
Abstract
Abstract
Background:
The short-term benefits of laparoscopy for rectal surgery are equivocal. The objective of this study was to determine the clinical and economic impact of an enhanced recovery pathway (ERP) for laparoscopic and open rectal surgery.
Materials and Methods:
All patients who underwent elective rectal resection with primary anastomosis between January 2009 and March 2012 at two tertiary-care, university-affiliated institutions were identified. Patients who met inclusion criteria were divided into four groups, according to surgical approach (laparoscopic [lap] or open) and perioperative management (ERP or conventional care [CC]). Length of stay (LOS), postoperative complications, and hospital costs were compared.
Results:
A total of 381 patients were included in the analysis (201 open-CC, 34 lap-CC, 38 open-ERP, and 108 lap-ERP). Patients were mostly similar at baseline. ERPs significantly reduced median LOS after both open cases (open-CC 10 days versus open-ERP 7.5 days, P = .003) and laparoscopic cases (lap-CC 5 days versus lap-ERP 4.5 days, P = .046). ERPs also reduced variability in LOS compared with CC. There was no difference in postoperative complications with the use of ERPs (open-CC 51% versus open-ERP 50%, P = .419; lap-CC 32% versus lap-ERP 36%, P = .689). On multivariate analysis, both ERP (−3.6 days [95% confidence interval, CI −6.0 to −1.3]) and laparoscopy (−3.6 days [95% CI −5.9 to −1.0]) were independently associated with decreased LOS. Overall costs were only lower when lap-ERP was compared with open-CC (mean difference −2420 CAN$ [95% CI −5628 to −786]).
Conclusions:
ERPs reduced LOS after rectal resections, and the combination of laparoscopy and ERPs significantly reduced overall costs compared to when neither strategy was used.
Introduction
U
However, perioperative management was not standardized in the landmark trials comparing laparoscopic and open rectal resections,2–5 which may play as important a role as surgical approach in improving postoperative recovery and minimizing postoperative morbidity. Enhanced recovery pathways (ERPs) are multidisciplinary clinical care pathways that incorporate multiple evidence-based interventions to decrease surgical stress and improve patient recovery and clinical outcomes.10,11 ERPs decrease hospitalization and morbidity12,13 and may reduce costs, 14 compared with conventional perioperative care for colorectal surgery. There are also data suggesting that ERPs may further improve outcomes after laparoscopic colectomy compared with conventional care (CC).15,16 However, few studies have examined the impact of ERPs in a population of patients undergoing rectal surgery only. We hypothesized that an ERP would further improve clinical outcomes and decrease medical costs for laparoscopic versus open rectal surgery. The objectives of this study are to determine the clinical and economic impacts of an ERP compared with conventional perioperative management for open and laparoscopic rectal surgery.
Materials and Methods
With Institutional Review Board approval, all patients who underwent elective rectal resection with primary anastomosis in the upper-, mid-, or low-rectum between January 2009 and March 2012 at two tertiary-care, university-affiliated institutions (located in the same city and affiliated with the same university) were identified and audited. All cases were performed by fellowship-trained colorectal surgeons with similar workloads. Patients who underwent end colostomy or major concomitant procedures, such as hepatectomy or peritonectomy, were excluded (synchronous uterine or partial bladder resections were included), as were procedures performed by a noncolorectal surgeon. An ERP has been in place at one of the two institutions since 2006 (Table 1). 17 In 2009, over 80% of all cases performed at this institution were managed by ERP. Before October 2010, patients with major intraoperative complications, those with major concomitant procedures, and those who underwent extensive adhesiolysis or dissection during the primary procedure were not enrolled. None of these cases were included in this analysis. Starting in October 2010, all such patients were enrolled in the ERP (and thus the analysis). The other participating institution managed patients by conventional perioperative management (Table 1). Therefore, all cases managed by ERP were performed at one institution, and cases managed by CC from the other. Patients who met the inclusion criteria were divided into four groups, according to surgical approach and perioperative management: open and conventional care (open-CC), open and enhanced recovery pathway (open-ERP), laparoscopy and conventional care (lap-CC), and laparoscopy and enhanced recovery pathway (lap-ERP).
DVT, deep vein thrombosis; POD, postoperative day.
