
Abstract
Abstract
Aim:
To evaluate short-term and long-term outcomes of laparoscopic-assisted transhiatal esophagogastrectomy (LTEG) for treatment of adenocarcinoma of the esophagogastric junction (AEG).
Methods:
Patients with AEG who underwent laparoscopic or open surgery at our department from October 2008 to December 2012 were enrolled in this retrospective study. Patients' demographics, perioperative outcomes, and survival data were collected.
Results:
A total of 136 patients with AEG were enrolled (103 patients underwent laparoscopic surgery and 33 patients underwent open surgery). Patient characteristics were comparable between two groups in terms of age, gender, tumor-node-metastasis stage, tumor size, preoperative complications, and type of surgery. The median operative time was longer in laparoscopic group (240 versus 210 minutes, P = .048). However, the estimated blood loss was less, and the rate of pleural rupture was lower in laparoscopic group (20 versus 70 mL, P < .001 and 18.4% versus 36.4%, P = .033, respectively). The rate of patients with pleural rupture requiring prolonged use of mechanical ventilation longer than 12 hours (6/31, 19.4%) was higher than that of patients without pleural rupture (6/105, 5.7%) (P = .019). The incidence of reflux symptoms at postoperative month six was similar in two groups (18.4% in laparoscopic group versus 24.2% in open group, P = .468), as well as the use of proton pump inhibitors (12.6% versus 15.2%, P = .709). Furthermore, the number of lymph nodes harvested (22 versus 25), 2-year cumulative overall survival rates (80.4% versus 57.5%), and the median survival times (51.52 months versus 24.24 months) were similar between two groups (P > .05).
Conclusion:
LTEG is a safe, feasible, and oncologically effective procedure for AEG when performed by an experienced surgeon. Laparoscopic surgery is associated with a lower risk of pleural rupture, but pleural rupture in laparoscopic surgery may cause an adverse effect on the recovery of pulmonary function presumably due to tension pneumothorax.
Introduction
A
Even though both transhiatal and transthoracic approaches have been widely accepted as treatment modalities for AEG in the past, a growing consensus has been seen in the last decade that transhiatal esophagogastrectomy (TEG) should be the first choice for type II/III AEG with limited involvement of the esophagus (<3 cm).2,3 Laparoscopic surgery has been used for both benign and malignant diseases; laparoscopic-assisted distal gastrectomy (LADG) and total gastrectomy procedures have been widely used for patients with early or advanced gastric cancer, especially in Asian countries where there is a high prevalence of gastric cancer. Compared with open gastrectomy, laparoscopic-assisted gastrectomy was associated with less surgical trauma, shorter hospital stays, and decreasing morbidity and mortality. Hence, LADG has been described as an investigational treatment for early gastric cancer (earlier than T2N1) in the Japanese gastric cancer treatment guideline. However, due to technical difficulty involving intramediastinum manipulation and alimentary reconstruction, few articles have reported the feasibility and safety of laparoscopic esophagogastrectomy with distal esophagectomy and intramediastinum reconstruction for type II/III AEG. Furthermore, literatures focusing on laparoscopic-assisted transhiatal esophagogastrectomy (LTEG) for AEG were all enrolling small study populations. Evidence on its safety, oncological effectiveness, and long-term results is warranted. Here, we report our preliminary results of LTEG compared with open TEG.
Materials and Methods
Patients
From October 2008 to December 2012, 136 consecutive patients diagnosed with AEG at the Department of Gastrointestinal Surgery, West China Hospital, Sichuan University, were enrolled in this retrospective cohort study. All patients underwent TEG, which was performed by an experienced surgeon. Before surgery, all patients received gastroscopy and thoracoabdominal computed tomography (CT) scan. The inclusion criteria for laparoscopic-assisted surgery were as follows: pathologically confirmed adenocarcinoma without distal metastasis such as peritoneum, lung, liver, or bone metastasis. The exclusion criteria were as follows: multiple primary gastric tumors, patients requiring emergency surgery for acute pyloric obstruction, and cases unsuitable for laparoscopic-assisted surgery for any other reason, such as patients had clinical mediastinal lymph node metastasis and needed lower mediastinal lymphadenectomy. Patient demographics, perioperative outcomes, and survival data were collected. Postoperative complications were recorded if they occurred within 90 days after surgery and were stratified according to the Clavien-Dindo classification. Major complications were defined as complications with a grade 3 and higher than the Clavien-Dindo classification. Mortality was recorded if they occurred within 90 days after surgery. Reflux symptoms were diagnosed according to the symptoms and endoscopic findings and were classified using the modified Visick scores (Table 1) at postoperative month six.
