
Abstract
Abstract
Background:
Thiol/disulfide homeostasis is a significant parameter in determining the oxidative stress response after ischemia and reperfusion. We aimed to investigate the effects of applying different intraabdominal pressure (IAP) on thiol/disulfide homeostasis, ischemia-modified albumin (IMA) levels, and hemodynamics in pediatric laparoscopic surgery.
Materials and Methods:
Blood samples were collected from 36 pediatric patients who were planned to undergo laparoscopic surgery for nonpalpable testis or varicocele under general anesthesia, immediately after intubation as the baseline and 5 minutes after abdominal desufflation for determining the thiol/disulfide, and IMA levels. The patients were divided into two groups; group 1 received a pneumoperitoneum pressure of 8 mm Hg (n = 18), and group 2 received 12 mm Hg (n = 18). The clinical characteristics and thiol/disulfide homeostasis and IMA levels of the patients were compared.
Results:
No difference was detected regarding the clinical features between the groups. The comparison after intubation and after desufflation in group 1 demonstrated lower native thiol (453 ± 67 versus 422 ± 57 μmol/L, P = .059) and total thiol (497 ± 73 versus 466 ± 62 μmol/L, P = .061) levels, which was statistically insignificant. The serum native thiol level was found lower than baseline in group 2 where a 12 mm Hg IAP was applied, this difference was not statistically significant (429 ± 47 versus 412 ± 53 μmol/L, P = .078). The comparison of serum IMA levels after desufflation with the baseline (0.505 ± 0.018 versus 0.632 ± 0.022) in group 2 was found statistically significantly high (P = .031). The comparison of the perioperative heart rate and SpO2 levels with before induction was found statistically insignificant.
Conclusions:
Neither of 8 nor 12 mm Hg IAPs in pediatric laparoscopic surgery caused any changes in novel indicators of thiol/disulfide homeostasis parameters; however, 12 mm Hg IAP increased the levels of IMA.
Introduction
L
Thiols in the organisms are components that involve the sulfur group and are the essential antioxidant buffers that interact with almost all physiologic oxidants. The majority of the plasma thiol pool consists mainly of albumin and of the other proteins and the small part consists of thiols with low-molecular weight such as cysteine, cysteinylglycine, glutathione, homocysteine, and γ-glutamylcysteine.11,12 The thiol groups of proteins are transferred to reversible disulfide bond structures by the oxidization of oxidant molecules in the environment. The disulfide bond structures may reduce back to thiol groups, and thus, the thiol disulfide balance is maintained. 12 Thiol/disulfide homeostasis has a significant role in vital functions, detoxification, antioxidant preservation, and in the regulation of cellular enzymatic activity. 11 Thiol/disulfide homeostasis was shown to have a role in the pathophysiology of various diseases.12,13
Another oxidation parameter that may be used as a perioperative ischemia marker is ischemia-modified albumin (IMA). Hypoxia, acidosis, and superoxide radical damage lead to the formation of IMA by decreasing the binding capacity of albumin to metals by changing the structure of the N-terminal. IMA is an indicator that increases early in ischemia, it increases in as little as 6 minutes. 14
The method of anesthesia, surgical method, drugs used, infection, and the duration of surgery affect the postoperative morbidity and mortality by changing the stress response. In addition, laparoscopic procedures and analgesia in the surgical region decrease the stress response. Researchers have investigated the effects of duration in laparoscopic surgery, and IAPs on hemodynamics, stress hormones, total oxidant status, and antioxidant capacity.3–6 Although similar studies have previously been performed in adults, the responses to hemodynamics and operative procedures in children differ from those in adults. It is well known that children exhibited lower values of IAP-induced cardiorespiratory changes than adults. 8 However, a limited number of studies have compared the oxidation parameters in pediatric laparoscopic surgeries with different IAPs. 3 Our hypothesis is that lower pressure has a beneficial effect on the thiol disulfide redox status in pediatric patients.
The change in thiol/disulfide homeostasis in laparoscopic surgery has been shown 15 ; however, we found no studies that investigated the effects of different IAPs in pediatric patients on thiol/disulfide homeostasis.
In the present study, we aimed to investigate the effect of applying different IAPs in pediatric patients during laparoscopic surgery on thiol/disulfide homeostasis, IMA, and intraoperative hemodynamics.
