
Abstract
Abstract
Background:
Intracorporeal anastomosis (IA) in right colectomies shows many advantages over extracorporeal anastomosis (EA). Many difficulties encountered in laparoscopic IA can be overcome with hybrid robot-assisted IA or recently with totally robotic procedures. In the literature, few works have been published comparing laparoscopic, hybrid, and totally robotic right colectomies. The aim of this study is to retrospectively analyze the improvements brought on by the evolution of robotic surgery at our specialized center.
Materials and Methods:
Two hundred six (hybrid and totally) robotic right colectomies (RRCs) with IA were compared with 160 laparoscopic right colectomies (LRCs) with EA. A separate analysis carried out by the robotic group compared 30 totally robotic right colectomies (TRRCs) with 176 hybrid robot-assisted right colectomies (HRRCs). Demographics, pathological features, operative details, and postoperative outcomes were retrospectively analyzed from a prospectively maintained database.
Results:
The groups were comparable with respect to demographics and tumor staging. When compared with LRC, RRC showed shorter time to first flatus (P < .001), stools (P < .001), solid diet (P < .001), and discharge (P < .001). The number of lymph nodes harvested was 23.13 ± 11.2 in RRC versus 20.5 ± 11.2 in LRC (P = .031). Operative time was longer in RRC (253.0 ± 47 minutes versus 209.9 ± 64 minutes; P < .001), but conversion to open (2.4% versus 18.1%; P < .001), anastomotic leaks (0.5% versus 5%; P = .012), and bleeding (0.3% versus 4.4%; P = .024) were significantly less frequent. Subsequent analysis shows no significant increase in operative time in TRRC versus HRRC (261.0 ± 41 minutes versus 251.6 ± 47.6 minutes; P = .310). Even if not statistically significant, TRRC showed faster bowel function recovery and tolerance to solid diet.
Conclusions:
We confirmed the clinical advantages of RRC with IA over LRC with EA in postoperative recovery outcomes and complication rate. Furthermore, our preliminary analysis in a cohort of 30 TRRC shows promising results.
Introduction
C
The introduction of robotic surgery reduces most of these technical limitations, providing 3D vision, allowing higher degrees of freedom motion in anatomically challenging sites and permitting high-precision dissection and suturing.5–7 The first robotic models were used in a hybrid (or robot-assisted) way, just for the most challenging tasks, such as IA. The introduction of the da Vinci Xi® Surgical System (Intuitive Surgical®, Sunnyvale, CA), permitting a multiquadrant surgery, solves some of the limitations of the previous models. In right colectomies, this leads to the adoption of laparoscopic procedures with robot-assisted IA only, to a fully robotic approach, even if few cases have been reported to date.
Some evidence can be found in studies comparing the most commonly practiced laparoscopic right colectomy (LRC) with EA with LRC with robot-assisted IA. In our previous study we compared 48 LRCs with EA with 48 LRCs with robot-assisted IA. We found a significant reduction in the recovery of bowel function, length of hospital stay, and postoperative complications (anastomotic leaks or twist and incisional hernia) in the robot-assisted group. 8
After the introduction of totally robotic procedures at our center, we decided to analyze the results of our first 30 totally robotic right colectomies (TRRCs) with IA, comparing them with our previous laparoscopic with EA (LRC) and hybrid robot-assisted right colectomies (HRRCs).
The aim of this study is to confirm the clinical advantages of RRC with IA over LRC with EA as previously reported, but in a bigger pool of patients, and to evaluate whether standardized TRRCs for cancer have any advantages over HRRCs.
Materials and Methods
Between January 1998 and June 2017, a consecutive unselected series of 1240 patients underwent minimally invasive colorectal surgery at our institute and data were entered into the institutional prospectively maintained database (Fig. 1).
