
Abstract
Abstract
Background:
A laparoscopic approach to repair of inguinal hernia has become popular. The reduction of an indirect sac can be challenging especially if it is long standing or is large. In such situations, the established practice is to divide the sac at the neck and ligate it. Ligation of the sac has been shown to cause increased postoperative pain. Hence we postulated that we could possibly avoid ligation of this divided sac without causing increased intraoperative difficulty or postoperative complications.
Methods:
This was a retrospective review of a prospectively maintained database of all patients who underwent laparoscopic totally extraperitoneal repair (TEP) during a 7-year period at our center with a minimum of 1 year of follow-up. We compared the outcomes of the patients who underwent only a division (group I) versus those who underwent division followed by ligation (group II) of the indirect sac.
Results:
There were 189 and 126 patients in groups I and II, respectively. Group I patients fared better in terms of operative times and postoperative pain scores. The postoperative complication and short-term outcomes were not significantly different between the two groups.
Conclusion:
Non-ligation of a divided indirect sac during TEP is feasible and has the advantages of reduced operative times and postoperative pain and does not lead to increased complications.
Introduction
L
Materials and Methods
This study was conducted at the department of surgical gastroenterology of a tertiary care hospital and was a retrospective review of a prospectively maintained database. An approval of the institutional review board was taken for the study. Since this was a retrospective study and no identifiable information would be recorded or revealed, an informed consent was deemed not necessary. The study period was from April 2008 to December 2015. The follow-up was updated until December 2016. The operated patients were divided into two groups for comparison. Group I was the nonligation group, operated upon by the first author who did not ligate the divided sac, and group II was the ligation group, operated upon by the second and third authors. All operating surgeons were experienced having done a minimum of 50 cases before this study period.
Aim
The aim of the study was to compare the outcomes between the two groups of patients. The primary objective was operative times and postoperative pain scores, and the secondary objectives were urinary retention, hospital stay, recurrences, intestinal obstruction, and costs.
Inclusion criteria
All indirect hernias that were operated by a totally extraperitoneal repair (TEP) technique and that necessitated a division of the hernia sac.
Exclusion criteria
All indirect hernias that did not require a division of the sac, direct hernias, bilateral hernias, recurrent hernias, complicated hernias, and pantaloon hernia and those that were operated by the transabdominal preperitoneal technique. Any patient in whom there was any deviation from the standard operating technique was also excluded.
Operative procedure
This has been described in detail in a previous publication. 7 The sac was divided using harmonic shear (Fig. 1a), and the proximal sac was left unligated (Fig. 1b). If ligation was done, a 0 polyglactin 910 endoloop (Vicryl; Ethicon) (Fig. 1c, d) was used. After the dissection, a 12 × 15 cm polypropylene mesh was introduced and spread to cover the entire myopectineal orifice. The mesh was fixed with absorbable tackers, medially on the Cooper's ligament and laterally near anterior superior iliac spine above the iliopubic tract. The standard analgesic used was injection diclofenac sodium at the end of the surgery and thereafter tab diclofenac sodium 12 hourly. The patients were usually discharged on the first postoperative day.
