
Abstract
Abstract
Background:
Anatomic segmentectomy for stage I nonsmall cell lung cancer (NSCLC) has potential advantages such as preserving pulmonary function and reducing postoperative complications. However, many surgeons are deterred from this procedure for its anatomical complexity. Therefore, we presented our early experience with video-assisted thoracoscopic surgery (VATS) anatomic segmentectomy compared with our most recent VATS lobectomy cases.
Patients and Methods:
Forty patients with cT1aN0M0 (ground-glass opacity [GGO] rate >50%) NSCLC underwent VATS segmentectomy from January 2015 to December 2016. To compare the short-term postoperative outcomes, 47 patients, who underwent VATS lobectomy for cT1aN0M0 NSCLC (GGO rate ≤50% and pure solid nodule) during the same period, were referred to as a control group.
Results:
The two groups were similar in age, sex, preoperative pulmonary functional assessment, and associated comorbidities. The tumor size in the segmentectomy group was significantly smaller (median, 0.8 cm versus 1.4 cm, P < .001). Segmentectomy and lobectomy groups had similar operating time, estimated blood loss, duration of chest tube drainage, length of postoperative hospital stay, and postoperative major and minor morbidities. With regard to lymph node evaluation, lobectomy was associated with more lymph nodes (median, 12 versus 9 nodes, P < .001) and mediastinal nodal stations evaluated (median, 3 versus 3 stations, P < .001).
Conclusions:
With acceptable morbidity and mortality, VATS segmentectomy may be an acceptable option for the treatment of cT1aN0M0 (GGO rate >50%) NSCLC.
Introduction
A
Despite its advantages in preserving pulmonary function and reducing postoperative complications,9,10 video-assisted thoracoscopic surgery (VATS) segmentectomy is still a highly complex procedure. Confirmation of nodule locations, identification of targeted segmental structures, preservation of intersegmental veins, determination of the surgical margin, and division of the intersegmental plane are all critical for successful anatomic segmentectomy, 11 which make segmentectomy being considered as more challenging than lobectomy. In this article, we present our early experience with VATS segmentectomy for cT1aN0M0 NSCLC with a ground-glass opacity (GGO) rate of more than 50%. Comparison was made with patients undergoing VATS lobectomy for cT1aN0M0 (GGO rate ≤50% and pure solid nodule) during the same period.
Patients and Methods
We retrospectively reviewed a prospectively collected lung cancer database to retrieve 40 consecutive patients with NSCLC undergoing VATS segmentectomy at our institution from January 2015 (when VATS segmentectomy was first adopted) to December 2016. This study was approved by the Institutional Review Board of the Affiliated Jiangning Hospital of Nanjing Medical University. Comparison was made with 47 VATS lobectomies performed for cT1aN0M0 (GGO rate ≤50% and pure solid nodule) during the same period (Fig. 1).

Study profile. GGO, ground-glass opacity; NSCLC, nonsmall cell lung cancer.