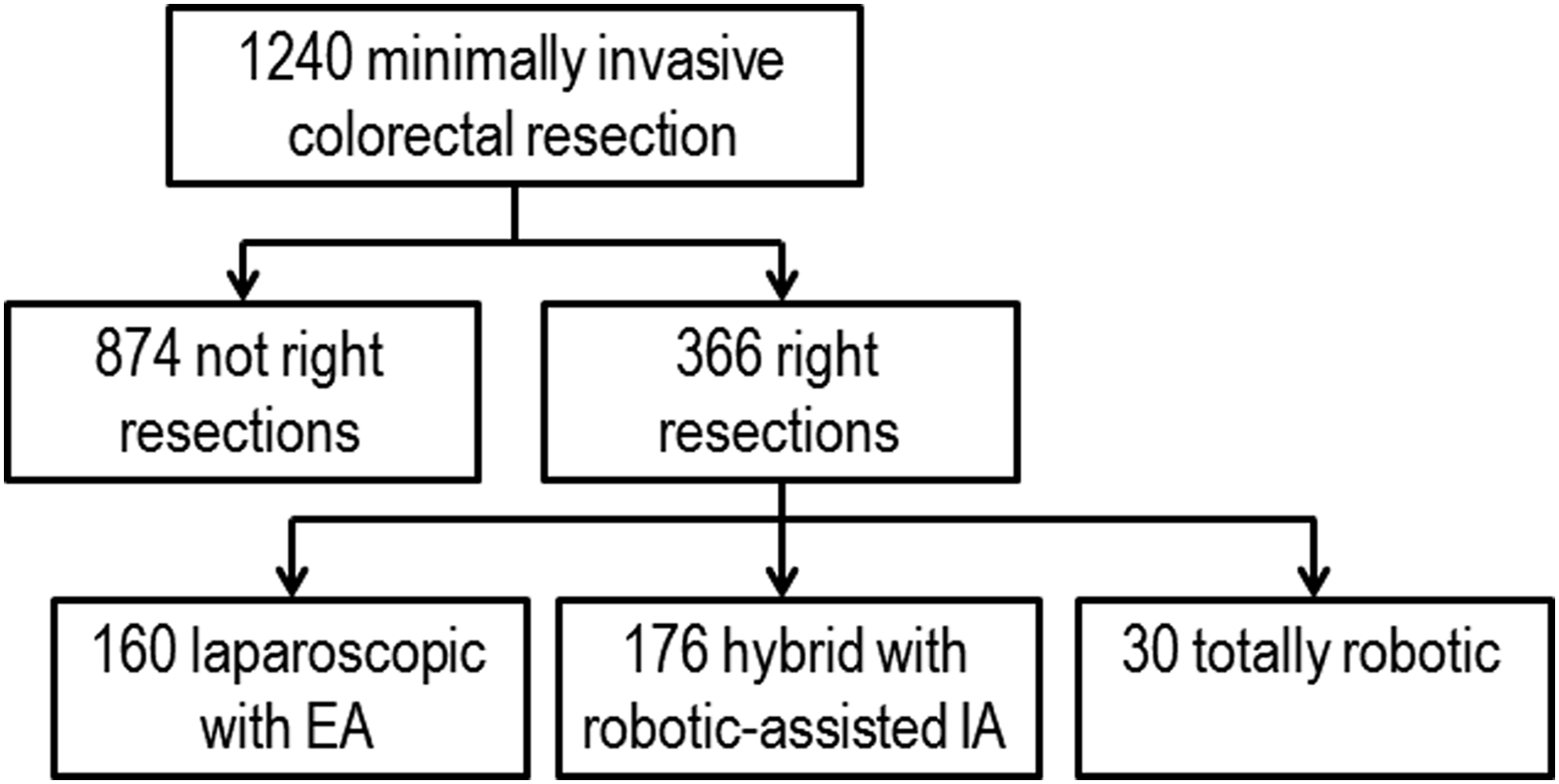
Diagram of patients submitted to minimally invasive colorectal resections between January 1998 and June 2017 at our center.
