
Abstract
Abstract
Purpose:
To compare the short-term outcomes of robot-assisted partial nephrectomy (RPN) and laparoscopic partial nephrectomy (LPN) when performed by highly experienced surgeons.
Methods:
A prospective multicenter study was conducted, including the 50 last patients having undergone LPN and RPN for T1-T2 renal tumors in two institutions between 2013 and 2016, performed by two different surgeons with an experience of over 200 procedures each in LPN and RPN, respectively, at the beginning of the study. Perioperative parameters and functional and oncological outcomes were collected and compared between the LPN and RPN groups.
Results:
The laparoscopic approach was associated with a longer warm ischemia time (15.7 versus 23 minutes; P < .001) and hospital stay (3.6 versus 4.6 days; P = .01). Conversely, estimated blood loss was significantly higher in the RPN group (381 mL versus 215 mL; P < .001), but transfusion rates were similar between the two groups (8% versus 6%; P = .33). In the RPN group, three patients (6%) required conversion to open partial nephrectomy and three patients (6%) required a conversion to radical nephrectomy (RN), while no conversion was needed in the LPN group. There were no differences in terms of perioperative complications, and change in renal function was comparable in the two groups postoperatively. Positive surgical margin rates were similar in the RPN and LPN groups (2% versus 6%; P = .36). After a median follow-up of 19 and 14 months in the RPN and LPN groups, respectively (P = .38), recurrence-free survivals did not differ significantly (P = .94).
Conclusion:
In this series, perioperative and short-term oncological and functional outcomes appeared broadly comparable between RPN and LPN when performed by highly experienced surgeons.
Introduction
P
PN has traditionally been performed through an open access. Expert teams described laparoscopic partial nephrectomy (LPN) in the early 2000's and reported similar cancer control, but improved postoperative recovery compared to open PN. 3 However, the use of LPN remained limited during this period because of its technical complexity. 4 Conversely, robot-assisted partial nephrectomy (RPN) has been widely adopted because of lower difficulty that enabled less experienced surgeons in laparoscopy to perform the procedure efficiently and safely. 5
Many studies comparing LPN to RPN have been published and constantly showed better perioperative outcomes with RPN. However, all these publications included cases performed by surgeons in their early learning curve.6,7 Moreover, LPN remains a minimally invasive technique and could offer a relevant cost-effective alternative to RPN. 8
The objective of this study was to compare perioperative and short-term oncological and functional outcomes of LPN and RPN performed by experienced surgeons beyond the learning curve. We hypothesized that the benefits provided by the robotic assistance would not necessarily remain once a surgeon has a large laparoscopic experience.
Methods
Study design and population
A prospective two-center study was conducted. Between January 2013 and June 2016, data from all patients undergoing LPN (center 1) and RPN (center 2) for T1-T2 renal tumors were prospectively collected. Patients operated by two experienced surgeons who had performed over 200 LPN (center 1, B.G.) or RPN (center 2, K.B.) at the beginning of the study period were included for analysis. Surgeon from center 2 (K.B.) had a previous LPN experience of 50 cases. Surgeon from center 1 (B.G.) also had a wide experience in laparoscopic urologic oncology.
The RENAL nephrometry Scoring System was used to evaluate tumor complexity. 9 The following perioperative data were collected: operative time (OT), warm ischemia time (WIT), estimated blood loss (EBL), transfusion rate, surgical margins, conversion to laparotomy, and/or conversion to RN. Complications were graded according to the modified Clavien-Dindo classification and were reported using the European Association of Urology (EAU) guidelines.10,11 Major complications were defined as Clavien score ≥3. Hemorrhagic complications were defined as the occurrence of one of the following events: pseudoaneurysm, arteriovenous fistula, bleeding requiring reoperation, or hematoma requiring blood transfusion.
Renal function was evaluated by estimated Glomerular Functional Rate (eGFR) using the Modification of Diet in Renal Disease equation. 12 Indications for nephron-sparing surgery were categorized as imperative (i.e., single kidney or preoperative eGFR <60 mL/min) or elective (no imperative criteria).
Surgical technique
All procedures were standardized and performed through a transperitoneal route. In both groups, intraoperative renal ultrasound was used systematically to confirm the depth and the limits of the tumor.
LPN in center 1
All PNs in this group were performed through a pure laparoscopic approach (i.e., no hand-assisted approach was used). Bulldog endoscopic clamp was used to clamp the renal artery. Sharp excision of the tumor was performed with cold scissors. Renal reconstruction was achieved with 2-0 Vicryl sutures and Hem-O-Lok® clips (Weck Closure Systems, Research Triangle Park, NC) according to the “sliding-clip” technique. Additional 2-0 Vicryl® sutures were placed through the renal capsule and tied over a Surgicel® bolster. Renal artery was unclamped at the end of renal parenchyma repair. When necessary, a topical hemostatic agent was applied over the bolster. A suction drain was left postoperatively in all patients.