All patients were preoperatively evaluated by pulmonary function test with blood gas analysis and contrast-enhanced CT scans of the chest and upper abdomen. For patients in the lobectomy group, positron emission tomography (PET) was performed at the discretion of the individual surgeon, according to patient symptoms and clinical findings (e.g., enlarged lymph nodes on CT scan). However, for the segmentectomy group, PET was not performed. Based on contrast-enhanced CT images, we preoperatively constructed three-dimensional (3D) lung modeling for majority of patients (38/40, 95%) who were scheduled for VATS segmentectomy or lobectomy. 12 Preoperative surgical simulation was performed based on the patient-individual 3D images. During the simulation for VATS segmentectomy, resection lines with a larger surgical margin than the tumor diameter (at least 1 cm or more even for a tumor smaller than 1 cm) were designed for each patient. If it was difficult to preserve the margin in a single segment resection, a combined segmentectomy with the adjacent subsegments would be considered. 13
Additional preoperative investigations (brain magnetic resonance imaging, bone scan, and flexible bronchoscopy) were performed at the discretion of the operating surgeon, according to patient clinical symptoms and radiological findings. Preoperative tissue diagnosis was carried out in selected patients using CT-guided fine-needle aspiration or transbronchial biopsy. In our department, the final extent of lung resection (lobectomy or segmentectomy) was decided according to preoperative examinations (e.g., nodule size, GGO rate, and nodule location) and intraoperative oncologic staging (e.g., macroscopic and microscopic examination of the resection margin and histologic examination of the main nodule and lymph nodes using frozen-section analysis). 8
Our indications for pulmonary segmentectomy included cT1aN0M0 lung cancer and a ground-glass lesion with a GGO rate of more than 50%.14,15 GGO was defined as an area of slight homogeneous increase in density that did not obscure the underlying vascular markings. 16 GGO rate was defined as the percentage of the lesion occupied by GGO as distinct from consolidation or soft tissue attenuation at the maximal dimension of the tumor on thin-section CT. 8 During VATS segmentectomy, conversion to lobectomy was indicated when an invasive carcinoma or a positive hilar or mediastinal lymph node was identified by frozen-section analysis. Patients with lymph node involvement were excluded from the segmentectomy group. In the segmentectomy group, negative surgical margins were intraoperatively confirmed through frozen-section analysis. If positive margins were observed, a combined segmentectomy with the adjacent subsegments or lobectomy was performed to obtain safe surgical margins.
Baseline characteristics and perioperative data were collected: sex, age, body mass index (BMI), smoking status (never smokers were defined as patients who smoked fewer than 100 cigarettes in their lifetime), associated comorbidities, preoperative pulmonary functional assessment, American Society of Anesthesiologists (ASA) physical status classification, tumor size, tumor location, operation time, estimated blood loss, duration of chest drainage, postoperative hospital stay, conversion, postoperative morbidity (graded and classified using the definitions outlined by Seely et al. 17 ), and 30-day operative mortality. Additionally, the number of lymph nodes and mediastinal nodal stations evaluated and pathologic staging according to the TNM classification of the American Joint Commission on Cancer Cancer Staging Manual (7th Edition) were recorded to investigate the pathologic outcomes. 18 The histological classification was determined according to the 2011 IASLC/ATS/ERS classification. 19
Surgical procedure
The operative technique of VATS lobectomy and segmentectomy was similar to our previous report. 12 All operations were performed with the patient in the lateral decubitus position and under general anesthesia with single-lung ventilation. Two ports and a utility incision were used without rib spreading. The first port was the inferior camera port located at the seventh or eighth intercostal space, through which a 30-degree thoracoscope was positioned. The anterior port was usually in the fourth or fifth intercostal space. The third port was usually in the seventh intercostal space in the posterior axillary line.
Preoperative simulation of segmentectomy was performed based on the patient-individual 3D images. During VATS segmentectomy, anatomical excision of one or more pulmonary segments was performed after individual isolation and division of segmental vessels and bronchi. After dissecting the bronchus, the lung on the operating side was reinflated. Pulmonary parenchyma was dissected along the inflation–deflation lines with two to three endoscopic staplers (Ethicon Endo-Surgery, Inc., Cincinnati, OH). In VATS lobectomy, pulmonary vessels, bronchi, and incomplete fissure were divided with an endoscopic stapler (Ethicon Endo-Surgery, Inc.). Systematic lymph node dissection was performed for all cases. One chest tube was used for postoperative drainage in all patients. Epidural analgesia was avoided in all patients. Postoperative pain control was achieved by a combination of intercostal nerve blocks during the operation and postoperative patient-controlled analgesia. Patients were routinely discharged 2 days after chest tube removal.
Statistical analyses
Variables were analyzed as proportions or medians with variability estimates in the form of interquartile ranges (IQRs), as appropriate. Characteristics of patients in the VATS segmentectomy and lobectomy groups were compared using the Mann–Whitney U test for continuous variables and Fisher's exact test and Mann–Whitney U test for categorical variables. All statistical analyses were carried out with the application of SPSS for Mac (version 22.0; IBM, New York), where P < .05 (two-sided) is considered to represent a significant difference.