A series of 366 patients underwent right colectomy for cancer. Of these, 160 were LRCs with extracorporeal anastomosis (between 1998 and 2017). Robotic surgery was first introduced in 2001 at our institute with the adoption of the da Vinci S® surgical system. From June 2009 to December 2015, a series of 176 patients underwent a standardized hybrid right colectomy with laparoscopic vascular control, bowel division, and robot-assisted IA. Since January 2016, the new da Vinci Xi replaced the previous surgical system and a totally robotic approach was offered to all patients who needed a right colectomy and were suitable for a minimally invasive approach, for a total of 30 patients at the time of the present study.
There were no planned selection criteria for each surgery. The choice between different approaches was simply chronological. Before the introduction of the da Vinci Xi, right colectomies were performed either in a robotic or laparoscopic way, depending on the availability of the robotic operating theater. With the introduction of the da Vinci Xi TRRC was the technique of choice (laparoscopic procedures were no longer performed).
Inclusion criteria were as follows: age ≥18, preoperative histological diagnosis of neoplasm (adenoma, carcinoma, other) of the right colon (cecum, ascending, right flexure, right transverse) and having undergone laparoscopic with EA, HRRC or TRRC with IA. Exclusion criteria included: patients <18, emergency procedures, and association with other major surgical procedures (such as hepatic resection).
We retrospectively analyzed data that included demographics, surgical history, body mass index, ASA score, localization of the tumor, pathologic features (size of specimen, distance of neoplasm from proximal and distal margins, number of lymph nodes harvested, staging), operative characteristics (time, conversion, intraoperative complications, estimated blood loss), and postoperative data (recovery of bowel function, time to first oral intake, hospital stay, medical and surgical postoperative 30-day complications, 30-day mortality, reoperation rate, and number of intraoperative and postoperative blood transfusions). Complications presented more than 30 days after surgery were recorded from follow-up documents or phone interviews, if needed.
No patient underwent mechanical bowel preparation. All patients were treated with short-term prophylactic antibiotics at the beginning of surgery (cefoxitin 2 g). A nasogastric tube and a urinary catheter were put in place after the induction of general anesthesia. In the absence of specific contraindications, the nasogastric tube was routinely removed immediately after surgery and the urinary catheter after 2 days, following the departmental protocol. A semiliquid diet was allowed after the first passage of flatus, followed by a regular diet as tolerated. Patients were discharged when fully functional.
For statistical analysis, continuous variables were expressed as mean ± SD and analyzed with the Student t-test, while categorical variables were expressed as percentage value and analyzed with chi-square or Fisher's tests, when appropriate. A P value below .05 was considered significant. Data analysis was conducted using SPSS software version 22.0 (IBM Corporation, Armonk, NY). Ethics committee approval was obtained according to the Italian law.
Surgical techniques included a standardized four-port medial-to-lateral laparoscopic with EA, the hybrid robotic, and the TRRC, as summarized in the following steps.
Surgical technique
TRRC with IA
The patient was in a supine position with both arms along the body. A left periumbilical 8-mm Hasson camera port was inserted. Three other 8-, 8-, and 12-mm ports were inserted in a line in the left abdominal side under direct vision (Fig. 2). The distance between each trocar along the line was of ∼8 cm. A 12-mm AirSeal® working trocar was inserted for the bedside assistant in the left flank.
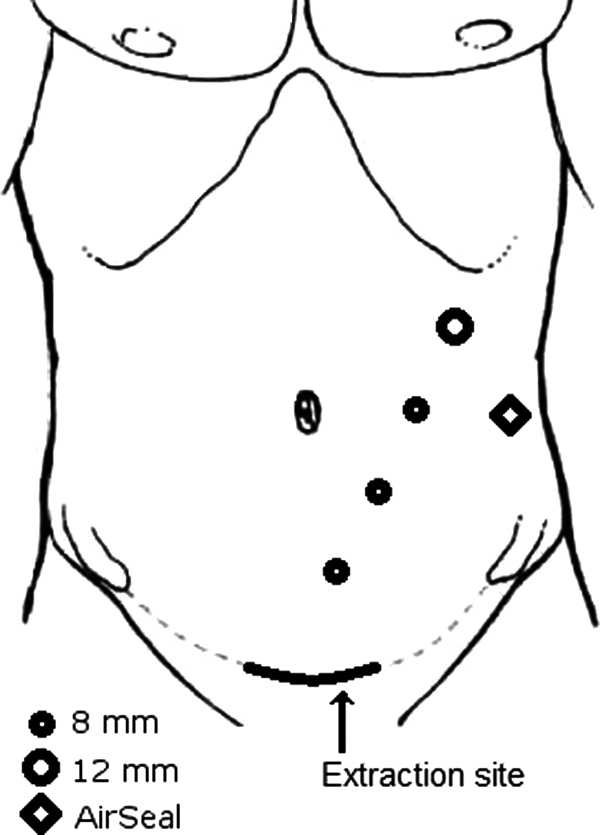
Port placement for da Vinci Xi® totally robotic right colectomy.
