
Abstract
Abstract
Background:
Ileostomy prolapse has a cumulative risk of 11% and represents a significant complication with associated morbidity, which may result in multiple admissions and procedures requiring a general anesthetic. We have developed a laparoscopic technique for managing stoma prolapse—so-called laparoscopic enteropexy for prolapsing stoma (LEPS).
Methods:
Retrospective analysis of a prospectively maintained departmental surgical logbook was performed alongside clinical case history review for patients undergoing LEPS. Primary outcome was defined as recurrent prolapse. Secondary outcomes were any postoperative complication or complication occurring at the time of stoma closure.
Results:
A total of 15 LEPS procedures were performed on 14 patients with stoma prolapse—13 were patients with ileostomy and 1 with a loop colostomy. Median operative time was 75 minutes (range 50–95). Median postoperative stay was 1 day (1–4 days). There was one return to theater for a small bowel intussusception on the second postoperative day wherein taking down of the bowel and repeat LEPS were necessary. There was one recurrence of prolapse in a separate patient (1/14 [7%]). Three patients have since had their stoma closed without complication.
Conclusion:
We describe here the initial case series of our LEPS procedure for managing stoma prolapse. This is a reproducible and technically straightforward laparoscopic procedure with an excellent success rate in preventing further prolapse.
Introduction
I
In 2005, the senior author presented a report of a novel technique to treat stoma prolapse by suturing the loop of the prolapsing stoma to the posterior aspect of the abdominal wall using a minimally invasive technique, the laparoscopic enteropexy for prolapsing stoma (LEPS). 3 We sought to describe our experience and patient outcomes with this technique in the intervening 12 years.
Methods
We performed a retrospective analysis of all cases of laparoscopic fixation of stoma, noting baseline demographics and diagnoses, information about the stoma prolapse before the LEPS procedure, details of the operative procedure, and any complications noted in the subsequent follow-up.