Results
The preoperative characteristics of patients during this study period are summarized in Table 1. The patients in this cohort study included 26 (29.9%) men and 61 (70.1%) women, of whom 40 (46.0%) underwent VATS segmentectomy and 47 (54.0%) underwent VATS lobectomy.
ASA, American Society of Anesthesiologists; BMI, body mass index; CAD, coronary disease; COPD, chronic obstructive pulmonary disease; CVD, cerebral vascular disease; DLCO, diffusion capacity of the lung for carbon monoxide; FEV1, forced expiratory volume in 1 second; IQR, interquartile range; MVV, maximal voluntary ventilation.
Patient age, sex, preoperative pulmonary functional assessment, smoking status, BMI, associated comorbidities, and ASA were equivalent between the two groups. Table 2 reports the sites of resected segments and lobes. The superior segments of the lower lobes, upper division of the left upper lobe, and the apical segment of the right upper lobe, in decreasing order of frequency, were the most common segmentectomies performed. Subsegmentectomy or combined subsegmentectomies were performed for 5 patients. The right upper lobectomy was the most common lobar resection performed. The median tumor size in the segmentectomy group was smaller at 0.8 cm (IQR, 0.7 to 1.0 cm), compared with 1.4 cm (IQR, 1.0 to 1.8 cm) in the lobectomy group (P < .001).
The nomenclature of subsegments is adopted according to the Japanese Committee on the Nomenclature for Bronchial Branching.
Perioperative outcomes
Perioperative outcomes are shown in Table 3. There were neither 30-day operative mortalities nor conversions from VATS to open operations in both segmentectomy and lobectomy groups. A VATS right upper lobectomy was performed for 1 patient after completing the right apical segmentectomy because an invasive adenocarcinoma was identified by intraoperative frozen-section analysis. The operating time was similar in the lobectomy group and segmentectomy group (median, 150 minutes versus 145 minutes, P = .354). In addition, estimated blood loss, duration of chest tube drainage, and length of postoperative hospital stay were equivalent between the two groups. With regard to lymph node evaluation, lobectomy was associated with more lymph nodes harvested when compared with segmentectomy (median, 12 versus 9 nodes, P < .001). Meanwhile, patients undergoing a lobectomy were likely to have more mediastinal nodal stations dissected (median, 3 versus 3 stations, P < .001).
Conversion from segmentectomy to lobectomy.
AAH, atypical adenomatous hyperplasia; AIS, adenocarcinoma in situ; IQR, interquartile range; MIA, minimally invasive adenocarcinoma.
Histological type showed that the new classification of adenocarcinoma, especially atypical adenomatous hyperplasia (AAH)/adenocarcinoma in situ (AIS)/minimally invasive adenocarcinoma (MIA), was 38 (95.0%) in segmentectomy and 5 (10.6%) in lobectomy, which meant that tumors in the lobectomy group showed more oncologic invasive behavior compared with the segmentectomy group (P < .001). This difference is believed to be principally due to the different surgical indications for segmentectomy and lobectomy. The concordance between clinical and pathologic stages was 93.1%. Pathologic upstaging occurred in 6 patients (12.5%) in the lobectomy group, compared with none (0%) in the segmentectomy group (P = .029). Four patients upstaged due to visceral pleural involvement, with the other two by lymph node involvement.
Postoperative complications
Postoperative major and minor morbidities are summarized in Table 4. The lobectomy group experienced 2 (4.3%) major morbidities versus 0 (0%) in the segmentectomy group (P = .497). One was a prolonged air leakage (longer than 5 days) with a pigtail catheter in place for the management of pneumothorax. The other was a complete right lower lobe atelectasis requiring bronchoscopy. There were 5 (12.5%) minor morbidities in the segmentectomy group compared with 6 (12.8%) in the lobectomy group (P = 1.000). The first 2 patients undergoing a segmentectomy of the left upper division experienced postoperative hemoptysis and were successfully treated with oral tranexamic acid, 3000 mg daily. After reviewing the surgical videos, the observed postoperative hemoptysis was supposed to be related, at least in part, to the division of intersegmental veins that should have been reserved.