Surgical techniques
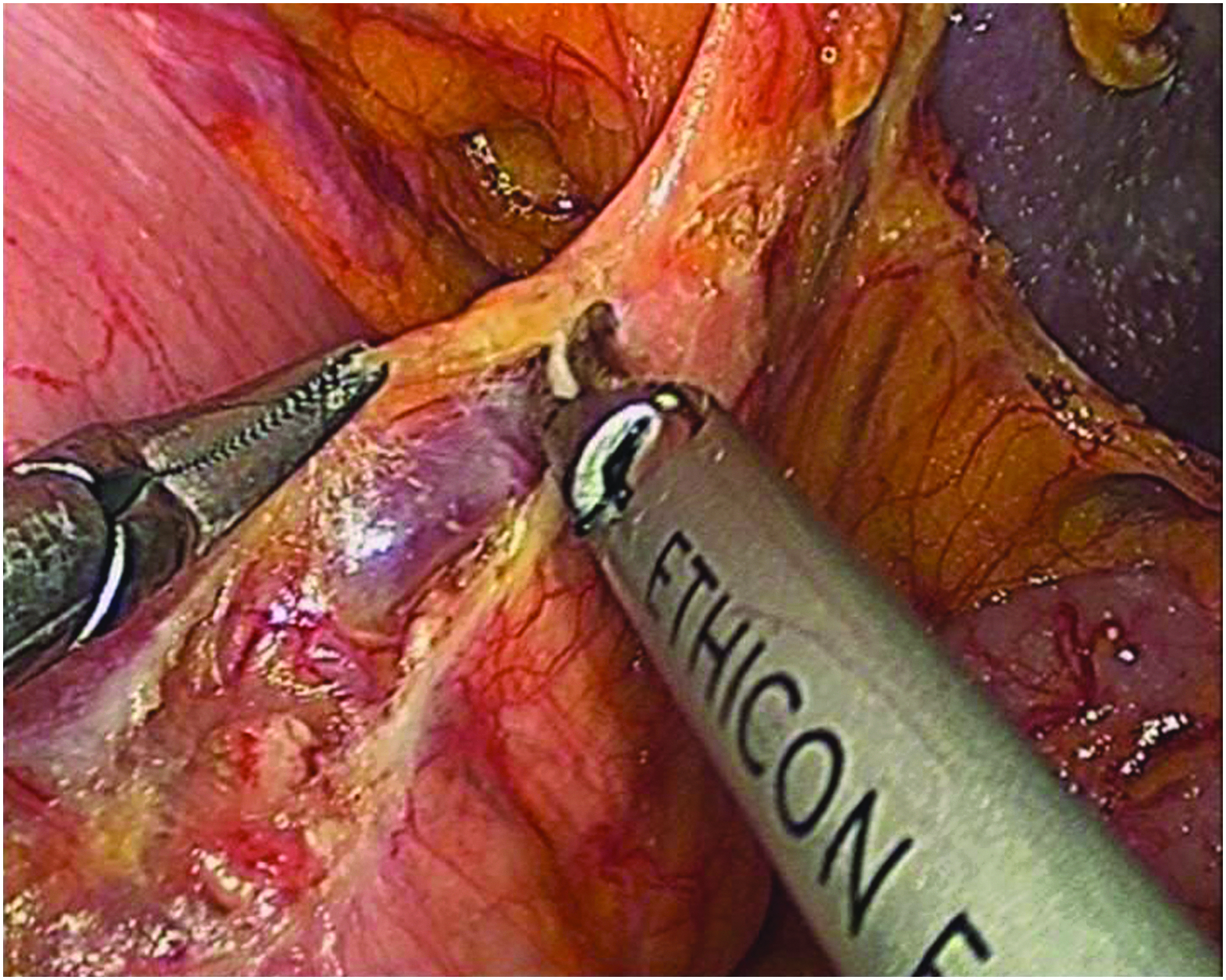
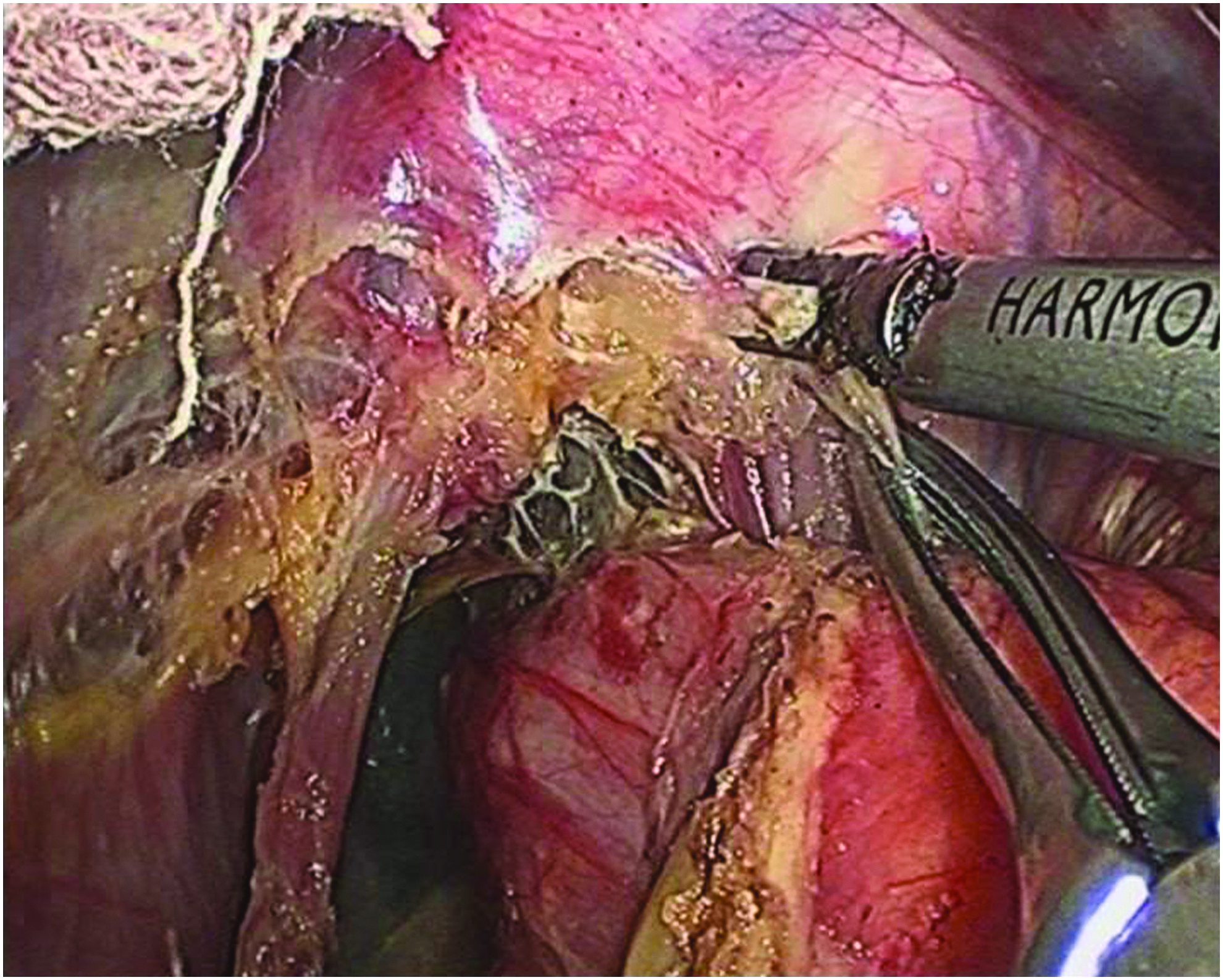
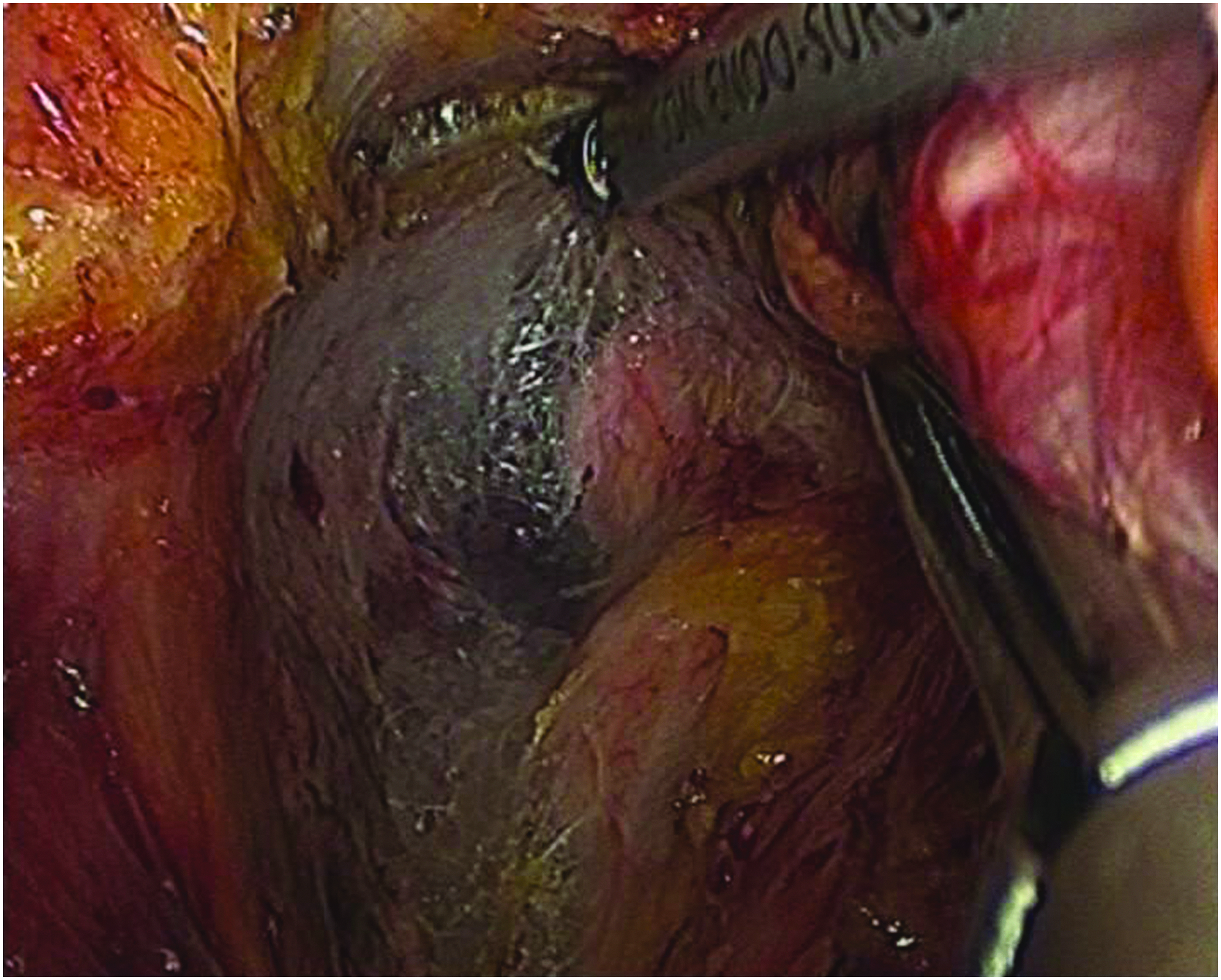
Five ports were used for laparoscopic-assisted surgery. A pneumoperitoneum was created with a pressure of 12–14 mmHg. An ultrasound knife (HARMONIC; Johnson and Johnson) was used for laparoscopic dissection. The surgery procedure was performed as follows: first, the greater omentum was divided from the transverse colon (Fig. 1). Lymph node, No. 4sa, No. 4sb, No. 11d, and No. 10 (in selected cases), dissection was performed by transecting the left gastroepiploic vessels at their origin. Next, the lymph nodes No. 11d and No. 10 were dissected along the splenic artery and vein (Fig. 2). The short gastric vessels were ligated near the splenic artery. The dissection of lymph nodes No. 1–9 and No. 11p was performed as reported previously. Second, a “Y” shaped incision was made in the middle of the diaphragm to enlarge the diaphragmatic hiatus (Fig. 3). Mobilization of the esophagus was gained along the esophageal wall when the lower mediastinal lymph node dissection was not planned. When mediastinal lymphadenectomy was necessary, dissection was usually performed by first separating the lymph adipose tissue from the cardiac capsule (Fig. 4). Extreme caution must be exercised when dissecting along the pleura. The mobilization of the esophagus could usually be performed up to the pulmonary ligament. Third, the esophagogastrostomy or esophagojejunostomy was completed with a circular stapler. The securing of the anvils in the esophagus was performed either by using hand sewn purse string suturing or by a modified double stapling technique. For the latter, the anvil was attached to a suture line with a stitch (Fig. 5). After advancing the anvil into the esophagus, the esophagus was transected with an endoscopic flexible linear stapler. By pulling the suture line, the central rod of the anvil was brought out from the anterior wall of esophagus as shown in Figure 6.