Laparoscopic exploration of the abdominal cavity was carried out to rule out peritoneal seeding or liver metastasis. The robot was then docked from the right side of the patient and targeted at the hepatic flexure. The three working arms carried two Cadiere's fenestrated forceps (one for static traction, one for dynamic traction) and a monopolar cautery hook. The peritoneum was opened just below the prominence of the ileocolic vessels and along the anterior aspect of the superior mesenteric vein. The ileocolic vessels were then isolated, clipped, and divided at the origin. The mesentery and the right colon were sharply dissected medial-to-lateral from the urogenital plane, the duodenum, and the head of the pancreas. The right colic vessels (if present), the right branch of the middle colic vessels, or the middle colic vessels if necessary were divided at their origin.
The omentum was then divided at the middle third of the transverse colon. After the gastrocolic ligament division, the right flexure was finally taken down, the bowel transected with a robotic linear stapler, and the two stumps oversewn with a 3/0 glycolic acid absorbable monofilament (Assufil®—Assut Europe SpA). The terminal ileum and the transverse colon were aligned side-by-side with a robotic stay suture, two enterotomies were performed, and the jaws of the robotic stapler were introduced in the viscera (the jaw with the staple cartridge in the colon). An isoperistaltic lateral to lateral anastomosis was performed with the robotic stapler and the enterostomies closed together with an Assufil 3/0 double-layer running suture. The mesentery defect was sutured at its base. The robot was undocked, and the specimen extracted via a protected muscle-splitting mini-Pfannenstiel incision.
HRRC with IA
We previously reported the procedural steps of an HRRC. 8 Briefly, the exploration, vessel isolation and division, medial-to-lateral dissection, and complete bowel detachment were performed in a laparoscopic way. Bowel transection was performed with a laparoscopic Endo-GIA. The da Vinci S was then docked to facilitate stump oversuture, their juxtaposition, the introduction of the laparoscopic Endo-GIA through the enterotomies, and their closure with a double-layer running suture. The mesentery defect was sutured at its base and the specimen extracted via a mini-Pfannenstiel incision.
Laparoscopic right hemicolectomy
In the laparoscopic group, the transverse colon was further mobilized to exteriorize the bowel through a periumbilical incision (rarely through a Pfannenstiel). The terminal ileum and the transverse colon were divided extracorporeally, the stump oversewn, and a hand-sewn double-layer lateral anastomosis performed. The mesentery defect was sutured only if its base could be exposed and was visible from the incision.
Results
Extracorporeal versus intracorporeal robotic anastomosis
There was no significant difference between EA and robotic IA groups in terms of demographics and cancer characteristics, except for a slight difference in the mean cancer stage (stage 2.2 ± 1.0 in EA versus 2.0 ± 1.2 in IA, P = .039) (Table 1). Operative results and short-term outcomes are shown in Table 2. Operative time (including the docking time in the robotic cohort) was significantly longer in the robotic IA group but conversion to open surgery was significantly less frequent. Both groups achieved an adequate number of lymph nodes harvested and margins of resection from the tumor. The number of lymph nodes harvested was greater in RRC (P = .031). Timing to first flatus, stools, diet, and discharge were significantly shorter in the robotic IA group.