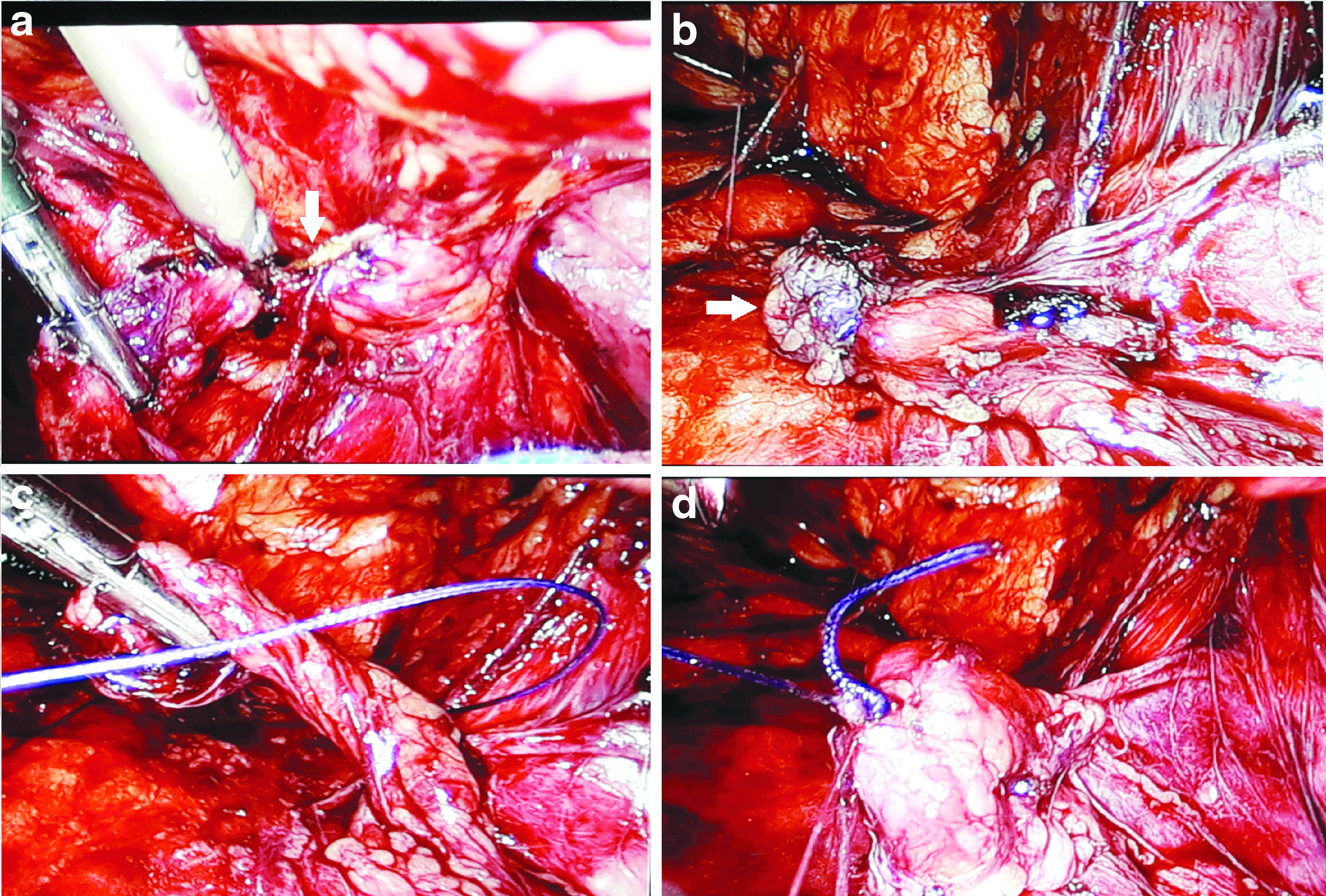
Intraoperative photographs.
Follow-up
The patients were regularly followed up. Follow-up was done at 1 week, 3 months, 6 months, and then yearly. The follow-up data for those patients who subsequently did not report for further follow-up were obtained by the means of telephonic interviews. Only patients who had completed a minimum of 1 year of follow-up were compared for recurrences and intestinal obstruction.
Definitions
Operative time
Time from the first skin incision to the last skin stitch/staple was applied.
Postoperative pain
Was assessed at 6 and 24 hours (just before administration of the next dose of analgesic) post-op and was assessed by a visual analog scale by the attending nursing staff.
Statistical analysis
Statistical analysis was done using the statistical software GraphPad available at www.graphpad.com. 8 Continuous data are presented as mean ± standard deviation and categorical data as numbers and percentages. Categorical variables were compared using Chi-square test or Fisher's exact test whichever applicable. Continuous variables were compared using Student's t-test. A P value of <.05 was considered as statistically significant.
Results
During this period a total of 637 patients were operated for an inguinal hernia laparoscopically. Of these, 315 patients met the inclusion criteria. There were 189 and 126 patients in group I (nonligation group) and II (ligation group), respectively (Fig. 2). The demographic profile and clinical characteristics between the two groups were not significantly different (Table 1).

