
Abstract
Abstract
Introduction:
Nissen fundoplication is frequently applied in the surgical treatment of patients with gastroesophageal reflux disease (GERD). When the gastroesophageal junction remains too large or becomes too narrow, persistent GERD or dysphagia may occur. To assure a correct size of the gastroesophageal junction, the fundoplication can be created over a bougie. However, this increases the risk of esophageal perforation. Therefore, we have modified a previously described technique to create a standardized fundoplication without the use of a bougie. In this article, we describe this technique and demonstrate the initial results.
Materials and Methods:
We describe a technique to create a standardized Nissen fundoplication. After suture repair of the hiatal hernia, three marking sutures were placed on the gastric fundus, based on an equilateral triangle. The size of this triangle determines the final diameter of the fundoplication. With these measurements, we assure sufficient patency, minimize rotation, and create a more reproducible fundoplication that may reduce postoperative dysphagia.
Results:
We have operated 15 patients according to this technique. Mean operative time was 69.5 (SD 8.4) minutes, no complications occurred. There was no early dysphagia and the mean length of stay was 1.3 days (1–2). Quality of life after 1 year was excellent.
Conclusions:
This modified method for standardized Nissen fundoplication is safe and might reduce postoperative dysphagia. Quality of life after 1 year is excellent. The effect on postoperative dysphagia and the reproducibility of this technique should be established in a large prospective study.
Introduction
G
Therefore, we have developed a modification to the current technique for Nissen fundoplication to create a standardized and reproducible wrap without the use of a bougie. With this technique, we try to assure sufficient patency and to minimize the risk of damage to the esophagus. This technique may minimize postoperative dysphagia. The aim of this study is to investigate whether this technique is feasible, safe, and does not lead to a significant increased operating time.
Materials and Methods
Study design
Based on previously published studies, we know that an esophagus with a 60Fr bougie in place has an outside diameter of ∼2.7 cm. 16 For this study, we used the measurements described by Reardon et al. 16 To create a “floppy” fundoplication, they added another 1.0 cm to this diameter, resulting in a fundoplication with an ideal inside diameter of 3.70 cm. According to the mathematical equation circumference (c) = π × diameter (d), this results in a circumference of 11.6 cm, rounded up to 12.0 cm (Fig. 1).