The values are in mean (SD) or n (%).
BMI, body mass index; EA, extracorporeal anastomosis; IA, intracorporeal anastomosis; LRC, laparoscopic right colectomy; SD, standard deviation.
The values are in mean (SD) or n (%). Bold indicates statistical significance.
EA, extracorporeal anastomosis; IA, intracorporeal anastomosis; LN/LS, lymph node to length of surgical specimen ratio; LRC, laparoscopic right colectomy; SD, standard deviation.
The mean follow-up was of 19.0 ± 23.4 months for the EA and 6.2 ± 14.1 months for the robotic IA group. Table 3 shows postoperative complications. Anastomotic leaks were significantly less frequent in the robotic group, with a percentage of 0.5% versus 5%. Similarly, intraperitoneal, anastomotic, or systemic bleeding was significantly less frequent in the robotic group. Other postoperative complications showed similar frequencies.
The values are in n (%). Bold indicates significant values.
Pulmonary, cardiac, thromboembolic, septic complications.
EA, extracorporeal anastomosis; IA, intracorporeal anastomosis; LRC, laparoscopic right colectomy.
HRRC versus TRRC
Demographics and pathological data were similar between groups. Operative results and complications are summarized in Table 4. TRRC added no significant increase in the operative time. Even if not significant, TRRC showed a quicker bowel function recovery and shorter time to diet intake. Postoperative complications and oncologic results were comparable between groups.
The values are in mean (SD) or n (%). Bold indicates significant values.
Pulmonary, cardiac, thromboembolic, septic complications.
LN/LS, lymph node to length of surgical specimen ratio; SD, standard deviation.
Discussion
This is a retrospective single-center study analyzing the short-term outcomes of LRC with EA, and HRRC and TRRC with IA. First, we compared the laparoscopic with the robotic group (hybrid+totally robotic) to confirm what we and others previously reported about the advantages of IA over EA. Then, we analyzed the results of our first 30 TRRCs compared with the HRRCs. The safety and feasibility of all considered approaches are well demonstrated by operative and short-term results in our series.
The comparison between IA and EA shows the most significant results. IA in our series has a clear impact on short-term postoperative outcomes, such as a faster recovery of bowel function. The RRC with IA group had a slight reduction in time to passage of first flatus (14 hours less, P < .001), time to first stools expulsion (∼1 day less, P < .001), and time to solid food intake (14 hours less, P < .01).
The length of postoperative stay (9.9 ± 7.1 in LRC with EA versus 7.9 ± 3.5 in RRC with IA, P < .001) is mostly due to social issues rather than clinical issues. RRC had a reduction in the length of hospital stay (2 days less), related to the shorter duration of postoperative ileus and also to the gradual changes in the department discharge protocols. Shorter ileus can be explained by the reduced manipulation of the colon and by the reduced traction of the mesocolon that are made possible by IA. Indeed, the most relevant advantage is represented by the remarkable reduction in anastomotic complications (leaks and twists: 5% in EA; 0.5% in robotic IA group, P = .012).
Conversion to open was significantly lower in the robotic group, with a percentage of 2.4% versus 18.1% in the laparoscopic group. As reported in Table 5, the most frequent causes of conversion in the laparoscopic group were the presence of locally advanced cancers and abdominal adhesions. First, this reflects a learning curve effect, as most laparoscopic resections were performed in the initial phases of our mini-invasive experience. Gaining proficiency, an increasing number of advanced cancers could be totally resected with a mini-invasive approach. This consideration is confirmed by a similar number of stage 3–4 cancers between LRC and RRC.
The values are in n (%).
EA, extracorporeal anastomosis; IA, intracorporeal anastomosis; LRC, laparoscopic right colectomy.