Materials and Methods
Study design
The study protocol was approved by the local Ethics Committee (2011-KAEK-25 2015/16-07). Written informed consent was obtained from parents. The study was conducted in accordance with the principles of the Declaration of Helsinki. This prospective, randomized study was carried out in a single center between January 2016 and June 2017. All researchers, except the pediatric surgeon, were blinded to the allocation to either low IAP or high IAP throughout the study period.
Patients who were, American Society of Anesthesiologists (ASA) physical status I, aged 2–16 years and scheduled for nonpalpable testis or varicocele surgery were enrolled in the study. The patients who had systemic infection, metabolic, endocrine, hepatic, or renal disease, patients using medicine that might affect the oxidation system, and patients with abnormal preoperative blood levels were excluded from the study. Patients who were converted to open surgery intraoperatively and those who developed complications were excluded from the study.
The patients were divided into two groups in accordance with the insufflation pressure levels as group 1 (n = 18), which was applied 8 mm Hg pressure, and group 2 (n = 18), which received 12 mm Hg pressure.
Anesthesia procedure
No premedication was administered to the patients. The determination of the groups was accomplished using a randomized system with the sealed envelope technique. Routine monitorization and Angiocut insertion were performed after administration of intravenous propofol (Pofol®, Ilsan-Iltas Kocaeli, Turkey) 2–2.5 mg/kg, rocuronium bromide (Curon® Mustafa Nevzat, Istanbul, Turkey) 0.6 mg/kg i.v., and fentanyl (Talinat®; Vem, Istanbul, Turkey) 1–2 mcg/kg for induction of anesthesia. After tracheal entubation, the fresh gas flow rate was set to 4 L/minutes in all patients. Anesthesia was maintained with 1.5–2 minimum alveolar concentration sevoflurane (Sevorane®; Abbvie, Istanbul, Turkey) in a 50/50% (v/v) oxygen–air mixture. Ventilation was performed to enable an end-tidal carbon dioxide (EtCO2) level of 35–40 mm Hg. Intravenous fentanyl 0.5 and 0.2 mcg/kg rocuronium bromide were administered for anesthesia maintenance. At the start of spontaneous respiration, 100% O2 was given, and extubation was carried out after the reversal doses of i.v. neostigmine (Neostigmine®; Adeka, Istanbul, Turkey) (0.03–0.05 mg/kg) and atropine sulfate (Atropin sulfat®; Osel, Istanbul, Turkey) (0.01 mg/kg).
For the determination of thiol/disulfide homeostasis and IMA serum level, blood samples were collected before insufflation (baseline) and 5 minutes after emptying the abdominal gas. The insufflation times of all patients were recorded. The perioperative heart rate (HR), perioperative systolic (SBP), diastolic (DBP), mean blood pressure (MBP) levels, peripheral oxygen saturation (SpO2), and end-tidal sevoflurane levels were recorded in the preoperative period, and at 5, 10, 15, 30, 45, 60, and 90 minutes after intubation.
Operative details
After induction of general anesthesia, a Veress needle was placed to the peritoneal cavity via an infraumbilical incision, CO2 flow rate was set to 2 L/minutes, and pneumoperitoneum was formed with a pressure of 8 or 12 mm Hg. The needle was pulled out and 10 mm trocar was inserted into the peritoneal cavity at the same incision. The telescope is then inserted and the intraabdominal cavity explored. Two further 3 mm ports were inserted lateral to each Rectus Muscle, at the same level as the umbilical trocar under direct vision. The patients were placed in a Trendelenburg position (25-degree head down). Laparoscopic procedures included laparoscopic identification of intraabdominal testes, hemoclip ligation of the testicular vessels for two-step orchiopexy, and intracorporeal ligation of spermatic vessels for varicoceles. At the end of laparoscopy, the patient was returned to the horizontal position and the abdomen was desufflated. The operative procedure was completed when the port sites are closed with a fascial closure.
Serum sampling
The blood samples were collected in 5-mL Vacusera clot activator tubes (Disera, Izmir, Turkey), and were immediately sent to the laboratory. The plasma and serum were differentiated and stored at −80°C until testing after centrifuging the serum samples at 2500 rpm for 10 minutes to study the native thiol, total thiol, disulfide, disulfide/native thiol ratio, disulfide/total thiol ratio, native thiol/total thiol ratio, and IMA. Serum disulfide/thiol homeostasis measurements were determined with the automated spectrophotometric method described by Erel and Neselioglu. 12 The IMA was studied using the spectrophotometric method defined by Bar-Or et al. and reported as absorption units. 16
Statistical analysis
Calculations were performed by using computerized software, SPSS version no. 21.0 (SPSS, Inc., Chicago, IL). The normality of the continuous variables was analyzed with the Kolmogorov–Smirnov test and Shapiro–Wilks test. Data are expressed as means ± standard deviations when normally distributed or with medians otherwise (Interquartile range). Paired t-test was used for intragroup comparisons. Data between the groups were compared with t test. A statistical significance was established when the P value was <.05.