Divided the greater omentum.
Dissected the lymph nodes along the splenic vessels.
Made a “Y” shaped incision in the middle of the diaphragm.
Dissected the mediastinal lymphadenectomy.

Attached the anvil for reconstruction.

Brought the central rod of the anvil out.
Follow-up
All patients were asked to fill out the questionnaire through an outpatient follow-up, telephone follow-up, or mail follow-up every 6 months after surgery. Serial carcinoembryonic antigen testing was performed every 3 months within the first 3 years; abdominal and thoracic CTs were performed every year; and gastric endoscopy was performed every 1 year within the first 2 years after surgery and then every 2 years. All patients were followed up until April 2014. The patient follow-up rate was 94.12% (128/136). One patient was lost according to the last follow-up calculation. Patients lost to follow-up not due to AEG were evaluated as censored data.
Analyses
SPSS 20.0 (Chicago, IL) for windows was used for statistical analyses. The categorical variables were analyzed by the chi-squared or Fisher's exact probability test. The continuous variables were compared by the Mann-Whitney U test. In addition, the Kaplan-Meier univariate analysis was used to compare the 2-year cumulative overall survival rates, as well as the median survival time between the two groups. P value <.05 was considered to be statistically significant.
Results
A total of 136 consecutive patients with AEG were enrolled in this study. Among them, 103 patients underwent laparoscopic surgery (laparoscopic group), while the other 33 patients underwent open surgery (open group). Laparoscopic surgery was performed successfully in 99 patients, while the other four patients (3.9%) were converted to open surgery. Of the four patients, three were due to severe adhesions, and one was due to bleeding that occurred when we dissected around the left gastric vascular under laparoscopy. The clinical characteristics of the two groups are shown in Table 2. There were no significant differences in age, gender, tumor-node-metastasis stage, tumor size, preoperative complications, or type of surgery between the two groups.
TNM, tumor-node-metastasis.
The perioperative outcomes of the two groups are shown in Table 3. The median operative time was longer in laparoscopic group (240 versus 210 minutes, P = .048). However, estimated blood loss and the rate of pleural rupture were less in laparoscopic group (20 versus 70 mL, P < .001 and 18.4% versus 36.4%, P = .033, respectively). No differences were observed between the two groups in terms of lymph nodes harvested, time in intensive care unit (ICU), time with ventilator and oxygen, or need for ICU stay and ventilator. Postoperative complications were comparable between two groups (17.1% in laparoscopic group versus 9.1% in open group, P = .246), as well as major complications (4.9% versus 0.0%, P = .199). There was no mortality in either group.
Major complications were defined as complications with a grade 3 and higher of the Clavien-Dindo classification.
ICU, intensive care unit.
Table 4 shows the situation in patients with pleural rupture. Although no significant difference was observed, patients with pleural rupture in laparoscopic group were more likely to be admitted to the ICU after surgery compared with that in open group (31.6% versus 8.3%, P = .201). In addition, 19.4% of patients (6/31) with pleural rupture required a prolonged use of mechanical ventilation, longer than 12 hours, compared with 5.7% of patients without pleural rupture (P = .019) (Table 5). The incidence of reflux symptoms at postoperative month six was similar in two groups (18.4% in laparoscopic group versus 24.2% in open group, P = .468), as well as the use of proton pump inhibitors (12.6% versus 15.2%, P = .709) (Table 6).