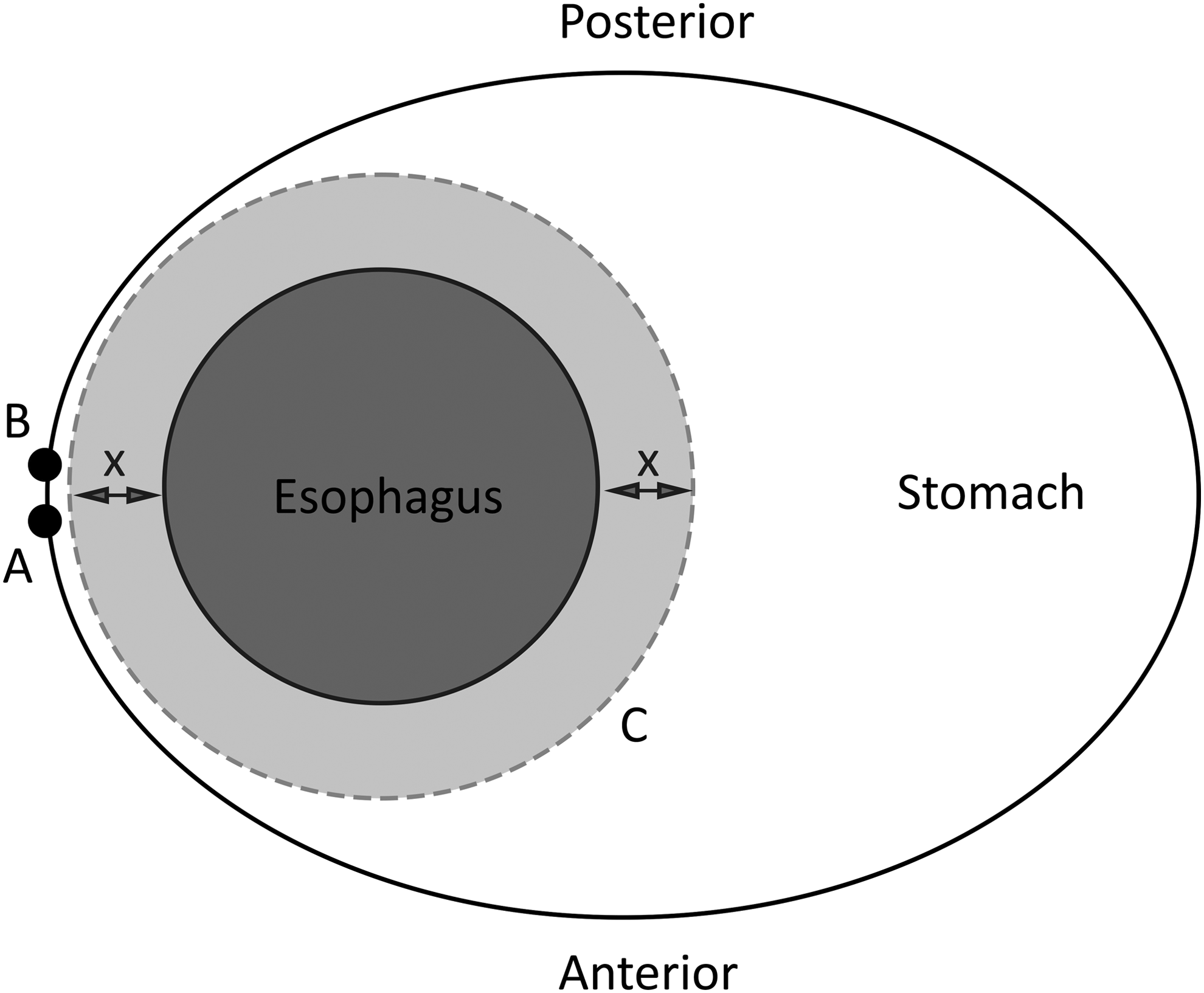
Schematic overview of the calculated distances for the modified technique. A = point A, on the anterior side of the stomach wall; B = point B, on the posterior side of the stomach wall; C = circumference of fundoplication, represented by dotted line; X = distance between outside of esophagus and the fundoplication, 0.5 cm on each side.
To create a fundoplication without any rotation, both point A (anterior side of the stomach) and point B (posterior side of the stomach) need to be determined. The great curvature should be in the center between these two points to prevent rotation of the fundoplication (Fig. 2). Measurements to locate these two points are depicted in Figure 3. Subsequently points A and B are brought together behind the esophagus and a “shoeshine” movement is performed to prevent rotation of the wrap. Then the fundoplication is completed by placing three nonabsorbable braided sutures (Ti-Cron™; Covidien, a Medtronic Company, New Haven, CT).

Overview of both points A and B in relation to the short gastric vessels, demonstrating the symmetry of the fundoplication. A = point A on the stomach wall; B = point B on the stomach wall; red dotted line = the short gastric vessels; His = the angle of His, the junction between the greater curvature and the esophagus.

Anterior view the measurements taken during surgery. His = angle of His; A = point A on the anterior wall of the stomach; red lines = short gastric vessels.
Patient selection
For this modified technique, we retrospectively evaluated the first 15 consecutive patients who have been operated according to this modified technique. All patients were diagnosed with GERD according to the SAGES guideline for GERD. Minimal age was 18 years and patients were not selected for this evaluation if they have had prior antireflux surgery.
Outcome measurements
To evaluate postoperative quality of life, all patients were sent a questionnaire by mail. Nonresponders were contacted up to three times by phone to optimize response rate.
Primary outcome of this study was the safety of this procedure, and therefore the complication rate. Secondary outcomes were time of surgery, length of stay, postoperative dysphagia, and short-term quality of life measured by the GERD-HRQL questionnaire.