Discussion
Lobectomy with mediastinal lymph node dissection remains the standard surgical treatment for stage IA NSCLC. Results of a randomized trial published by the LCSG in 1995 showed that sublobar (segment or wedge) resection for stage I NSCLC did not result in improved morbidity, mortality, or postoperative pulmonary function and was associated with a threefold increase in local recurrence and a trend toward more favorable overall survival after lobectomy, although the difference was not significant. 4 This landmark report has established lobectomy as the gold standard treatment for stage I NSCLC, whereas segmentectomy was considered as a compromised treatment used in patients who had an impaired pulmonary reserve and were not candidates for lobectomy. Improved detection rate of small NSCLC tumors, by advances in high-resolution CT imaging and the availability of low-dose CT screening, 20 has led many surgeons to question the appropriateness of lobectomy for these early stage lung cancers.6,21
A substantial body of research has emerged in the last decade that led many surgeons to reassess the use of anatomic segmentectomy in the management of small peripheral NSCLC. Kodama et al. reported that the oncologic outcome of segmentectomy versus lobectomy is similar in cT1aN0M0 NSCLC patients. 8 Koike et al. published results showing that similar 5-year overall survival and disease-free survival rates, with more preserved postoperative pulmonary function, were observed in patients who underwent limited resection (90.9% segmentectomy) compared with those who underwent lobectomy with 2 cm or less NSCLC. 7 These growing results have led to segmentectomy being reevaluated as an alternative to lobectomy for selected patients with small peripheral NSCLC. As a result, there has been increasing interest in adopting VATS segmentectomy for early stage lung cancer in an attempt to preserve more postoperative pulmonary function; however, it is difficult to perform an accurate VATS segmentectomy because of its anatomical complexity, which has deterred more surgeons from this procedure.
A new classification of lung adenocarcinomas was proposed by the International Association for the Study of Lung Cancer, American Thoracic Society, and European Respiratory Society. 19 In this classification, patients with completely resected noninvasive AAH and AIS and MIA will involve 100% or near-100% disease-specific survival, respectively. 22 In selecting early lung adenocarcinoma candidates for segmentectomy, the preoperative radiologic criteria for noninvasive AAH and AIS and MIA have been realized to be a crucial point. A prospective multi-institutional study (Japan Clinical Oncology Group 0201) has shown that a consolidation/tumor (C/T) ratio on thin-section CT of 0.25 or less in cT1a (2.0 cm) could be used as a radiologic criterion for noninvasive pathology. 14 A postoperative observation study with the same patients (Japan Clinical Oncology Group 0201) found that both radiographic criteria of C/T ratio 0.25 or less in cT1a and C/T 0.5 or less in cT1a-b (3.0 cm) could identify a group of patients with an excellent prognosis, with a 5-year overall survival of ∼97%. 15
Based on these results, we performed segmentectomy for patients with clinical T1aN0M0 lung cancer and a ground-glass lesion showing a 50% or over GGO rate. In this study, two invasive adenocarcinomas were identified by intraoperative frozen-section analysis after completing VATS segmentectomies. One patient who underwent a VATS right apical segmentectomy was converted to lobectomy. The other patient who underwent a VATS left upper division segmentectomy, after confirmation of negative surgical margins and lymph node status through frozen-section analysis, was not converted to lobectomy. We thought that the left upper division segmentectomy could be considered as a lobectomy, given its size and anatomic and functional similarity to the right upper lobe (closely connected with the lingular segment, has venous drainage typically associated with the lingular branch of the pulmonary vein, and discrete arterial branches arising from the main pulmonary artery).