Patients' flowchart.
Operative time
The mean operative time in groups I and II was 42.4 ± 10.7 and 46.9 ± 12.1 minutes, respectively. This was statistically significant (Table 2 and Fig. 3a).
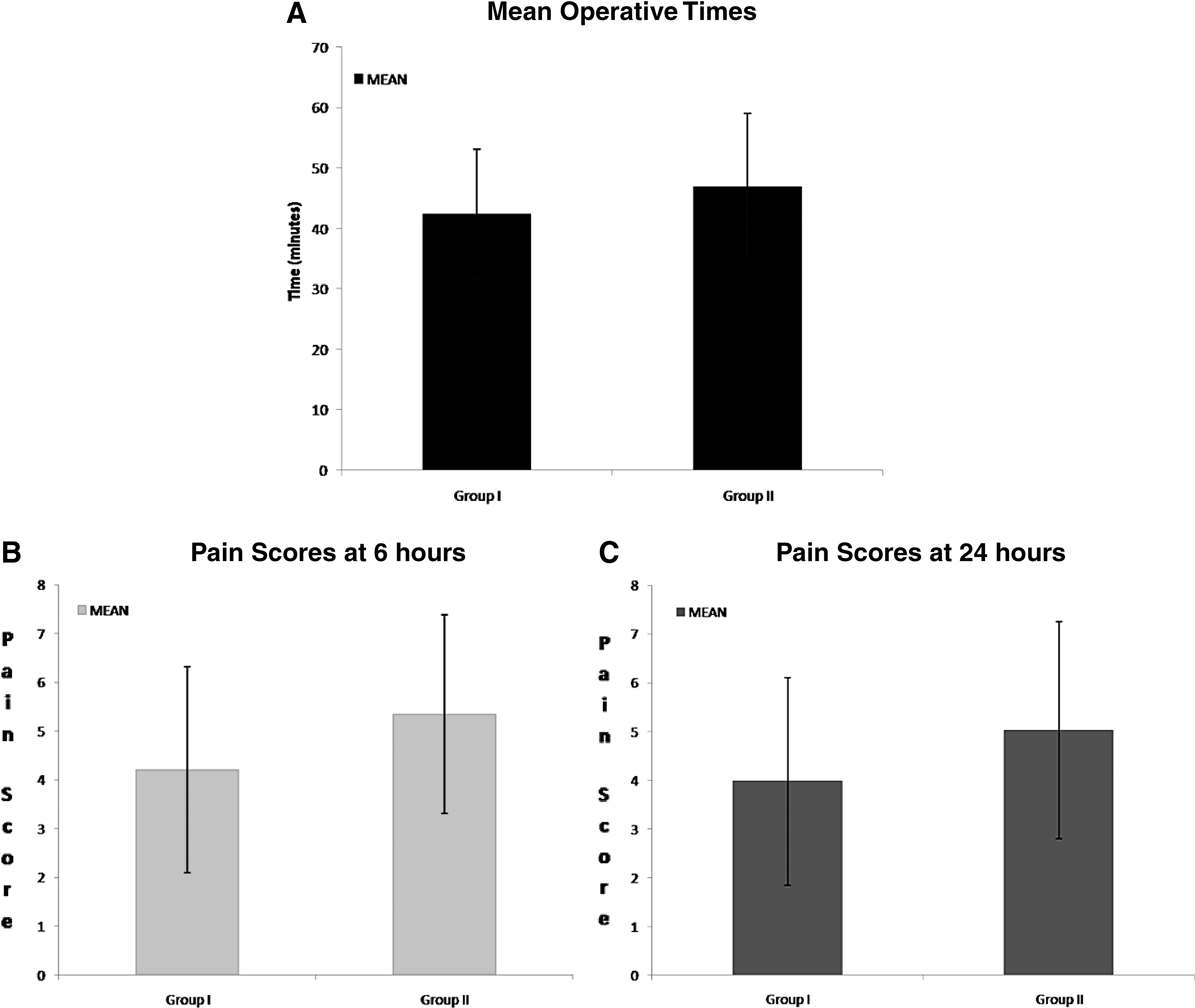
Pain scores
The pain scores, both at 6 and 24 hours postsurgery, were significantly more in the ligation group; 4.21 ± 2.11 versus 5.35 ± 2.04 (P = .008) at 6 hours and 3.98 ± 2.13 versus 5.03 ± 2.23 (P = .010) (Table 2 and Fig. 3b, c).