ICU, intensive care unit.
PPI, proton pump inhibitors.
Subgroup analysis was conducted according to type of surgery (Table 7). The operative time of partial gastrectomy was similar between two groups, while operative time of total gastrectomy was longer in laparoscopic group (270 versus 235 minutes, P = .045). Estimated blood loss of partial and total gastrectomy was less in laparoscopic group (20 versus 70, P < .001 and 20 versus 75, P = .001, respectively). In addition, the rate of pleural rupture was lower in laparoscopic group (8.8% versus 30.4%, P = .035) for partial gastrectomy, but it was comparable between two groups for total gastrectomy.
Major complications were defined as complications with a grade 3 and higher of the Clavien-Dindo classification.
PPI, proton pump inhibitors; ICU, intensive care unit.
After a mean follow-up period of 29 months, 51 patients died and 8 patients had recurrence. Kaplan-Meier analysis showed that there were no significant differences in 2-year cumulative overall survival rates between the two groups (80.4% versus 57.5%, P > .05) (Fig. 7).

Cumulative survival curve of patients undergoing laparoscopy and open surgery for adenocarcinoma of the esophagogastric junction. The two groups did not differ significantly (80.4% versus 57.5%, P = .11).
Discussion
A TEG refers to a procedure that includes opening of the hiatus and performing a distal esophagectomy with lymph node dissection in the posterior mediastinum following stomach mobilization and abdominal lymphadenectomy. 4 The JCOG9502 study in Japan showed that TEG could achieve better long-term outcomes and lower postoperative complications compared with thoracolaparotomy for AEG. An increasing number of studies have considered TEG as a mainstream surgical procedure in recent years.5–8 As for laparoscopic surgery, laparoscopic distal, proximal, and total gastrectomy have been reported as safe, feasible, and effective treatments in the management of both benign and malignant tumors. Costi 9 first performed a total LTEG without thoracic or cervical access in a patient with Siewert type II adenocarcinoma. After that, the feasibility and safety of LTEG have been further demonstrated by several other authors. 1 Kinoshita et al. 10 and Bann et al. 11 showed that laparoscopy was superior to laparotomy with regard to blood loss, postoperative gastrointestinal functional recovery, hospital stay, and postoperative complications. However, the number of cases of those studies was very small. Even the largest case series only enrolled 32 cases reported by Palanivelu 12 from India. Therefore, the effectiveness of LTEG in long-term and oncologic outcomes remains debatable. Here, we report our preliminary results of 103 consecutive cases of AEG who underwent LTEG. To the best of our knowledge, this study represents the largest series of cases to date.
Laparoscopic-assisted intramediastinal dissection of the distal esophagus, alimentary tract reconstruction, as well as lower mediastinum lymphadenectomy (which is considered to be the most challenging part) could be safely completed intracorporeally. The four cases of conversion were not due to technical difficulty of the intramediastinal dissection. We generally avoid the pleura to the best of our ability when performing the esophagus dissection or lymphadenectomy. When pleural rupture occurred, the defect was repaired if it was possible. This prevented chest infection and provided a timely healing in three of the four patients who developed leakage. These patients were successfully managed conservatively, with a healing time of 14–30 days. The operative time was significantly longer and the mean blood loss was significantly less in the laparoscopic group. The other postoperative short-term outcomes, including gastrointestinal function recovery, hospital stay, analgesic use, and ICU stay, were all comparable between the two groups. Hulscher et al. 13 also showed that a transhiatal procedure was associated with significantly fewer pulmonary complications (27% versus 57%) and chylous leakages (14% versus 16%).When compared with thoracoscopic combined Ivor-Lewis surgery or laparoscopic transhiatal esophagectomy with cervical access, this method showed favorable postoperative morbidity and mortality.
In terms of cancer clearance, a clear resection margin was achieved in all but one patient in the laparoscopic group. During follow-up, two anastomotic recurrences were confirmed (one in laparoscopic group and one in open group). Therefore, our study suggested that LTEG could provide a sufficient proximal resection margin for most type II or III AEG patients, which is similar to the results of clinical trial JCOG9502 (which advocates performing a transhiatal esophagogastrectomy for AEG with an esophageal invasion of <3 cm).