Performing anatomical segmentectomy is considered to be more of a technical challenge for surgeons given the need for thorough familiarity with segmental anatomy to individually isolate and divide the appropriate segmental vessels and bronchi to obtain safe surgical margins. 13 In this initial experience with complete VATS segmentectomy, we have shown that anatomical segmentectomy can be performed safely with similar short-term postoperative outcomes when compared with a similar group of patients with cT1aN0M0 NSCLC undergoing mature VATS lobectomy. Although the two groups were at opposite ends of the learning curve, we thought this comparison was more appropriate compared with segmentectomy by thoracotomy.
When learning a new surgical technique, there is a learning curve that must be overcome. There were many factors that might help us to reduce the learning curve of VATS segmentectomy. First, before and during the procedure of implementing VATS segmentectomy, we made full use of postoperative lobectomy specimens to help us better understand the pulmonary segmental anatomy. In the lobectomy specimens, we carefully mobilized the pulmonary vessels and bronchi to the segmental and subsegmental levels and identified the segmental planes depending on the location of intersegmental veins. With thorough training on these lung specimens, the learning curve might be shortened even if the surgeon has limited prior experience in segmentectomy.
Second, we have used reconstructed 3D images for preoperative surgical simulation for patients who planned to have an anatomic segmentectomy in our institution (Fig. 2). 12 Preoperative reconstructed 3D images can help to locate pulmonary nodules, confirm anatomic variations, and identify targeted segmental anatomic structures and surgical margins. 11 Meanwhile, preoperative simulation with 3D images can help to determine the optimal sequence for dissecting the segmental structures, which can significantly improve the efficiency of operation. According to our data, even early in the surgeon's experience, median operation times of VATS segmentectomy and lobectomy were 145 and 150 minutes, respectively, which may indicate the merit of simulation with 3D images.
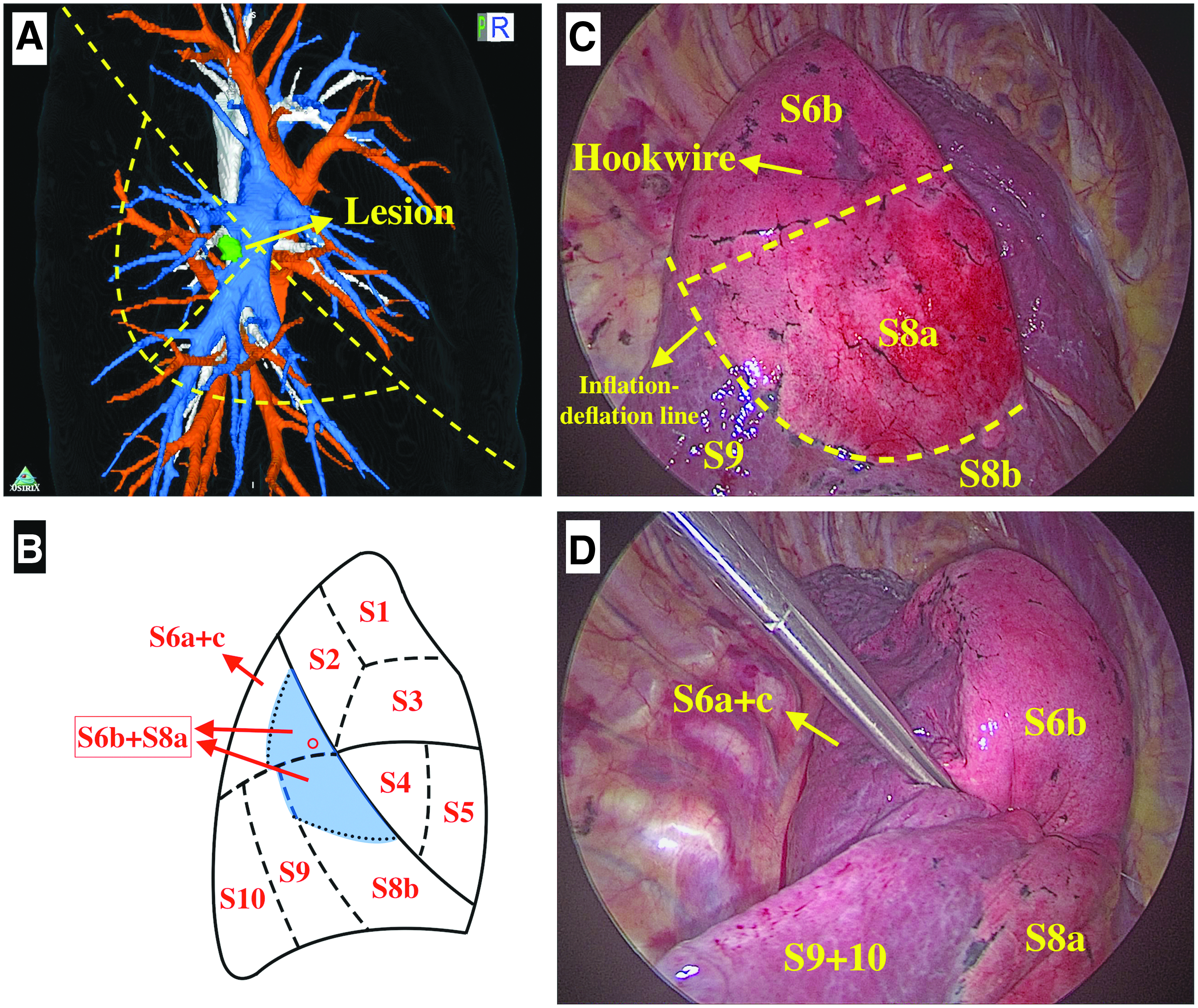
Surgical procedure with the assistance of 3D image navigation.