Short-term complications
At a mean follow-up of 31.2 ± 11.1 and 21.3 ± 6.1 months for the two groups, the recurrences or the incidences of intestinal obstruction were low and not significantly different (Table 2).
Discussion
In laparoscopic inguinal hernia surgery, the sac is dissected out, reduced without ligation, and a mesh is placed. While the management of a direct sac during laparoscopic inguinal hernia repair is relatively easy, it is not so in the case of an indirect hernia. It can be really challenging to dissect out a complete sac or an adherent long-standing sac or in recurrent hernias, especially in TEP when the working space is very limited. Prolonged dissection to completely reduce the sac can be time consuming, messy, and can lead to increased chances of injury to cord structures. 4 To avoid this, it may be better to divide the sac at the neck, ligate it, and leave the distal sac open, as is done in open repairs. But studies with open repairs have shown that this ligation of the sac leads to increased pain.
The concerns in leaving a divided indirect sac without ligating it are:
The idea of not ligating the divided sac was born out of the first author's experiences. He observed that when there was an inadvertent rent in the sac during its dissection and was not repaired, this did not lead to significantly increased difficulties during the surgery. In addition, these patients did not experience any complications related to the unrepaired rent in the postoperative period and in the short-term follow-up. This evolved to adoption of non-ligation in the case of divided indirect sacs during TEP. This non-ligation is akin to a peritoneal rent that occurs during dissection in TEP. The explanation put forth for not finding an increased difficulty is that when an ultrasonic shear is used to divide the sac, the divided end remains sealed for some time. If and when the neck ultimately opens out, the resulting pneumoperitoneum does not cause too much loss of working space as the pressures in the extra and intraperitoneal space equalize with less than expected loss in working space. In addition, the Trendelenburg position with the operated side raised higher adopted ensures that the carbon dioxide “rises” into the extraperitoneal compartment. Furthermore, the division of sac is the penultimate step and only the placement of mesh remains, which can be easily accomplished in this reduced space. Shpitz et al., in their prospective study, have questioned the practice of closing peritoneal rents during TEP. They divided the peritoneal tears into two groups—early (during balloon dissection) and late (during dissection of the sac). In the late group, the surgery could be completed successfully, needed no conversion, with only an occasional use of Veress needle to decompress the pneumoperitoneum and without much difficulty. 11
In open repairs, it has been shown that it is safe to divide the sac at the neck and leave it open without ligating it.12,13 Smedberg et al. have shown that this does not lead to increased recurrences and at the same time causes less postoperative pain. 6 Shulman et al., in a large study of adult inguinal hernias, termed the ligation of sac a needless step and showed that it leads to increased postoperative pain. 14 A high dissection of the sac, right down to the retroperitoneum and not the ligation of the sac, is the crucial step to prevent recurrences. 15 It has been shown that the peritoneal defect rapidly closes within a few hours to a day due to the migration of the mesothelial cells in the peritoneum.15,16 In addition, a properly placed mesh would effectively prevent recurrences.
Leaving the peritoneum open has been shown not to cause more adhesions as it rapidly heals.17,18 In contrast, we believe that the focal inflammation at the site of ligation of the peritoneal sac might induce adhesion formation. Shpitz et al. did not close the peritoneal rents that occurred during TEP and found no complications related to nonclosure of the rents in their mean follow-up of 16 months. 9 In our study, we found that there were no increased incidences of intestinal obstruction due to adhesions or internal herniation in the nonligation group. In fact, the only incidence of intestinal obstruction in our study occurred in the ligation group. The patient was operated upon, and the obstruction was found to be due to a loop of small intestine that had herniated through a peritoneal rent at the proximal edge of the mesh and was sandwiched between the mesh and anterior abdominal wall.