Operative technique
The entire procedure was performed laparoscopically with patients in a supine position and under general anesthesia with the surgeon positioned between the legs. Pneumoperitoneum was obtained using a Veress needle technique typically at Palmers point. Our preference, for safety reasons, was to place the first trocar under direct vision. We, therefore, used a 12 mm Visiport (Visiport™; Medtronic, North Haven, CT) in the supra umbilical position. After inspection for adhesions and/or other abnormalities, two 5 mm trocars and one 8 mm trocars were inserted. Then the liver retractor was placed in position to create enough space to perform the procedure.
The procedure starts with opening the lesser omentum and phrenoesophageal ligament, followed by dissection of the right and left limbs of the crus of the diaphragm. Then the short gastric vessels were divided using an ultrasonic device (Harmonic ace®; Ethicon, US).
The next step was to create a window behind the esophagus and encircle the esophagus with a silicone tube to retract the esophagus without damage. At least 3 cm of the esophagus was dissected and has to lay tension free in the abdomen. The hernia sac was brought back into the abdomen and if a hiatal hernia was present, this was narrowed with braided sutures (Ti-Cron; Covidien, a Medtronic Company).
We pursued patency for a 10 mm instrument to pass besides the esophagus. If a large hiatal hernia was present or in case of weakness of the crus, the cruroplasty was reinforced with a synthetic nonabsorbable mesh (Parietex™ Composite Mesh Hiatal; Sofradim, a Medtronic Company, Trevoux, France).
A large hiatal hernia is defined as migration of >50% of the stomach into the thorax. 17
We measured 6 cm from the angle of His along the great curvature using the grasper, which has a length of 2.5 cm, and placed a marking suture. From this point, we created an equilateral triangle with sides of 6 cm (Fig. 2). We placed a second marking suture on the anterior side of the stomach. The next step was to flip the stomach anteriorly and perform the same maneuver on the posterior side of the stomach and place a third marking suture. All marking sutures were braided absorbable sutures (Polysorb™; Covidien, a Medtronic Company). To facilitate the mobilization of the stomach, the suture at the posterior side was kept a little longer. Then the silicone was removed and using a grasper the posterior suture was grabbed behind the esophagus. A “shoeshine” movement was performed to make sure that there was no rotation. The surgeon brought the posterior suture together with the anterior suture and the assistant held them in place. Then the procedure was completed by placing three braided sutures (Ti-Cron; Covidien, a Medtronic Company) to fixate the fundoplication. The most distal suture was attached to the esophagus to prevent telescoping. A video of the complete procedure can be found in the Supplementary Video S1 (Supplementary Data are available online at www.liebertpub.com/lap).
Ethics
Since it concerns the routine implementation of a modification of a previously described technique that is now routinely applied in our institution, informed consent was waived.
Results
Patient characteristics
A total of 15 patients were operated according to this technique between March 2015 and January 2016. Mean age during surgery was 53.4 (SD 11.8) years, 9 (60%) of the patients were male, and the mean body mass index was 26.5 (SD 3.7) kg/m2. A total of 93.3% of the operated patients experienced preoperative heartburn, 26.7% of the patients experienced regurgitation, and dysphagia was present in 20% of the patients. A complete overview of the baseline characteristics for all patients is presented in Table 1.
ASA, The American Society of Anesthesiology classification of physical status; PPI, proton pump inhibitor; SD, standard deviation.
All patients were diagnosed according to the SAGES guideline for GERD. An overview of the preoperative work-up is demonstrated in Table 2.
Operative results
All patients underwent a primary laparoscopic Nissen fundoplication. Mean operative time was 69.5 (SD 8.4) minutes. We experienced no operative complications and there were no conversions to an open procedure. There were no reoperations during follow-up. Details regarding the procedures are summarized in Table 3.
LOS, length of stay; SD, standard deviation.
Postoperative results
Postoperative stay at the hospital was 1 or 2 days. No postoperative complications were seen and only 1 patient was readmitted within the first 30 days. The reason for readmission was general illness with fever. This appeared to be due to a urinary tract infection. The patient was treated with antibiotics and the patient was discharged after 3 days.
Quality of life
A total of 9 patients (60%) returned the quality-of-life questionnaire. This resulted in a median quality of life after 1 year of 69 out of a maximum score of 75 (range 36–75). The median heartburn score was 30, with a maximum score of 30. Postoperative proton pump inhibitor usage was 44.4%.
