± 1.2 days), P = .01.
Complications
There were no complications in either group with regard to cryoablation; however, 2 patients in the cryo group had an allergy to the metal in the bar. One was treated with a steroid taper and the other required removal.
Discussion
The Nuss procedure has proven to be a very safe and effective method for correction of pectus excavatum.2–4 It is widely accepted as the preferred approach for correction of this chest wall abnormality; however, its main drawback, postoperative pain, is well documented.5–8 Numerous studies have compared traditional methods of postoperative analgesia including narcotics, nonsteroidal anti-inflammatory medications, local anesthetic infusion devices, and epidural infusions with limited success in reducing postoperative pain.12–18
Cryoanalgesia has recently been reported to show very promising results when compared with other traditional pain control modalities.6–8 Keller et al. and Graves et al. reported significantly reduced time to discharge and reduced narcotic requirement when comparing cryoanalgesia patients with their historical control patients who received thoracic epidurals.
As our group sought to employ the use of cryoanalgesia for our patients undergoing Nuss repair, we were concerned about passing the probe transmediastinally and sought to modify the technique to allow for ipsilateral treatment of the intercostal nerves with the cryoICE probe. The chest tube provides malleable insulation to protect surrounding tissue from touching unexposed probe and allows the probe to be passed from the ipsilateral chest with good thoracoscopic observation. The modifications to the probe are quick and easy to perform and obviate the need for sternal elevation and passage of the probe across the mediastinum. Therefore, although the technique of ablation is certainly not new, we have modified the approach for our pediatric population.
Although cryoanalgesia requires the probe to sit on each intercostal nerve for 2 minutes theoretically adding a minimum of 20 minutes to standard operative time (2 minutes × 5 nerves × 2 sides), we found that operative time was not significantly increased. We suspect this may be due, in part, to the elimination of placing local anesthetic infusion devices for cryo patients.
Highest postoperative pain score was similar between the two groups and was actually slightly higher in the cryo patients. This difference, however, was minimal and not statistically significant when considering the small sample size of this study.
Postcryoanalgesia neuralgia has been noted as a complication in multiple (but not all) studies on the subject.10,19–23 As far as we know, none of the patients complained of neuralgia symptoms. Sensation usually returned in 2–3 months after cryoanalgesia administration; however, exact timing was not annotated in follow-up visits except for 1 patient who noted sensation was returning at 2 months postoperation. A prospective study is planned to look closer at the time for return of sensation.
Our study results show a significant decrease in postoperative narcotic usage and a significantly shorter time to discharge. A 10-year review shows an average time to discharge of 4.3 days, which is similar to our historical cohort. 1 Our cryo group had markedly shorter discharge of 2.2 days. In comparison with the Keller and Graves studies, we did not use thoracic epidurals in our historical control cohort. Our nocryo patients received only local anesthetic infusion in conjunction with patient-controlled opioid analgesia. This would suggest similar efficacy of local anesthetic infusion when compared with thoracic epidural; however, that comparison is not within the scope of this study. This data is also subject to the biases and limits associated with retrospective reviews.
Conclusion
We report a novel technique modification that allows for what we feel is a simplified approach to performing intercostal nerve cryoanalgesia for patients undergoing Nuss repair of pectus excavatum. Operative time is not significantly increased and our preliminary results suggest that this procedure can be performed safely while reducing patient narcotic usage and expediting time to discharge. Although cryoanalgesia is not new, we hope to add to the currently small body of literature supporting this modality of analgesia while also providing a novel technique.
Footnotes
Disclosure Statement
No competing financial interests exist.
The views expressed in this article are those of the authors' and do not reflect the official policy or position of the Department of the Army, Department of Defense, or the U.S. Government.