An indirect measure of the difficulty during the surgery is the operative time. 19 In this study, the operative time was significantly higher in the ligation group. This, on one hand, reflects the extra time consumed in ligating the divided sac, while on the other hand, it goes on to underline the fact that no extra time was needed to place the mesh after dividing the sac and not ligating it. Lau et al. compared the ligation of sac versus complete dissection of the sac and reduction. They found significantly increased operative time in the ligation group. 5 In this study, the authors ligated the sac using 2–0 Vicryl using an intracorporeal knotting technique before dividing the sac. We circumferentially dissected the sac and divided it carefully avoiding cord structures and used a Vicryl endoloop to ligate it which required lesser time than would be required for intracorporeal knotting, and still, the operative time was longer in the ligation group. Increased operating time means longer anesthesia time and higher costs. 20 A difference of about 4 minutes between the two groups, notwithstanding the fact that it was found to be statistically significant, may not appear to be clinically relevant in day-to-day practice. But in terms of opportunity costs for the surgeon, it may be substantial when we consider the total time lost in a year for this particular surgery. 21 Nevertheless, the point of the article is not about the time saved or economy achieved. It is about the feasibility of eliminating a non-essential step thereby making the technique simpler and easier without compromising the safety or results.
A significant finding of our study was the lesser pain scores at 6 and 24 hours after surgery. This echoes the findings of various studies in the literature.6,14 The pain scores in our study were not assessed by the operating surgeons, but by the attending nursing staff and, thus, would not lend to any bias. A meta-analysis of sac ligation in inguinal hernia repair concluded that sac ligation was associated with higher postoperative pain and did not offer any advantage over non-ligation. 22 The ligation of sac causes crushing and ischemia of the peritoneum which would, in turn, lead to focal peritonitis.17,23 This possibly could explain the increased postoperative pain in this group. In fact, we believe that this ischemia and focal peritonitis might cause adhesions at the site and its related complications. However, this can only be conclusively proven in animal studies as not many of these patients would undergo a laparotomy or laparoscopy at a later date to record the findings, and the complication caused by these adhesions would be infrequent. Of many reasons for postoperative urinary retention, pain is one of the causes. An increased pain in the immediate postoperative period should give rise to increased incidences of urinary retention. Our study, however, failed to demonstrate this difference. A possible explanation would be the relatively younger cohort of patients in our study as our inclusion criteria included indirect hernias only which would preclude direct hernias which are more prevalent in the older population.
Our study is the first one to look into the merits of non-ligation of a divided indirect sac in TEP. We have shown that the ligation of the divided sac is not necessary and gives rise to increased postoperative pain. Furthermore, by not ligating the sac, there would be some cost benefits too.
Our study has a few drawbacks. The first one is that this is a retrospective study. However, the data analyzed were a prospectively maintained one. The second is that both groups were not operated by the same surgeon(s). In this study, we would like to emphasize that all surgeons were experienced and followed the same technique except for the management of the divided sac. Furthermore, an audit of TEP done at our center before introduction of non-ligation showed that the operative times were similar for all the three surgeons. The third is that we did not record the pain scores beyond the 24 hours after surgery. It would have been interesting to know how the two groups fared at 1 week and beyond and if there were any difference in the time taken to the resumption of normal activities. In addition, we did not record the total number of analgesic doses taken by the patients in the postoperative period after discharge. Finally, the follow-up was significantly longer in the non-ligation group compared to the ligation group. This was because the second and third author joined the team at a later date and hence the follow-up was comparatively shorter.
In conclusion, we suggest that one could safely avoid ligating a divided sac while managing a difficult indirect sac during a laparoscopic TEP of an inguinal hernia. In doing so, it lessens the operative time, causes lesser postoperative pain to the patients, does not lead to increased complications like recurrences, and costs less too.
Footnotes
Disclosure Statement
No competing financial interests exist.