Patient, operative, and pathologic characteristics were recorded. Clinical outcomes were recorded up to 30 days postoperatively. LOS included primary hospitalization and any readmissions that occurred within 30 days of initial surgery. Anastomotic leak included perianastomotic abscesses diagnosed by computed tomography or leaks diagnosed intraoperatively. Cardiopulmonary complications included myocardial infarction, pulmonary edema requiring diuresis, pneumonia, new onset arrhythmias, or pulmonary embolism. Surgical site infections (SSIs) were defined as per Centre for Disease Control definition. 18 The most severe postoperative morbidities were also categorized as per the Clavien–Dindo classification of surgical complications. 19
The economic evaluation was performed from an institutional perspective, using a time horizon of 30 days. Medical costs were calculated by microcosting, in which the frequencies of each resource consumed were recorded, and multiplied by their respective unit cost to generate the total medical costs. Unit costs were obtained from the finance and accounting department of each institution, or were derived by dividing the total direct costs by the total output (e.g., number of patient bed-days occupied for a specific ward; figures obtained from the provincial health ministry 20 ) if not directly available. All unit costs included overhead (e.g., administration, information technology, and housekeeping), which was distributed by direct allocation. Physician fees were not included, as they are not paid by the hospital within the Canadian healthcare system. Operative costs included the cost of nursing, anesthesia, and equipment. Postoperative costs included laboratory, pharmacy, radiology, allied health professionals (such as physiotherapists and occupational therapists), and any costs associated with reoperations. All costs were adjusted to 2012 Canadian dollars using the real healthcare inflation rate, which is specific for healthcare services and adjusted for population growth. 21
Univariate comparisons among the four groups were performed using Chi-squared or Fisher's exact tests for categorical variables and ANOVA or Kruskal–Wallis for continuous variables. Due to the extreme right-skewedness of cost data, 95% confidence intervals (CIs) around point estimates were derived from bootstrap estimates (10,000 iterations) taken at the 2.5th and 97.5th percentiles. Multivariate analyses were performed using linear and logistic regression to determine the independent effect of laparoscopy and ERP on LOS and complications after adjusting for confounders. The interaction between laparoscopy and ERP was also tested for each outcome, and reported if significant. All statistical analyses were performed using STATA 12 (StataCorp, College Station, TX).
Results
A total of 381 patients were included in the analysis (201 open-CC, 34 lap-CC, 38 open-ERP, 108 lap-ERP). There were no differences in age, gender, body mass index, Charlson Comorbidity score, indication for surgery, anastomosis location, and number of cases in which a new stoma was created among the four groups (Table 2). More patients managed by ERP received neoadjuvant therapy compared with those managed by CC (51% versus 34%, P = .005). Procedure duration was significantly different among the four groups (open-CC 3.3 hours versus open-ERP 3.4 hours versus lap-CC 4.7 hours versus lap-ERP 3.8 hours, P < .001). There was no difference in the number of conversions between the lap-CC and lap-ERP groups (17% versus 10%, P = .214) (Table 2).
Data are presented as means with (SD) or percentages with (n). Percentages may not add up due to rounding.
P value comparing open-CC and open-ERP.
P value comparing lap-CC and lap-ERP.
P value comparing differences across the four groups.
CC, conventional care; ERP, enhanced recovery pathway; NA, not applicable; OR, operating room; SD, standard deviation.
Median LOS was significantly higher in the open-CC group compared to open-ERP, lap-CC, and lap-ERP groups (10 days versus 7.5 days versus 5 days versus 4.5 days, P < .001) (Table 3). More specifically, ERP significantly reduced median LOS after both open cases (open-CC 10 days versus open-ERP 7.5 days, P = .003) and laparoscopic cases (lap-CC 5 days versus lap-ERP 4.5 days, P = .046). In patients who did not experience a postoperative complication, this difference in median LOS was more pronounced (open-CC 8 days versus open-ERP 4 days, P < .001; lap-CC 5 days versus lap-ERP 4 days, P = .001) (Table 3). There was also a difference in LOS among the four groups in patients who did experience a complication (open-CC 14 days versus open-ERP 13 days versus lap-CC 13 days versus lap-ERP 10 days, P = .037) (Table 3). However, there was no difference when comparing only open cases or only laparoscopic cases (P = .376 and P = .418, respectively) (Table 3). There was also much lower variability in LOS in patients managed by ERP compared with those managed by CC (Fig. 1). Laparoscopy was also associated with lower median LOS compared to open surgery in patients managed by CC (lap-CC 5 days versus open-CC 10 days, P < .001) and in patients managed by ERP (lap-ERP 4.5 days versus open-ERP 7.5 days, P = .024). On multivariate analysis, both ERP (−3.6 days [95% CI −6.0 to −1.3]) and laparoscopy (−3.6 days [95% CI −5.9 to −1.0]) were independently associated with decreased LOS, after adjusting for age, comorbidities, and the creation of a new stoma.