Results
Forty-seven patients who underwent laparoscopic surgery for nonpalpable testis or varicocele were included in the study; 7 patients were excluded due to their age, and open surgery was performed in 2 patients. Thirty-six patients were included in the statistical evaluation because the serum of 1 patient was hemolyzed, and 1 patient's serum sample was inadequate (Fig. 1). No significant difference was detected regarding demographic data such as age, weight, duration of surgery, and duration of pneumoperitoneum (P > .05) (Table 1).
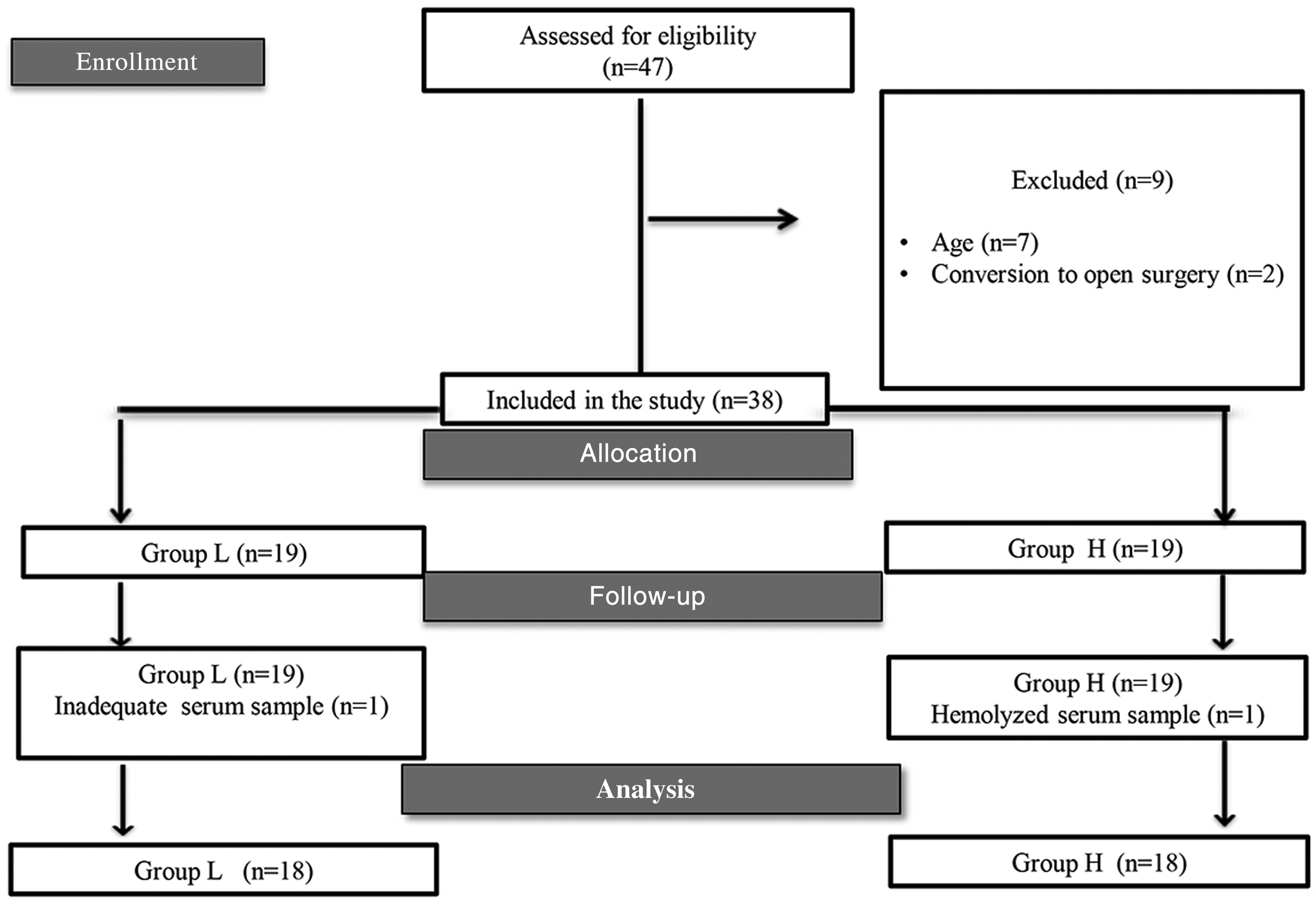
Flowchart of the study.