Discussion
In this article, we present a modified technique to create a floppy Nissen fundoplication without the use of a bougie. The aim of this modification was to create a standardized and reproducible fundoplication without the risks that come with the use of a bougie and that is better teachable to surgeons in training. Theoretically, this technique might reduce postoperative dysphagia without increasing the rate of recurrent heartburn compared with the standard technique.
Based on current literature we have found an incidence of early dysphagia up to 76%. 5 A retrospective study performed by Lamb et al. investigates the results of revision surgery after prior antireflux surgery for GERD. 18 This study demonstrates that persistent dysphagia is the most reported indication for revision surgery (52%). We also know from literature that patients who experience postoperative dysphagia report suboptimal outcomes after revision surgery.19–21 It is, therefore, important to reduce the risk of postoperative dysphagia and minimize the chance for revision surgery.
Our hypothesis is that postoperative dysphagia may be, among other causes, the result of both a too tight fundoplication and some sort of rotation in the wrap. A too tight wrap as a cause of postoperative dysphagia has been investigated previously. 22 However, there is no consensus regarding the ideal diameter of the fundoplication and it is hard to feel the correct tightness of the wrap. Some authors, therefore, advocate the use of a bougie to assure sufficient patency.11,12 Nevertheless, different bougie sizes have been used that vary between 52Fr and 60Fr, but the optimal size is yet to be found. The positive effect of a bougie on postoperative dysphagia was already demonstrated by Demeester et al. in 1986. 23 This study showed a significant decrease in postoperative dysphagia for a 60Fr bougie compared with a 36Fr bougie, especially in the first 3 postoperative months. The use of a bougie comes, however, with the severe risk of esophageal perforation, which comes with serious morbidity and even mortality. 15 Despite these possible serious complications, an anonymous survey performed in 2005 by Huttl et al. in Germany showed that still 46% of the surgeons still routinely used a bougie during laparoscopic Nissen fundoplication at that time. 24 A possible explanation might be that it is difficult, especially for the inexperienced surgeon, to create a proper fundoplication with a correct diameter. This hypothesis is supported by historical studies, which demonstrates a learning curve of ∼25 procedures per surgeon.25–27 These studies also show a prior complication rate of 24%–55%, which decreases to ∼10% when more experience is obtained. By this modified technique, we aim to aid surgeons who start performing laparoscopic Nissen fundoplication and to create a standard fundoplication that ensures sufficient patency. Further research is needed to investigate whether this technique indeed reduces the learning curve and reduces long-term dysphagia.
According to published literature, we believe that a common error made by surgeons is to create an asymmetrical fundoplication, resulting in a “twist” in the fundoplication.16,28 With the already mentioned technique, we assured that the fundoplication that is created is as symmetrical as possible. This leads to a reduced risk of shifting the line of the greater curvature to either anteriorly or posteriorly (Fig. 2).
In this report, we demonstrate the first 15 patients who have been operated according to this modified technique. We are aware of the fact that this is a very small group and follow-up is short and only 60% returned the quality-of-life questionnaire. However, we did not see any perioperative complications, only 1 patient was admitted for a urinary tract infection on postoperative day 3. This is a minor complication and in our opinion not related to the modified technique.
Since the measurement of the exact points A and B does take some extra time, we compared the operative time with our retrospective cohort of the past 10 years. The mean operative time in this cohort was 78.8 (SD 39.2) minutes, 29 where the mean operative time for this modified technique was 69.5 (SD 8.4) minutes (P = .752). There is no statistically significant difference between both techniques in operating time. However, we do expect that especially inexperienced surgeons will benefit from this modified technique, which might even result in an even faster operating time. This hypothesis will be subject of further research.
Conclusion
The size of the gastric wrap, created during a Nissen fundoplication, can be standardized using an atraumatic and minimal invasive approach. This modified technique is safe with no early postoperative complications and good results at 1 year follow-up. The possible advantage regarding reproducibility, reduced learning curve, and less postoperative dysphagia is yet to be established in further studies.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.