Second, the different conversion rate between groups could be partially explained by our choice to routinely perform a laparoscopic abdominal exploration even in suspected advanced cases or in previously operated patients, not clearly fitting for mini-invasive approach. Anyway, our conversion rate is consistent with other studies published in the literature, which reported a conversion rate between 0% and 8.3% in RRC and smaller than the corresponding laparoscopic group in every case.6,7,9–11
Operative time was significantly longer in the robotic group; however, it was within the mean range reported in the literature (190.2–287.4 minutes).6,7,9–11
Short-term benefits of IA have been previously reported and are likely to be related to less surgical trauma to the bowel. IA avoids the extensive transverse colon mobilization and mesenteric traction required to exteriorize the bowel and to perform the anastomosis through minilaparotomy. This allows a quicker recovery of bowel function, a shorter and alternative incision site for specimen extraction (such as a Pfannenstiel incision or a McBurney incision), and a decreased need for analgesic drugs.5,7,12,13 Another big advantage of IA derives from the direct vision of the mesentery, which prevents anastomotic and mesentery twist, a dangerous occurrence on which we previously reported. 8
Two recent meta-analyses compared IA and EA in 1957 and 1492 patients, respectively, submitted to LRCs, in terms of intraoperative and postoperative outcomes.2,3 Both meta-analyses showed shorter time to first defecation, shorter time to diet, and shorter length of hospital stay in the IA group. One of the two showed additional reduction of short-term morbidity and surgical-site infection in the IA group. No differences were found for anastomotic leakage, operative time, conversion, lymph nodes harvested, ileus, intra-abdominal abscess, hernia, and mortality.
Therefore Trastulli et al. properly noticed that better postoperative short-term results may be related to the performance of an IA rather than to the use of the robot itself. 7 In a retrospective multicenter study, they compared RRC-IA with either LRC-IA or LRC-EA in 236 patients. They found clear advantages of RRC-IA over LRC-EA, but when comparing RRC-IA with LRC-IA, the first group showed better results only in the time to first flatus (2 days versus 4 days), but no significant difference in the length of hospital stay, conversion rate, postoperative complications such as anastomotic leakage, wound infections, reoperations, and mortality. The authors conclude that RRC-IA does not offer significant advantages compared with LRC-IA.
In 2012, Park et al. published the only randomized clinical trial comparing RRC and LRC 10 ; they found no benefit in the use of robotics, however, as noted by others, 7 a big limitation was that both laparoscopic and robotic cases received mixed IA or extracorporeal anastomosis.
The lack of the laparoscopic IA group represents a big limitation of our study. Nevertheless, apart from Trastulli's analysis, 7 evidence that compares RRC-IA with LRC-IA is lacking. The reason for this is that many surgeons who used to perform EA have an incentive to switch to IA only when da Vinci devices become available at their institution. On the contrary, surgeons who already have access to a robotic system tend not to renounce its convenience and dexterity in favor of laparoscopy. This is particularly true with the most recent da Vinci Xi robotic system (Intuitive Surgical), which solves some of the limitations of previous models.
After FDA approval, the da Vinci® surgical system produced different models. The da Vinci Standard®, S and Si represent a continuous evolution of a robotic system designed to work in a narrow space (such as the pelvis) and in procedures that do not require frequent change of the operative field. These models have robotic arms diverging from a common central column and a system of joints that makes instruments converge to a narrow targeted anatomical area.
The relative position of the cart column and the patient is well established and critical to obtain a correct positioning of the robot. Such configuration requires a port placement in a semicircular manner with a distance of at least 8 cm in between each other and does not allow the arms to work in a parallel way. If the surgical procedure requires an extension beyond the targeted anatomy, such as in colorectal resections, a new docking procedure is needed to avoid frequent robotic arm collisions. Furthermore, the use of the fourth arm is troublesome as it accentuates the conflicts between arms. The last disadvantage is the lack of intracorporeal robotic staplers.
Because of these limitations, TRRCs using the da Vinci S were excluded at our center and the robot was exclusively used in a hybrid way to perform the most demanding tasks, such as the IA. The da Vinci Xi represents a great evolution in multiple quadrant surgery. Thanks to a rotating column the chart can be placed in any position relative to the patient and still be set to the targeted anatomy. This feature allows a positioning where no one else is standing, offering easy access to the patient for the bedside assistant. The four robotic arms are slimmer and designed to work in parallel, reducing conflicts even when the surgeon oversteps the limits of the initial targeted structures forcing the arms to work in a diagonal setting.