Group 1, received a pneumoperitoneum pressure of 8 mm Hg; Group 2, received a pneumoperitoneum pressure of 12 mmHg. Data are expressed as mean ± SD.
SD, standard deviation.
Primary outcomes
The comparison of the two groups before insufflation and after desufflation revealed no statistical difference regarding the native thiol, total thiol, disulfide, disulfide/total thiol ratio, native thiol/total thiol ratio, and IMA levels. Although native thiol (453 ± 67 versus 422 ± 57 μmol/L, P = .059) and total thiol (497 ± 73 versus 466 ± 62 μmol/L, P = .061) levels decreased in group 1 in the within-group comparison before insufflation and after desufflation, no statistically significant difference was detected (Table 2).
Group 1, received a pneumoperitoneum pressure of 8 mm Hg; Group 2, received a pneumoperitoneum pressure of 12 mmHg; *P = .031, IMA levels compared with baseline after desufflation in Group 2; data are expressed as mean ± SD statistically differences compared to baseline paired t test.
IMA, ischemia-modified albumin; ABSU, absorbance units; SD, standard deviation.
The serum native thiol (429 ± 47 versus 412 ± 53 μmol/L, P = .078) and total thiol (468 ± 46 versus 454 ± 53, P = .147) levels decreased in comparison with before insufflation and after desufflation in group 2, in which higher IAP was applied; however, the difference was statistically insignificant. Serum IMA levels in group 2 after desufflation were statistically significantly higher compared with the levels before insufflation (0.505 ± 0.18 versus 0.632 ± 0.22, P = .031) (Table 2).
Secondary outcomes
No statistically significant difference was detected regarding the perioperative SBP, DBP, and MBP levels between the groups. No statistically significant difference was detected in the intraoperative end-tidal sevoflurane and EtCO2 measurements between the groups (P > .05). SpO2 was detected to be statistically significantly lower in group 2 compared with group 1 at 30, 45, 60, and 90 minutes (respectively, P = .02, P = .002, P = .004, P = .001). The HR was found statistically significantly lower in group 2 perioperatively at 5, 15, 30, and 45 intraoperative minutes compared with group 1 (P < .05). No difference was detected in SBP, DBP, and MBP in the comparison of the groups (P > .05).
Discussion
We found no significant difference after desufflation in the comparison of native thiol, total thiol, and disulfide levels with baseline levels in pediatric patients who were applied 8 or 12 mm Hg IAP. Postoperative IMA levels were significantly higher compared with the basal level in the group that was applied 12 mm Hg pressure.
Studies have investigated oxidative stress in laparoscopic surgery3–6,17,18; however, the number of studies investigating the effects of laparoscopy on oxidative stress in the pediatric age group is limited. 3 According to our literature search, our study is the first to compare thiol/disulfide homeostasis in different IAPs during laparoscopy surgery in pediatric patients. Recently, Elmas et al. demonstrated that thiol disulfide homeostasis as a novel indicator of oxidative stress was strongly associated with increased inflammation in children. 19 Both are noninflammatory diseases, and inflammatory processes have been shown in many studies that can increase oxidative stress. 20 In this study, we selected patients with undescended testis and varicocele to investigate the effect of IAP during surgery without coexistence of inflammation.
Although the blood flow to the parietal peritoneum significantly decreased when the IAP was higher during surgery, no change was demonstrated with an IAP of 10 mm Hg. 21 It was anticipated that the postoperative oxidative system would be activated due to the intestinal manipulation, splanchnic vasoconstriction, intervention on peritoneum, perfusion decrease in the visceral region, reperfusion, and inflammatory cell stimulation during surgery, in addition to intraabdominal CO2 insufflation.3,4,18 Earlier, researchers found that the oxidative stress developed in laparoscopic patients was significantly correlated with gas volume and the insufflation period. 22
In the literature, blood samples have been collected at different perioperative periods in studies on oxidative stress during laparoscopic surgery. Oxidation parameters were generally studied before insufflation,3,18 immediately after desufflation, and until 24 hours.16,18 Immediately after reperfusion, free oxygen radicals are released and have been proposed as important mediators of tissue injury. 23 In our study, we did not sample patients' blood after abdominal insufflation, because our main goal was to investigate the reperfusion injury caused by abdominal desufflation.