RPN (center 2)
The Da Vinci® Surgical System (Intuitive Surgical, Inc., Sunnyvale, CA) was used with a standard 3-arm approach. Excision of the tumor was always performed with cold scissors. In most cases, the early unclamping technique was used (the renal artery was unclamped after one or two running sutures on the tumor bed, but before parenchymal repair). 13 The renal reconstruction was made according to the sliding-clip renorrhaphy technique. Hemostatic agents were never used, and no drain was left postoperatively in place.
Follow-up
Patients were followed according to local postoperative protocols. A clinical examination, serum creatinine measurement, and contrast-enhanced computed tomography of the chest, abdomen, and pelvis were performed at 6, 12, 18, and 24 months and then yearly for a minimum of 5 years.
Statistical analyses
Means and standard deviations were reported for quantitative continuous variables, median and range for quantitative ordinal variables, and proportions for nominal variables. Comparisons between groups were performed using χ2 test and Fisher exact test for discrete variables and Mann–Whitney test for continuous variables. Cancer-specific survival (CSS), overall survival (OS), and recurrence-free survival (RFS) were estimated using the Kaplan–Meier analysis and compared with the log-rank test. Statistical analyses were conducted using JMP® v.12.0 software (SAS Institute, Inc.®, Cary, NC). All tests were two sided with a significance level at P < .05.
Results
Patients' characteristics and surgical techniques
The last 50 consecutive PN performed by each surgeon were included (100 patients in total). The patients' characteristics are summarized in Table 1. Patients in the LPN group were older (63.8 years versus 57.6 years; P = .01), but had comparable comorbidities (American Score of Anesthesiology [ASA] 3: 24% versus 30%; P = .43). There were more imperative indications in the RPN group (24% versus 2%; P = .05).
ASA, American Score of Anesthesiology; eGFR, estimated glomerular functional rate; LPN, laparoscopic partial nephrectomy; RPN, robot-assisted partial nephrectomy.
Surgical techniques are summarized in Table 2. There was a much wider use of the early unclamping in the RPN group (92% versus 2%; P < .001). Hemostatic agents were used only in the LPN group (90% versus 0%; P < .001). Similarly, postoperative drainage was used only in the LPN group (98% versus 0%; P < .01).
Perioperative outcomes
Mean OT was similar between the RPN and the LPN groups (134 versus 146.6 minutes, P = .1) (Table 3). Mean WIT was shorter in the RPN group (15.7 versus 23 minutes; P < .001). EBL was significantly higher in the RPN group (381 mL versus 215 mL; P < .001). Transfusion rates were similar between the LPN and the RPN groups (8% versus 6%; P = .33). In the RPN group, there were three conversions to an open approach and three conversions to RN: two patients required conversion to open RN (one because of tumor effraction and discovery of hilar nodes and one because of intraoperative discovery of tumor thrombus), one patient required conversion to open PN because of adherent perirenal fat making the dissection difficult, and one patient required conversion to RN because of a hilar bleeding despite optimal repair. In the LPN group none of the patients had conversion nor RN during the laparoscopic surgery.
Nineteen patients had complications after LPN (38%) and 16 patients (32%) after RPN (P = .53). There was no difference between the two groups in terms of major complications (8% versus 10%; P = .55).
Major complications in the LPN cohort included two Clavien 3 complications (perirenal urinoma requiring percutaneous drainage, urinary fistula that required reintervention) and three Clavien 4 complications (one reintervention for a hemorrhage on the resection bed, one patient who required a RN for persistent bleeding, and one patient who developed respiratory failure due to bilateral pulmonary atelectasis).
Four patients experienced major postoperative complication in the RPN group. Two patients developed a pseudoaneurysm that required angioembolization and blood transfusion, and two patients had an arteriovenous fistula requiring angioembolization.
Mean length of stay (LoS) was longer in the LPN group (3.6 versus 4.6 days; P = .01).
Short-term oncological and functional outcomes
Functional outcomes are summarized in Table 4. There was no difference between the two groups in terms of eGFR changes in the early postoperative period, at 1 month or at last follow-up.
Oncological outcomes are detailed in Table 5. Positive surgical margin rates were similar in both groups (2% versus 6%; P = .36). Histological subtypes, T stage, and Fuhrman grade were also similar between the two groups. After a median follow-up of 19 and 14 months in the RPN and LPN groups, respectively (P = .38), RFS (Fig. 1), CSS, and OS were similar. No cancer-specific death was observed in any of the two groups during follow-up.