As a consequence, the placement of the trocars is less restrictive, they can be positioned in line, and the distance in between them can be shorter, which is particularly helpful in small patients. Distant structures can be easily reached with 5 cm longer robotic instruments, the camera can be inserted in any of the four 8 mm trocars, and robotic staplers are now available. This provides a real four-arm device, allowing for more adaptability in multiquadrant procedures, leading to a preference for totally robotic procedures and making hybrid procedures obsolete. 14
Another potential advantage of TRRC is represented by a more efficient lymph nodal and mesocolic excision. The concept of complete mesocolic excision (CME) with central vascular ligation has been first described by Hohenberger, based on the same principles as total mesorectal excision for the treatment of rectal cancer. 15 Variants of the original procedure have then been proposed and, after the introduction of the da Vinci Xi, we adopted a modified CME (mCME), as described by Cho et al. 16 Studies on oncological outcomes showed that CME has better survival rates when compared with incomplete mesocolon excision. 15
To obtain an adequate oncological radicality, CME requires a careful mesocolic dissection and a meticulous vessel isolation, which can be safely achieved by laparoscopy for cancers of the proximal right colon, but laparoscopic CME seems to be inferior to open CME for tumors located at any point between the distal ascending and proximal transverse colon in terms of completeness of mesocolic excision and number of lymph nodes harvested. 17 In these cases, robotic surgery may provide the comfort level and accuracy needed to perform an extended lymphadenectomy and adequate vascular control, particularly in obese patients, as some authors noted. 7
It is not clear whether robotics can effectively impact lymph node yield. In our series, the robotic group shows a greater number of lymph nodes harvested (20.5 ± 11.2 in the laparoscopic versus 23.13 ± 11.2 in the robotic group; P = .031), but no significant difference was found between HRRC and TRRC groups. The number of totally robotic procedures that we performed is likely still too small to lead to a definitive conclusion. Lymph node to length of surgical specimen ratio (LN/LS ratio) was also not significantly different between groups.
Nevertheless, other authors recently demonstrated that RRC improves lymph node yield and LN/LS ratio when compared with open and laparoscopic surgery. 18 They compared 181 open right colectomies with 163 laparoscopic and 119 robotic cases. Mean lymph node yield was significantly higher in the robotic approach (28, 29, and 34, respectively, in open, laparoscopic, and robotic groups; P < .01). Furthermore, robotic mean LN/LS ratio was higher compared with open surgery (1.0 versus 0.83, P < .01). These findings may reflect a better mesocolic excision in the robotic group. 18
At the time of the present work, few studies have been published demonstrating better oncological outcomes in terms of recurrence rates or survival rates with the use of robotics. Spinoglio et al. recently published a retrospective analysis on 100 patients who underwent right colectomy with mCME and IA. During a median follow-up period of 48.5 months (range 24–114 months), the survival rates were 94.5% for disease-specific survival, 91.4% for disease-free survival, and 90.3% for overall survival. 19
The lack of randomized controlled trials and the retrospective nature of most published analyses represent a strong limitation to confirming the potential advantages we presented. Further investigations and meta-analysis will hopefully confirm the surgical and oncological improvements that present literature highlights.
Conclusions
LRC, HRRC, and TRRC are safe approaches to right colon resections. RRC with IA shows better postoperative bowel recovery, shorter hospital stay, and lower rate of anastomotic complications (leaks and twists) and bleeding when compared with LRC with EA. Furthermore, it allows a more accurate CME. We then showed our preliminary results in a series of 30 TRRCs: recovery outcomes are encouraging but have to be confirmed in future analysis. The evolution of robotic surgical systems has provided surgeons a powerful tool even in multiquadrant procedures. The retrospective nature of the study represents a limitation to the validity of our results.
Footnotes
Disclosure Statement
No competing financial interests exist.