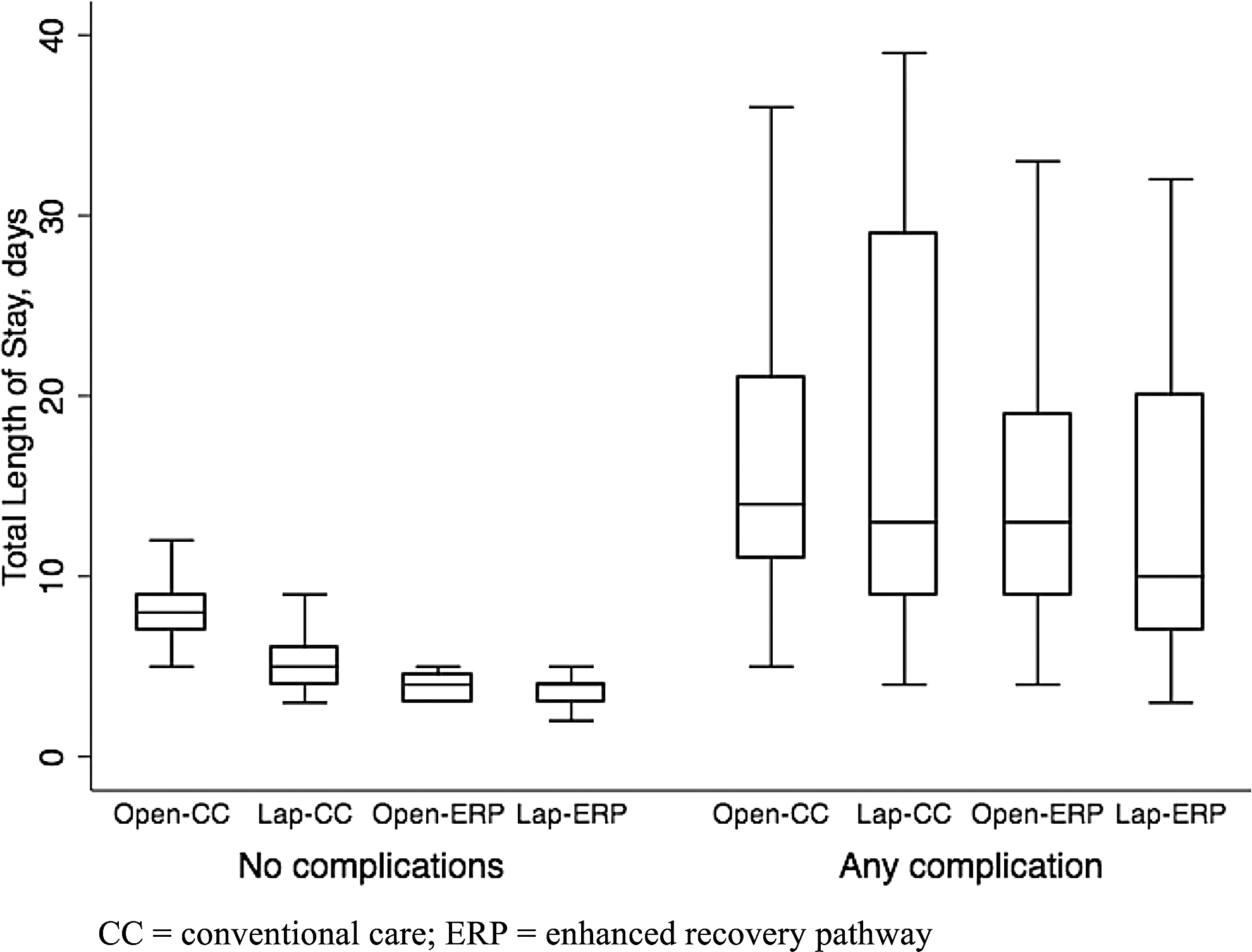
Comparison of the variability in length of stay among the four groups.
Data are presented as medians with [IQR] or percentages with (n). Percentages may not add up due to rounding.
P value comparing open-CC and open-ERP.
P value comparing lap-CC and lap-ERP.
P value comparing differences across the four groups.
CC, conventional care; ER, emergency room; ERP, enhanced recovery pathway; IQR, interquartile range; LOS, length of stay; SSI, surgical site infection; UTI, urinary tract infection.