We defined primary outcome as a need for further surgery for prolapse and secondary outcome as any reported form of minor recurrent prolapse not yet requiring any intervention, as well as any complications of the surgery itself—including wound complications.
We were unable to gain surgical operative time for all patients, so used total GA time available from the anesthetic charts as a surrogate for the duration of surgery. We measured postoperative stay to the nearest day—but excluded long term in patients who had surgery for prolapse during a protracted hospital stay. Follow-up duration was defined as the time to the last clinic review in a child with a stoma, or the time to open revision or closure of the stoma in the event of either of these. Continuous variable data were documented as median values with accompanying ranges.
Operative technique
A 5 mm Hasson port is placed using an open technique in the left flank for camera access. Two further 5 mm working ports are placed in the left upper quadrant and left iliac fossa (Fig. 1). The peritoneum at the back of the anterior abdominal wall is opened for 10 cm and the ileum immediately proximal to the stoma is stitched to the exposed fascia of the anterior abdominal wall with interrupted 3-0 Prolene (Fig. 2). Nonabsorbable monofilament is the preferred suture material of the senior author, but we concede that the choice of suture material will rest with the operating surgeon. We do recommend nonabsorbable suture as the senior author had 1 patient in whom this technique was used in open surgery, but prolapse recurred as an absorbable suture material was used. Laparoscopic ports are routinely closed with Vicryl sutures and Indermil™ glue.
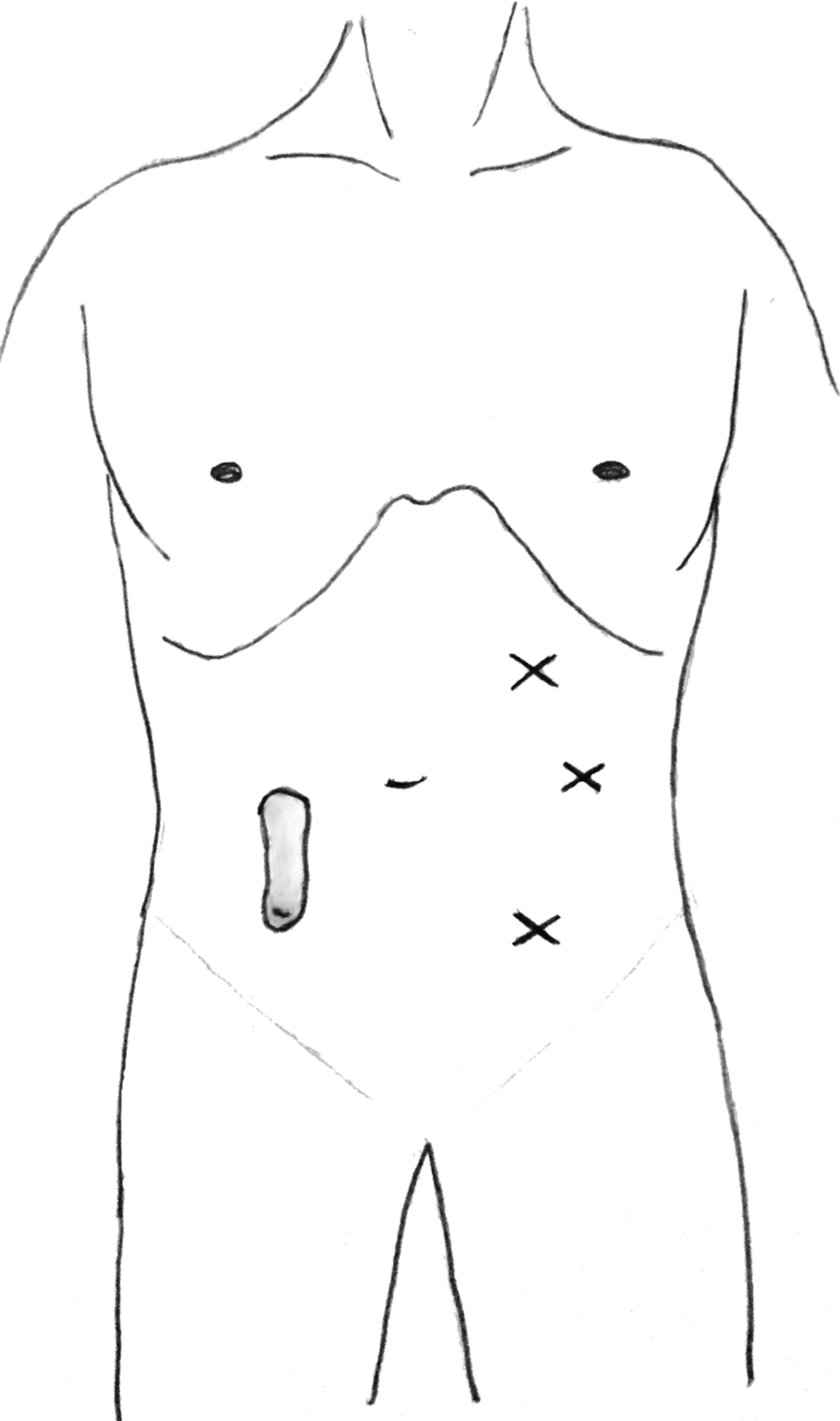
Operative port placement for right-sided ileostomy.
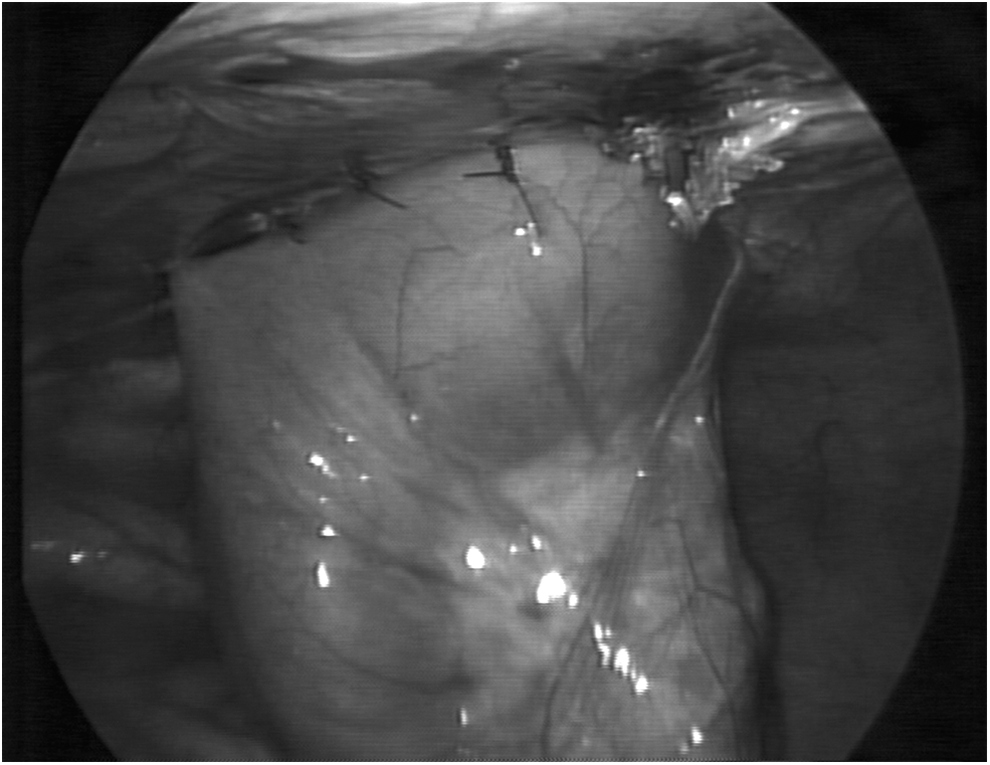
Proximal loop of bowel is sutured to the posterior aspect of the abdominal wall.