Polat et al. 15 demonstrated that the occurrence of ischemia–reperfusion with reperfusion after the increase of IAP and after desufflation might affect thiol/disulfide homeostasis. The researchers monitored the changes in thiol/disulfide homeostasis until 24 hours postop in adult patients undergoing laparoscopic cholecystectomy and open inguinal surgery. 15 They found the native thiol, total thiol, and disulfide levels significantly lower after desufflation in the laparoscopy group compared with baseline; however, IMA levels were higher compared with baseline levels. Our study was different from theirs because we studied pediatric patients and only included the intraoperative period due to the performance of ambulatory surgery. The native thiol and total thiol levels decreased in both groups after desufflation compared with baseline; however, the disulfide levels were higher, which was statistically insignificant. In our patients, IMA levels were statistically significantly high only in the higher pressure group compared with baseline.
The increase of pneumoperitoneum pressures over 10 mm Hg leads to splanchnic ischemia, formation of free oxygen radicals, tissue damage, and organ dysfunction. 24 Despite different opinions on the safe pressure range in laparoscopy, 8–12 mm Hg IAP application was found as a safe pressure range in immune, metabolic, and oxidative stress response. 25 Polat et al. 18 found no difference in lipid peroxidase levels as an oxidative stress marker in laparoscopic cholecystectomy groups where 10 or 15 mm Hg IAP was applied. Nunes et al. 26 detected that 12 mm Hg CO2 pneumoperitoneum pressure and deep anesthesia caused a higher oxidative stress response in patients who underwent laparoscopic surgery. However, those pressure levels were described in adult patients. In the present study, we found that pressures of 8 or 12 mm Hg in pediatric patients did not affect thiol/disulfide homeostasis.
Researchers demonstrated that laparoscopic surgery caused ischemia reperfusion, and this ischemic effect might occur with the increase in serum IMA level within minutes. 27 We also detected an increase in IMA levels after desufflation in the group that received 12 mm Hg pressure. Similar to our study, Aran et al. reported that IMA levels increased 30 minutes after insufflation in adult patients who underwent laparoscopic surgery 25 ; however, no significant difference was detected in the oxidative indicator malondialdehyde, total oxidant status, total antioxidant status, and oxidative stress index. The authors interpreted that IMA was a more sensitive indicator below 12 mm Hg IAP.
Different results have been reported in human and experimental studies that investigated the hemodynamics and respiratory changes in laparoscopic surgery in the literature.9,28,29 Ahmed 2 found hemodynamic changes in patients who were applied 12 mm Hg pressure compared with 6 mm Hg pressure in their study, and echo findings significantly changed. Rishimani et al. 28 found that HR and SpO2 were not statistically significantly lower in adult laparoscopic cholecystectomies with different IAP applications. Sakka et al. 9 found a decrease in transesophageal echo and higher cardiac index in pediatric patients undergoing laparoscopic hernia repair who were applied 6 and 12 mm Hg IAP; however, the decrease was not significant for the clinics. Halachmi et al. 29 found a statistically significant decrease in HR and SpO2 after carbon dioxide insufflation in laparoscopic surgery in the high IAP group. In our study, the decrease of perioperative HR and SpO2 levels in the high-pressure group was not statistically significant compared with the preinduction levels. No hemodynamic or respiratory problems were detected in our patients after desufflation or in the postoperative period.
Limitations of the study: our study was a single center study conducted with a small number of patients, and we did not investigate the thiol/disulfide parameters in the late postoperative period.
Conclusion
We found that both 8 or 12 mm Hg IAP in pediatric laparoscopic surgeries caused no significant changes in thiol/disulfide homeostasis parameters, and caused no oxidative stress that might affect the antioxidant pool of the human body. However, the early increase in IMA with 12 mm Hg IAP in children was interpreted as the organism's reperfusion response to a nonsignificant oxidative state. We suggest that more studies with larger numbers of patients and with a longer postoperative period are required in pediatric patients.
Footnotes
Disclosure Statement
No competing financial interests exist.