The incidence of postoperative complications was also different among the four groups (Table 3). However, this was more related to surgical approach, as there were significant differences between laparoscopic and open cases in patients managed by ERP (lap-ERP 36% versus open-ERP 50%, P = .019) and by CC (lap-CC 32% versus open-CC 51%, P = .047), but no differences between ERP and CC in cases performed laparoscopically (lap-ERP 36% versus lap-CC 32%, P = .689) and open (open-ERP 50% versus open-CC 51%, P = .419). The incidences of anastomotic leak, cardiopulmonary complications, and SSIs were similar among the four groups. However, the incidence of urinary tract infection was highest in the open-CC group (open-CC 8% versus open-ERP 3% versus lap-CC 3% versus lap-ERP 1%, P = .033) (Table 3). There were no differences in mortality, emergency room visits, or readmissions among the four groups (Table 3). On multivariate analysis, only laparoscopy was independently associated with decreased complications (OR 0.45 [95% CI 0.26–0.79]), whereas ERP was not (OR 1.12 [95% CI 0.64–1.96]), after adjusting for age, comorbidities, and the creation of a new stoma.
The mean overall, operative, and postoperative costs of the four groups are reported in Table 4. Laparoscopy was associated with significantly higher operative costs compared with open approach in both the ERP (mean difference +1381 CAN$ [95% CI 895–1790]) and CC (mean difference +2104 CAN$ [95% CI 1585–2593]) groups. There were no differences in operative costs between lap-ERP and lap-CC, or open-ERP and open-CC. Postoperative costs were lower in lap-CC compared with open-CC (mean difference −4459 CAN$ [95% CI −7142 to −1732]) and in open-ERP versus open-CC (mean difference −2398 CAN$ [95% CI −5618 to −567]), but not between lap-ERP versus open-ERP or lap-ERP versus lap-CC. Overall costs were only lower when lap-ERP was compared with open-CC (mean difference −2420 CAN$ [95% CI −5628 to −786]). There were no significant differences between the remaining groups (Fig. 2).
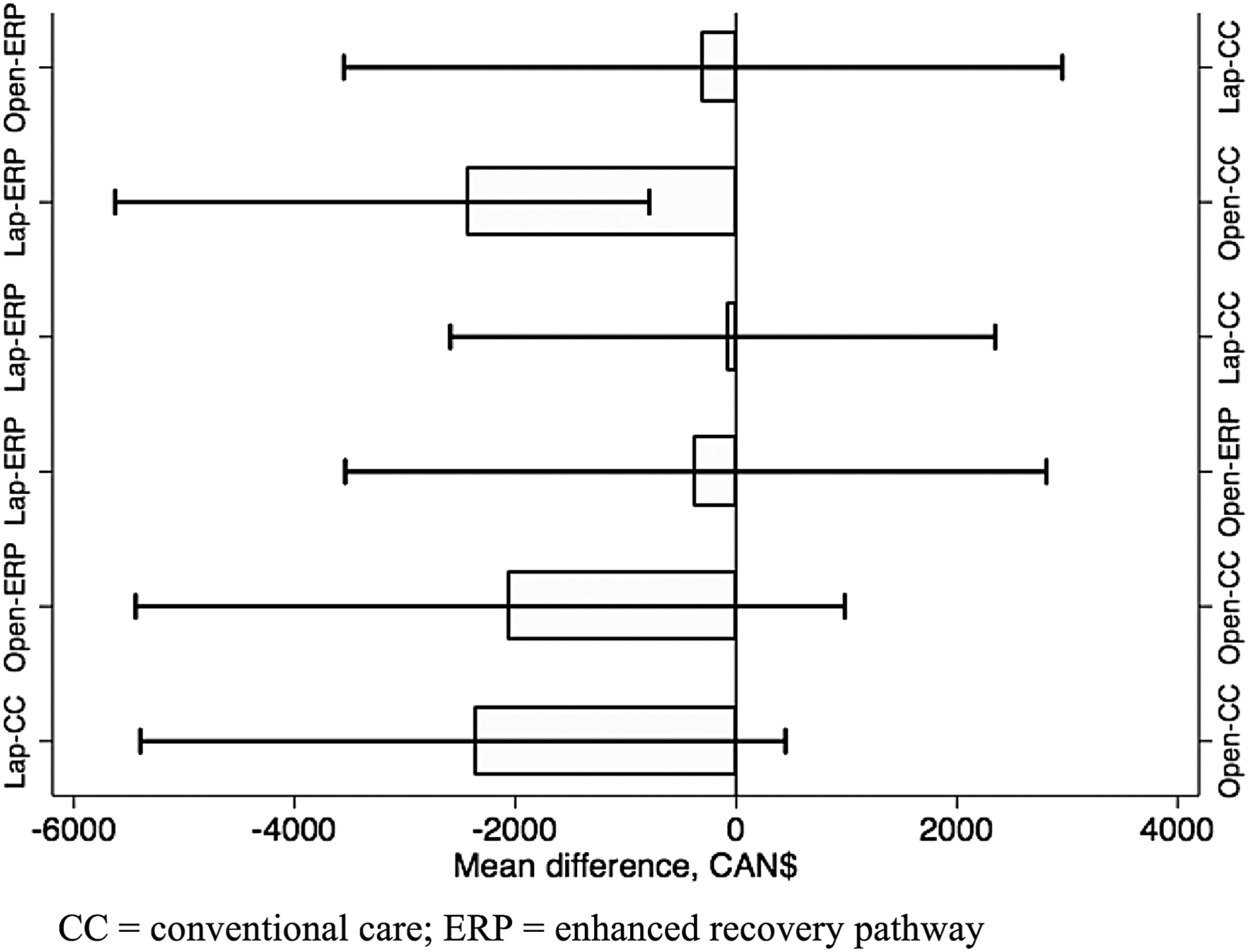
Mean differences and 95% CIs (represented by whiskers) in overall cost between groups. CIs were derived from bootstrap estimates (10,000 iterations). Ninety-five percent CIs that do not cross 0 (vertical line) denote significant results. CI, confidence interval.
CC, conventional care; CI, confidence interval; ERP, enhanced recovery pathway.
Discussion
In the present study, we investigated the impact of ERPs on clinical and economic outcomes after laparoscopic and open rectal surgery. Our results demonstrate that the use of ERPs was associated with significant reductions in LOS after both open and laparoscopic procedures, both of which were more pronounced in patients who did not develop a postoperative complication. ERPs also reduced variability in LOS. Laparoscopy similarly reduced LOS in both CC and ERP cases, and both ERPs and laparoscopy remained significant in reducing LOS on multivariate analysis. The use of laparoscopy and ERPs together also significantly reduced overall cost compared to when neither was used. Where the short-term benefits of laparoscopy for proctectomy have not been readily apparent,2–5 the addition of ERPs works synergistically to maximize patient outcomes. When it can be applied appropriately, laparoscopy is an integral element of an optimal ERP.