Adequate lymphadenectomy is an integral component in the surgical management of NSCLC. In addition to potentially understaging patients and failing to identify those eligible for adjuvant therapy, a lack of nodal sampling could potentially influence the outcome of survival and local recurrence with segmentectomy. 23 Stiles et al. reported that selected patients with clinical stage IA peripheral NSCLC undergoing wedge resection with lymph node removal appeared to have better survival and less local and regional disease recurrence than patients without lymph node removal. 24 In this study, systematic lymph node dissection was performed for all cases. However, when compared with lobectomy, segmentectomy was associated with fewer lymph nodes and mediastinal nodal stations evaluated. This difference is believed to be principally due to the smaller specimen obtained during segmentectomy. 25 Another possible reason was that the pulmonary ligament was not routinely dissected in the segmentectomy group and the pulmonary ligament nodes (station 9) were missed.
Limitations
There are a number of potential limitations in this study. First, this was a small-sample retrospective study in a single institution, which may have introduced biases in the selection of a patient for a given procedure. The continuous variables, which were expressed as medians and IQRs in this study, were not normally distributed and compared using the nonparametric Mann–Whitney U test. Use of a Mann–Whitney U test, however, makes an overall comparison of distributions in the two groups and does not specifically test for a difference in means. 26 Moreover, since the VATS segmentectomy group is an early experience, the study lacked adequate power to detect all clinically significant differences between the two groups. Second, in conjunction with short-term postoperative outcomes, oncologic outcomes and survival are necessary in the analysis of any new surgical technique. We acknowledge that the lack of long-term follow-up data limits conclusions that can be drawn from this study. A multicenter, prospective, randomized Japanese study is currently underway (Japan Clinical Oncology Group 0802/West Japan Oncology Group 4607L) to compare the disease-free survival of patients with small (2 cm) peripheral NSCLC undergoing lobectomy versus limited resection (segmentectomy), which will help illuminate the role of segmentectomy in the treatment of small (2 cm) peripheral NSCLC. 27
Conclusions
In conclusion, on the basis of our early experience, VATS segmentectomy may be an acceptable option when an adequate assessment of margin status and lymph node status is made in treating cT1aN0M0 (GGO rate >50%) NSCLC, with acceptable morbidity and mortality. Large-scale randomized studies are needed to validate the utility of VATS segmentectomy.
Footnotes
Acknowledgment
The authors would like to thank Prof. Liang Chen from the First Affiliated Hospital of Nanjing Medical University for providing useful suggestions.
Disclosure Statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.