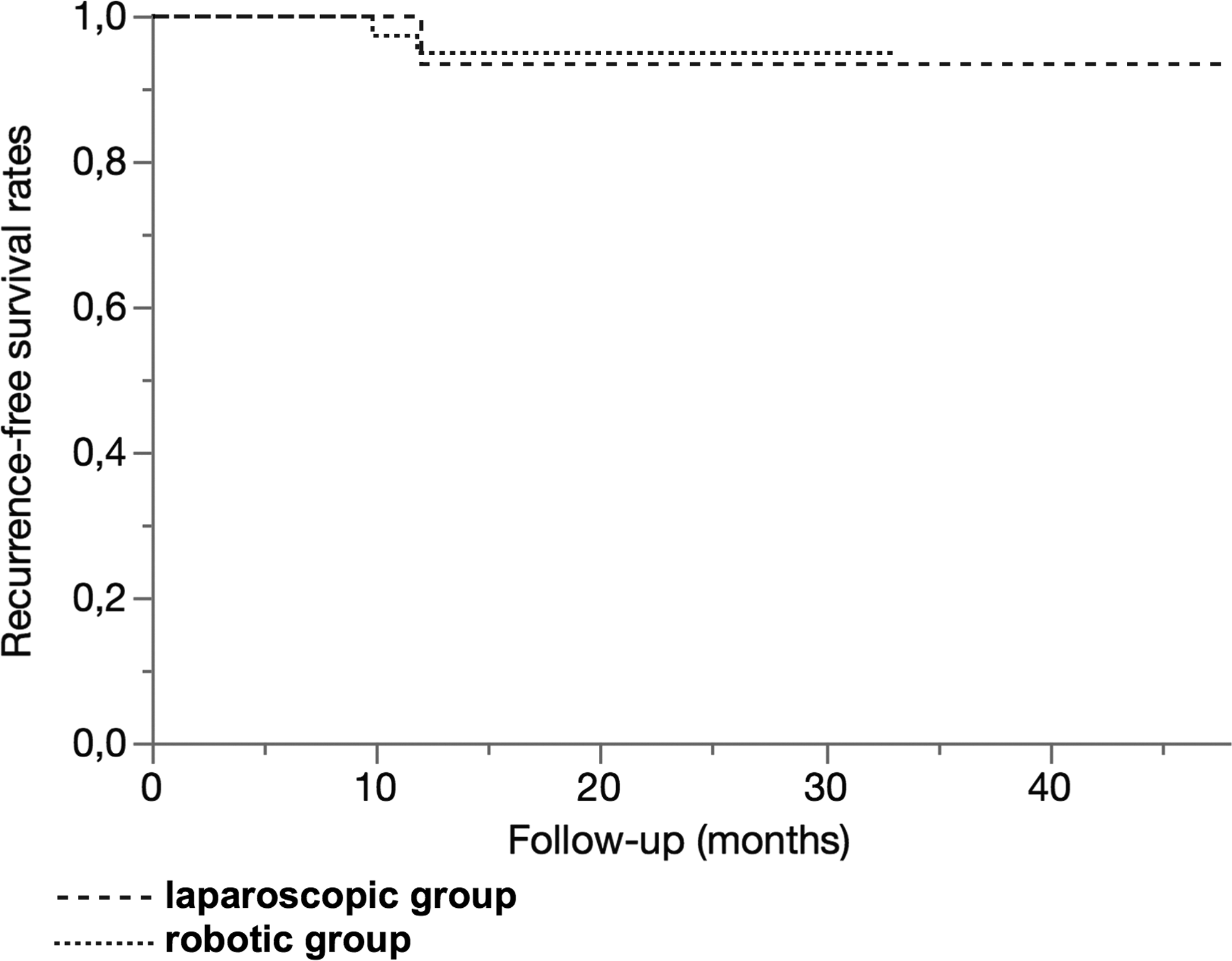
Recurrence-free survival. Log-rank test: P = .89
NA, not applicable.
Discussion
Many studies suggested that RPN is associated with better perioperative outcomes than LPN. Robotic articulated instruments and three-dimensional magnified vision have greatly facilitated renal dissection and repair. Nevertheless, the benefits of RPN over LPN remain controversial. Two well-conducted meta-analyses14,15 comparing LPN with RPN found no difference in terms of OT, conversion rates, EBL, positive surgical margin rate, complications, and length of stay (LoS). The most recent meta-analysis, 16 including 23 articles and 2240 patients, reported lower rates of conversion to RN and open surgery, shorter WIT, and better preservation of renal function in RPN patients. However, these studies were heterogeneous and always included procedures performed during the surgeons' learning curve. Several studies have suggested a long learning curve for LPN with more than 200 cases to decrease complication rates and WIT.17,18 Despite the paucity of data in the literature, the RPN learning curve is usually assumed to be shorter, which could have contributed to its rapid widespread through the urological community.