Few other groups have reported on the use of ERPs in rectal surgery specifically. Khreiss et al. reviewed the Mayo Clinic experience of minimally invasive rectal cancer surgery and demonstrated that ERPs reduced the average LOS from 6 to 4 days, and that 31% of patients managed within an ERP were discharged by postoperative day 2. 22 They also observed no difference in 30-day readmission with the use of ERPs, similar to our study. Two other series similarly reported 3-day reductions in LOS among laparoscopic rectal resections without an increase in readmission rates.23,24 Huebner et al. reported on their 7-year, single institution experience of minimally invasive rectal resections and found that ERPs only reduced LOS in patients without a complication. 25 This is consistent with the present study, where the difference in LOS was more pronounced in patients without postoperative complications.
The majority of patients in this study did not experience any postoperative complications, and the benefits of ERPs appear greatest in this population. ERPs also reduced variability in LOS, which may allow for more predictable discharge planning. However, once a patient develops a postoperative complication, he or she falls off the pathway and no longer extracts any benefit from the ERP, as evidenced by the similar LOS between open and laparoscopic cases with or without ERPs. Huebner et al. found that more complications were identified within the first 3 days postoperative in ERP patients compared with CC patients, proposing that early detection may lead to earlier discharge. However, they could not demonstrate this effect on LOS in ERP patients with complications. 25
Even more scarce in the literature are reports of the use of ERPs after open rectal resections. The aforementioned studies all focused on laparoscopic proctectomies, which undoubtedly plays a major role in the implementation of ERPs. However, it is perhaps after open surgery that the benefits of ERPs are most needed and can be maximized. Keane et al. reviewed their experience of 105 rectal operations with the majority being open, and demonstrated significant reductions in LOS (8 days versus 10 days) with ERPs. 26 The Laparoscopy and/or Fast Track Multimodal Management Versus Standard Care (LAFA) study found no difference in LOS after open surgery using fast-track or standard care postoperative management, but in colonic surgery only. 16 In the present study, a greater reduction in LOS with ERPs was observed after open rectal resections compared with laparoscopic resections. Furthermore, in patients without postoperative complications, the median LOS was 4 days with either surgical approach if an ERP was used. We also did not select cases to enroll onto an ERP, meaning that even complicated open procedures (major intraoperative complications, concomitant procedures, and extensive adhesiolysis) were enrolled onto ERPs for the majority of the study period. In the context of the best available evidence, the use of laparoscopy for rectal cancer is still being questioned.4,5 The majority of rectal resections are still being performed open,8,9 and implementation of ERPs for these patients may have important implications for decreased hospitalization and resource utilization.