Results
We performed 15 procedures on 14 patients. Patients' demographics and details related to the initial stoma, prolapse, and subsequent LEPS procedure are displayed in Table 1. Before the LEPS procedure, all patients had suffered recurrent prolapse of the stoma (defined by more than two episodes with symptoms). Furthermore, 4 of 14 had required a general anesthetic to achieve reduction of a persistent stoma prolapse.
GA, general anesthetic; LEPS, laparoscopic enteropexy for prolapsing stoma.
All but 1 of the patients had an ileostomy, and 1 patient had a colostomy for persistent incontinence post-re-do Duhamel pull-through for long-segment Hirschsprung's Disease with Down Syndrome.
Complications
There was one immediate failure on the 2nd postoperative day. This patient continued to have pain and signs of obstruction and was re-explored. An intussusception was found just proximal to the stoma that was then reduced and the bowel again fixed to the back of the abdominal wall with no subsequent complications, including prolapse.
A second patient had a single episode of stoma prolapse, reduced on the ward on day 163. This stoma was revised on day 175 at the same time as an elective open colectomy.
We had no wound infections and no complications of bleeding. Three patients have had their stoma closed without complication.
Success rate
The success of LEPS at preventing further prolapse was 93%. We report one immediate complication requiring emergent surgery and 1 case of prolapse post-surgery which did not require immediate surgical intervention.
Discussion
Existing management of stoma prolapse for the most part involves simple manual reduction with adequate pain control. More recently the use of osmotic agents has been widely adopted for reduction of edema to facilitate manual reduction.4–6 Failure to achieve this in an awake or sedated patient indicates a general anesthetic to ensure complete reduction. If reduction under anesthetic is not possible, surgical exploration and revision may be required, which may involve bowel resection. 7
Various strategies have been suggested for the surgical management of patients suffering from recurrent reducible prolapse. Several groups have described resection of the redundant bowel and resiting of the stoma, often using a linear stapling device.8,9 However, this strategy has only been reported in adult patients, whereas preservation of bowel length is a major consideration in young children. More complex techniques have been employed in adults, such as extraperitonealization of the prolapsing loop and plication of the loops of intestine immediately proximal to the stoma. 10 Such techniques require a major laparotomy, made technically more challenging by the size of the patient (the median age of our cohort was 4.7 years at the time of LEPS).
This case series represents, to the authors' knowledge, the first describing a success rate of a procedure for ileostomy prolapse, and is also the only series describing outcomes in an exclusively pediatric cohort. There are several individual case reports describing novel techniques for managing prolapse,10,11 however, previously reported series describe techniques used as a revision strategy for a variety of complications and do not describe specific outcomes for prolapse.9,12,13 A recently published systematic review acknowledges very scarce literature in the pediatric age group referring to surgery for stoma prolapse. The author of this review notes that in other surgical procedures that avoid laparotomy, recurrence approaches 50%. 14
Prolapse is known to correlate with poor quality of life outcomes in patients with a long-term stoma, 15 with patients demonstrating reduction in both physical and mental component scores of the generalized quality-of-life questionnaire SF-36, 16 as well as a significantly lower scores when assessed with gastrointestinal quality of life index. 17 We note from this select series that prolapse in this group of children happens relatively early after initial stoma formation and this may prompt the attending surgeon to consider surgery, addressing the issue early in the patient journey.
Young patients with severe gastrointestinal dysmotility often have markedly disrupted education and social development, because of frequent and lengthy admissions with uncontrolled symptoms. 18 This group is also thought to be more susceptible to stoma prolapse. 19 Reducing the incidence of mechanical issues with stomata in this population serves to maximize their time at home and school, which must be a priority in the holistic management of such children.
The LEPS technique is technically straightforward for a surgeon with a moderate to high level of laparoscopic ability. The domain of the abdomen is preserved and most children may be discharged within 24–36 hours postoperatively. There have been 2 other individual published cases wherein our technique has been used; the authors from the first center in 2013, described this technique to manage a loop colostomy prolapse. 20 The authors from a second institution elected to suture the small bowel mesentry as opposed to the bowel itself—citing a possible risk of fistula formation. 21 We have not seen this complication in our series. Neither of these reported cases note any postoperative complication.
One potential difficulty we have envisaged with this technique is the mobilization of the afferent bowel when reversing the stoma. We have been careful in our operative documentation to make note of the direction in which the bowel has been fixed to the abdominal wall. It has been possible to complete stoma closure in the 3 cases in this series without complication based on this knowledge.
There are limitations that are inherent of a study of this kind. Clearly, presenting descriptive data as a case series, we are unable to deliver a recommendation of our technique over another strategy. The nature of retrospective data means that follow-up is nonuniform, and although some of our patients have been seen in the clinic for >5 years, others are still in the early postoperative months. We believe laparoscopic fixation would certainly produce lower morbidity than larger incisions associated with local revision or a procedure requiring a laparotomy. This approach is now the authors' first choice method to manage prolapse and we feel that it is straightforward and reproducible by any experienced laparoscopist.
Footnotes
Disclosure Statement
No competing financial interests exist.