Our major finding is that the benefit of RPN over LPN might fade away when surgeons have experience in both RPN and LPN techniques. Indeed, in our series, the two approaches yielded similar rates of complication, readmission, positive surgical margins, or conversion to RN. These results suggest that LPN could be a relevant technique in experienced hands. However, PN remains a relatively scarce procedure, and most urologists will not have sufficient volume to reach the level of expertise of laparoscopic surgeons involved in this series. 19 As previously highlighted, LPN might not be recommended in low or moderate volume centers, 20 and selective referral to one specific surgeon should be favored at high volume institution willing to use this technique.
Most outcomes were comparable between LPN and RPN groups. However slight differences favored either RPN (shorter WIT and shorter LoS) or LPN (lower EBL). These differences might not be related to the approach per se but rather to some technical differences between both surgeons and their own clinical pathways. In the LPN group, almost 100% of the patients had a perinephric drain, whereas no patients in the RPN group had postoperative drainage. A perinephric drain has traditionally been left after PN to monitor urinary leakage and/or hemorrhage postoperatively and to prevent urinoma when the collecting system is entered. In their multicentric study, Peyronnet et al. showed that the drain could safely be omitted after RPN, without increasing postoperative complications nor enhancing the risk of urinary fistula. Besides, they showed that systematic drainage did not decrease the use of postoperative CT scan when a complication was suspected, whereas it seemed to prolong hospital stay. 21 Systematic drainage in the LPN group might explain the increased LoS. In our series, LPN was associated with a significantly longer WIT. This result is likely due to the wide use of the early unclamping technique in the RPN group, which has been shown to decrease WIT. The early unclamping technique might also explain the increased blood loss in the RPN group, as suggested in previous series. 13 In the same way, the omission of hemostatic agents in the robotic group may have contributed to shorten WIT, as recently reported in a multicenter series. 22
Several series reported better renal function preservation with RPN than LPN. In our study, although WIT was significantly increased in the LPN group, there was no difference regarding short-term postoperative renal function between the two groups. Recent studies suggested that WIT is not the only determinant of impaired renal function after PN: the amount of renal parenchyma preserved during PN and its quality (i.e., preoperative renal function) are also major contributors of postoperative renal function.23,24 Moreover, current evidence supports that a limited WIT (<25 minutes) will not cause any damage to the operated kidney. 25 The fact that mean WIT remained below the 25 minutes threshold even in the laparoscopic group may explain the lack of difference in renal function preservation between the two approaches. 26
Despite its potential benefits, RPN is associated with higher costs than LPN.27,28 Our analysis did not take into account the financial issue, and our results may suggest the cost-effectiveness of LPN when performed by a highly experienced surgeon. Our results may have overlooked some RPN benefits. In the second center, while tumor complexity and size rapidly increased during the first 30 cases, WIT decrease and TRIFECTA achievement reached a plateau after the first 20 cases. 29 In contrast, the technical challenge of laparoscopy limits its utilization to experienced laparoscopic surgeons. Gill & al described their first 800 LPNs, showing a consequent learning curve of about 500 cases to reach a stability zone in terms of perioperative, oncological, and functional outcomes. 17 In the center 1 experience, the learning curve seems to be shorter with equivalent outcomes after 200 RPN cases. This might be explained by the high experience of the surgeon regarding mini-invasive techniques.
This study has several limitations. First, our findings are limited by the nonrandomized design of the study. Another flaw is the relatively short follow-up, especially in the robotic group, which limits the value of survival analyses. The lack of statistical power inherent to the relatively small sample size prompts to interpret our results with caution, notably all the “not significant differences” (e.g., urinary fistula, conversion to RN, hemorrhagic complications) that may have become significant with larger cohorts. Another important shortcoming is the inappropriate design to evaluate the impact of both techniques on renal function, as no assessment of split renal function was made despite the use of a two-kidney model. 30 Finally, the two groups differed not only regarding the approach used but also regarding several technical aspects that might explain, at least partly, the differences observed. Conversely, no group was competing to demonstrate that one technique was better than another. This study reflects the daily practice in center of expertise.
In this series comparing the experience of LPN and RPN “beyond the learning curve,” perioperative and short-term oncological and functional outcomes appeared to be broadly comparable. We were not able to demonstrate that early unclamping of renal arteries leads to improved functional outcomes when WIT is below 25 minutes. These results suggest that the poorer perioperative outcomes previously reported with LPN may rely mostly on its steep learning curve.
Footnotes
Disclosure Statement
Pr Bensalah and Dr Verhoest are proctors for Da Vinci®.
Dr Alimi, Dr Peyronnet, Dr Khene, Dr Pradère, Pr Sebe, Dr Cote, Dr Kammerer-Jacquet, Dr Mathieu, and Dr Guillonneau have nothing to disclose.