Similar to previous studies, we found no difference in complications among patients managed by ERP or CC.22–25 This remained true for both procedures performed open or laparoscopically. Conversely, surgical approach did impact the development of complications, as fewer complications occurred after laparoscopic procedures regardless of perioperative management plan. Only laparoscopy was independently associated with a reduction in complications on multivariate analysis. Many other studies have also reported a decrease in complications after laparoscopic rectal resections,27–29 but not unequivocally.2–5 With regard to individual complications, only urinary tract infection was statistically different among the four groups, with the highest incidence in the open-CC group and trending down to 1% in the lap-ERP group. This could, in part, be explained by the use of Foley catheters, which may be removed earlier in patients undergoing laparoscopic surgery in an ERP. 30
Literature on the economic impact of either laparoscopy or ERPs in rectal resections is conflicting. With laparoscopy, the debate usually hinges on whether or not the postoperative savings can outweigh the increase in operative cost. While some studies have found laparoscopy to be cost-effective, 31 most have found that it increases total hospital costs, including a large multicenter report from the Netherlands.32,33 This differs from colonic surgery, where the Dutch group found laparoscopy to be cost-effective, 33 perhaps reflecting the relative complexity of minimally invasive rectal surgery and its slower adoption. 34 ERPs in colorectal surgery have been shown to decrease costs, but with limited evidence.14,35 In the present study, neither laparoscopy nor ERPs had an independent impact on cost; however, there was a significant reduction in overall costs when laparoscopy and ERPs were used, compared with when neither was used. Laparoscopy not only reduced postoperative complications—the treatment of which incurs an additional cost in itself—but also when combined with ERPs, it allows for the 60%–70% of patients who do not experience a complication to consistently meet the targeted discharge of postoperative day 3, which further reduces postoperative costs. This exemplifies how patient outcomes can be maximized with both laparoscopy and ERPs. 36 Furthermore, ERPs can result in culture change, which may provide clinical and economic benefits beyond the specific ERP itself, 37 but which are not as easily captured or measured.
There are several limitations to this study. First, selection bias may be present given the study design. Decision to enroll a patient onto an ERP was dictated by institution, which may have led to systematic differences between groups. However, we did not demonstrate any difference in baseline patient characteristics among the four groups other than the use of neoadjuvant therapy, which has not been shown to affect postoperative outcomes.38,39 Also, there may have been some contamination of the CC group, as despite this institution not formally implementing ERPs, certain elements may have been used. We also did not report on any patient-centered outcomes; however, previous work demonstrated no differences in postoperative quality of life with laparoscopy or ERPs for colonic surgery. 16 Finally, this was a single university, dual-institutional perspective from Canada with a modest sample size. While there are significant differences between the Canadian and U.S. healthcare systems, the potential advantages of ERPs and laparoscopy are likely to confer meaningful benefits in increased patient flow, operative capacity, and cost savings regardless of system perspective.
Conclusion
The use of ERPs had an independent impact on reducing LOS after rectal resection, demonstrating its ability to improve on the short-term benefits afforded by laparoscopy. ERPs also had significant benefits in LOS after open rectal surgery, which remains the most prevalent rectal surgery approach. Furthermore, only the combination of laparoscopy and ERPs significantly reduced overall costs compared to when neither strategy was used. Our findings suggest that laparoscopy and ERPs may improve short-term outcomes for patients undergoing rectal resection.
Footnotes
Disclosure Statement
The Steinberg-Bernstein Centre for Minimally-Invasive Surgery is supported by an unrestricted educational grant from Covidien. No other grants or support relevant to this study. Author L.S.F. is a paid consultant for Covidien and receives research support from Ethicon. Author S.L. is a paid speaker and a surgical proctor for Covidien. Author P.C. is on the advisory board for Merck. Authors R.G., M.B., G.G., C.A.V., B.S., and L.L. have no potential conflicts of interests to disclose.