Lee et al. 14 reported that the number of lymph nodes harvested in open surgery was more than that in laparoscopic surgery. However, Tanimura et al. 15 believed that the number of dissected lymph nodes was comparable between traditional laparotomy and laparoscopic groups. In our study, a mean of 22 lymph nodes were retrieved in the laparoscopic group, which was comparable to its open counterpart and met the requirement of retrieving at least 15 lymph nodes for gastric cancer. The number of lymph nodes may not only reflect the radical degree of tumor but also act as a significant prognostic parameter. Although there was no significant difference, the 2-year cumulative overall survival was higher in laparoscopic group (80.4%) than that in open group (57.5%). In addition, a stage-to-stage analysis also showed no difference in the survival rates between the two groups. The 2-year cumulative overall survival rate of the laparoscopic group was comparable to that of other large case studies, including 74.4% in JCOG9502 and 72.9% in a study presented by Yamashita. 16 LTEG, however, was not recommended to treat squamous cell carcinoma, which had multiple lesions with upper/middle mediastinum lymph node metastases.
The most common intraoperative complication in both groups was pleural rupture, which primarily occurred during intramediastinal lymphadenectomy. In our series, pleural rupture occurred in 18.4% of patients in laparoscopic group and 36.4% in open group (P = .033). Patients in laparoscopic group had lower risk of pleural rupture, which was attributed to better exposure in laparoscopy. However, a higher rate of ICU admittance (nonsignificant) and prolonged mechanical ventilation among patients with pleural rupture were observed in laparoscopic group. Although this complication did not increase pulmonary infection rates and postoperative mortality, it was found to raise the rate of prolonged mechanical ventilation over a 12-hour period (19.4% in ruptured group versus 5.7% in nonruptured group). Accordingly, our finding indicated that pleural rupture and subsequent hypertension in the pleural cavity had an adverse effect on intraoperative and postoperative pulmonary function. Pleural rupture during laparoscopic surgery may cause higher airway pressure and decreased arterial oxygen saturation, observed in at least four patients in our series, which could be successfully corrected by the use of positive end expiratory pressure (PEEP). 2 However, the adverse effects on postoperative pulmonary function recovery are still worthy of attention.
Given that pleural rupture mostly occurred during intracorporeal mediastinal lymphadenectomy, there is still controversy on whether laparoscopy could be routinely used in lower mediastinal lymphadenectomy. In this study, the rate of pleural rupture was lower in laparoscopic group, which was attributed to the chief surgeon's adept technique. The optimal extent of mediastinal lymphadenectomy for Siewert type II or III AEG also remains controversial. Although in patients with Siewert type II or III tumor, lower mediastinal paraesophageal nodal involvement (level 8, 9) was reported to be 8%–15%, nodal metastases to the upper or middle mediastinum were relatively rare. 1 Therefore, routine dissection of this area seems to be unnecessary. However, it had been widely accepted that dissection of the mediastinal lymph nodes is necessary if the involved length of the esophagus above the esophagogastric junction is more than 1 cm. 17 In addition, others argued that mediastinal lymphatic spread in patients with type II and III tumors was a late finding and dissection of lymph nodes Nos. 111 and 112 did not improve survival rate.3,4 If dissection of mediastinal lymph nodes was performed in Siewert type II or III tumor with the involved length of the esophagus more than 1 cm, open TEG should be considered as the first choice. Laparoscopic surgery is not appropriate for patients with pulmonary dysfunction. If pleural rupture occurred during operation, lowering the pressure of the pneumoperitoneum associated with PEEP and timely repairing of the defect could decrease stress on the lung. After completion of the surgery, attention must be paid to deflate the pleural cavity thoroughly and insert a temporary catheter if it is necessary.
Conclusion
LTEG is a safe, feasible, and oncologically effective procedure for AEG when performed by experienced surgeons. Although laparoscopic surgery is associated with a lower risk of pleural rupture, pleural rupture in laparoscopic surgery might have an adverse impact on the recovery of pulmonary function, presumably due to tension pneumothorax. Considering that lower mediastinal lymphadenectomy frequently causes pleural injury, LTEG should be avoided for AEG patients with long esophageal invasion when a lower mediastinal lymphadenectomy is needed. Large-scale trials in selected patients are needed to further define the role of this technique.
Footnotes
Disclosure Statement
No competing financial interests exist.